Article Text

Abstract
OBJECTIVE To assess resting and exercise echocardiography for prediction of left ventricular dysfunction in patients with significant asymptomatic aortic regurgitation.
DESIGN Cohort study of patients with aortic regurgitation.
SETTING Tertiary referral centre specialising in valvar surgery.
PATIENTS 61 patients (38 men, 23 women; mean (SD) age 53 (14) years) with asymptomatic or minimally symptomatic aortic regurgitation and no known coronary artery disease; 35 were treated medically and 26 had aortic valve replacement.
INTERVENTIONS Exercise echocardiography was used to evaluate ejection fraction, which was measured on the resting and post-stress images using the modified Simpson method. Patients with an increment of ejection fraction after exercise were denoted as having contractile reserve (CR+); those without an increment were labelled CR−.
MAIN OUTCOME MEASURES Standard univariate and multivariate methods and receiver operating characteristic analyses were used to assess the ability of contractile reserve to predict follow up ejection fraction.
RESULTS In the 35 medically treated patients, 13 of 21 (62%) with CR+ (mean (SD) ejection fraction increment 7 (3)%) had preserved ejection fraction on follow up. In the 14 patients with CR− (ejection fraction decrement 8 (4)%), 13 (93%) had a decrement of ejection fraction on follow up from 60 (5)% at baseline to 54 (3)% on follow up (p = 0.005). Age, resting left ventricular dimensions, medical treatment, aortic regurgitation severity, exercise capacity, and rate–pressure product were similar in both CR+ and CR− groups. Among the 26 surgical patients, 13 showed CR+ (ejection fraction increase 9 (5)%), all of whom had an increase in ejection fraction on follow up (from 49% to 59%). Of 13 surgical patients with CR− (ejection fraction decrease 7 (5)%), 10 (77%) showed the same or worse ejection fraction on postoperative follow up.
CONCLUSIONS Contractile reserve on exercise echocardiography is a better predictor of left ventricular decompensation than resting indices in asymptomatic patients with aortic regurgitation. In patients undergoing aortic valve replacement, contractile reserve had a better correlation with resting ejection fraction on postoperative follow up. Measurement of contractile reserve may be useful to monitor the early development of myocardial dysfunction in asymptomatic patients with aortic regurgitation, and may help to optimise the timing of surgery.
- aortic regurgitation
- contractile reserve
- exercise testing
- ejection fraction
Statistics from Altmetric.com
Volume overload from aortic regurgitation is usually well tolerated by the left ventricle early in the course of the disease. The development of symptoms occurs later and implies left ventricular decompensation.1 ,2 Aortic valve replacement is commonly recommended while the patient is still asymptomatic, but selection of the optimum time for surgery may be difficult. Although early surgery has been proposed,3 ,4 valve replacement carries a 1–3% operative mortality and the ongoing risks of a prosthetic valve warrant consideration as aortic valve repair is rarely feasible. However, left ventricular function is a major determinant of long term prognosis,3 and excessive delay before surgery can result in compromised long term survival owing to significant myocardial damage and the development of left ventricular dysfunction.4-6 The ability to predict left ventricular dysfunction during follow up could have important implications for the timing of intervention.7
Several studies have examined the outcome of medical and surgical treatment in patients with aortic regurgitation, most of which have focused on symptomatic patients with overt left ventricular dysfunction.5 ,8 ,9 The presence of preoperative left ventricular dysfunction (left ventricular systolic dimension > 55 mm and fractional shortening < 25%) is significantly related to the risk of the developing chronic heart failure and to mortality.5 Other criteria involving left ventricular dimensions and resting indices of left ventricular function have been shown to predict outcome,5 ,10-12 but various investigators have argued that these are either too restrictive or too liberal,13-15 and the guidelines for intervention in asymptomatic patients are not universally accepted.
Previous work with radionuclide ventriculography has shown that the ejection fraction during exercise and the change from rest to stress to be abnormal in many patients with aortic regurgitation,16-18 and these data may be predictive of outcome.18 Echocardiography is a more widely available technique, and exercise echocardiographic measurement of ejection fraction and end systolic volume has been shown to predict outcome in patients with mitral regurgitation.19 However, there are limited data to support its use in aortic regurgitation,20and in the most recent guidelines for the management of patients with valvar heart disease21 this technique was given a class III indication (evidence or general agreement that the procedure is not useful). In this study, we sought to determine whether exercise echocardiography might be used to predict left ventricular dysfunction during follow up of patients with significant asymptomatic aortic regurgitation.
Methods
STUDY PATIENTS
We prospectively studied 61 patients (38 men, 23 women; mean (SD) age 53 (14) years) with asymptomatic or minimally symptomatic severe aortic regurgitation. These patients were selected from a larger population referred to the Cleveland Clinic Foundation for evaluation of chronic aortic regurgitation and potential valve surgery. From this larger group, those with clear indications for valve replacement proceeded to surgery. These patients had symptoms (mainly exercise intolerance), severe left ventricular enlargement (left ventricular systolic dimension > 55 mm or volume > 60 ml/m2), or left ventricular dysfunction (ejection fraction < 50%).21 The remaining patients with severe aortic regurgitation (grade 3/4 or 4/4) in the absence of symptoms or echocardiographic indications for intervention were recruited into the study.
Patients with previous cardiac surgery, coexisting mitral valve disease, more than mild aortic stenosis, and suboptimal images were excluded. Patients with a history of angina, previous acute myocardial infarction, coronary artery bypass grafting, or known coronary artery disease on angiography were excluded, in order to minimise additional factors that may affect left ventricular function. Although images were of variable quality, no patient was excluded because of suboptimal images.
The aetiology of aortic regurgitation included congenital bicuspid aortic valve, rheumatic valvar disease, sclerodegenerative disease, and aortic annular dilatation.
BASELINE RESTING AND EXERCISE ECHOCARDIOGRAPHY
All patients underwent transthoracic echocardiography in the left lateral decubitus position at rest and immediately after exercise. Imaging was performed with standard commercially available equipment and digitised on-line into a quad screen, cineloop format (ImageVue, Kodak Health Imaging, Allendale, New Jersey, USA). Images were also recorded on half inch VHS videotape. Resting left ventricular end diastolic and end systolic dimensions and the thickness of the interventricular septum and posterior wall were measured. The severity of the aortic regurgitation was assessed semiquantitatively by colour and continuous wave Doppler by expert echocardiographers independent of the investigators, using a combination of colour jet dimensions, pressure half time, and aortic flow reversal.22-24 Left ventricular end diastolic and end systolic volumes were measured from the apical four chamber view, by an experienced observer using the modified Simpson rule. Only representative cycles were measured and the average of three measurements was taken. The endocardial border was traced, excluding the papillary muscles. The frame captured at the R wave of the ECG was considered to be the end diastolic frame, and the frame with the smallest left ventricular cavity, the end systolic frame. Ejection fraction was calculated from the difference between the end diastolic and end systolic volumes, at rest and immediately after exercise. The difference between the resting and postexercise ejection fraction was defined as the contractile reserve (CR). Patients with an augmentation of ejection fraction with exercise were designated as having contractile reserve (CR+), and those failing to augment were identified as CR−.
We have previously shown a mean (SD) intraobserver variability for the recording of resting ejection fraction of 2 (4)%, and of left ventricular end diastolic and end systolic volumes of 5 (10) ml (r = 0.97) and 1 (4) ml (r = 0.99), respectively. After exercise, the respective variabilities were 1 (2)%, 1 (10) ml (r = 0.98), and 1 (3) ml (r = 0.99). Values for interobserver variability were comparable.19
The 12 lead ECG was performed, using conventional chest lead positioning, before exercise, at the conclusion of each stage, and after stress. Symptom limited treadmill exercise testing was performed in all patients, using a protocol selected according to the cardiovascular and overall physical state of each subject (Bruce, modified Bruce, or Naughton). Blood pressure and the physical signs were monitored during exercise testing in the usual fashion, and the conventional end points for exercise testing were applied.25 Peak heart rate, blood pressure, rate–pressure product, and estimated exercise capacity were recorded for all patients. All but five patients in the medically treated group achieved 85% of their age predicted maximum heart rate with exercise.
FOLLOW UP
Thirty five patients (19 men, 16 women; mean (SD) age 51 (15) years) proceeded with medical treatment selected by the physician caring for the patient; these included 28 patients (80%) in functional class I and seven (20%) in functional class II at the time of inclusion into the study.
The surgical group comprised 26 patients with significant aortic regurgitation who underwent aortic valve replacement within 3 (2) months of their exercise stress test. This clinical decision was made by the treating physician, based on progression of the disease and independent of the study. In most patients this reflected the interim development of symptoms, but included increasing left ventricular systolic dimension (to > 55 mm) and volume (to > 60 ml/m2), and falling ejection fraction (to < 50%) on serial studies.21
A resting transthoracic echocardiogram was repeated and recorded (as described for the baseline study) at the end of the follow up period. The follow up ejection fraction was compared with their baseline ejection fraction in order to identify any change in left ventricular function.
STATISTICAL ANALYSIS
In both the medically treated group and the patients undergoing an aortic valve replacement, the results were examined in two different analyses. First, according to the change in ejection fraction induced by exercise, patients were grouped as those with preserved or impaired contractile reserve. Second, comparing their follow up ejection fraction with that at baseline, patients were grouped as those in whom the ejection fraction had decreased or remained steady/improved when compared with baseline. Results are expressed as mean (SD) unless stated otherwise. The χ2 test was used to compare categorical variables and the paired or unpaired Studentt test to compare continuous variables. Spearman's correlation coefficient was used to estimate the correlation between continuous variables. Multiple linear regression models were developed to examine the independent predictors of global left ventricular function over follow up. Receiver operating characteristic (ROC) curves were used to evaluate various levels of contractile reserve for the prediction of left ventricular function over follow up. Significance was defined as a value of p < 0.05.
Results
CLINICAL CHARACTERISTICS
Table 1 summarises the clinical characteristics of medically and surgically treated patients, subdivided into those with and those without contractile reserve. Patients were not systematically given medical treatment; any treatments given were based on the presence of symptoms. Those undergoing valve replacement had more severe aortic regurgitation but were otherwise comparable to those treated medically.
Clinical characteristics of patients with (CR+) and without (CR−) contractile reserve. No significant differences were present between CR+ and CR− groups
In the medically treated group, 21 of the 35 patients in the study (60%) increased their ejection fraction with exercise, signifying intact contractile reserve (CR+), whereas 14 (40%) lacked contractile reserve (CR−; decrease or no change in their ejection fraction). In the patients undergoing aortic valve replacement, the contractile reserve was preserved in 13 (50%) of the 26 patients and lacking in the other half of the group. Patients with and without contractile reserve were comparable on clinical grounds.
BASELINE ECHOCARDIOGRAPHY
The resting and exercise left ventricular dimensions and exercise responses of medically treated patients with and without contractile reserve are listed in table 2A, and equivalent data for those who underwent aortic valve replacement are given in table 2B. Patients with contractile reserve were characterised by a reduction in end systolic volume, which produced an increment of the ejection fraction. Patients in the CR+ subset showed a 9% decrease in end diastolic volume in both the medical and surgical groups. This was similar to a 10% decrease in the end diastolic volume both medical and surgical groups in the CR− subset (NS). However, the end systolic volume in the CR+ subset decreased by 23% and 24% in the medical and surgical groups, respectively, whereas there was a 9% and 4%increase in the end systolic volume in the respective medical and surgical subsets of the CR− patients (both p < 0.0001). Thus the postexercise ejection fraction increased by 7 (3)% and 9 (2)% in the medical and surgical CR+ subsets, whereas the CR− subset had an 8 (3)% and a 7 (2)% decrease in medical and surgical patients (p = 0.001). All other aspects of exercise characteristics were comparable in the two groups; specifically, there were no significant differences in exercise capacity or conventional indices of left ventricular function.
Rest and exercise measurements in patients with (CR+) and without (CR−) contractile reserve)
FOLLOW UP OF PATIENTS ON MEDICAL TREATMENT
None of the medically treated patients developed a significant change in functional status or underwent surgery during the mean follow up period of 15 (7) months. On follow up cross sectional echocardiography, there were 14 patients (40%) whose ejection fraction was unchanged from the baseline and 21 (60%) who showed a deterioration. Latent left ventricular dysfunction was identified retrospectively by the finding of a reduction in resting ejection fraction on follow up compared with baseline function.
The baseline clinical and exercise characteristics and resting left ventricular dimensions were comparable in patients with and without a change of ejection fraction on follow up (table 3). However, the contractile reserve at baseline correlated with the change in ejection fraction on follow up (fig 1A). When the contractile reserve on exercise was examined as a categorical variable to predict a change in the ejection fraction (table 4), of the 21 patients with a positive contractile reserve at baseline, 13 had a preserved ejection fraction at follow up. On the other hand, of the 14 patients with a negative contractile reserve on exercise at baseline, 13 showed a significant decrease in ejection fraction on follow up (χ2 = 10.5, p = 0.001).
Baseline characteristics of groups with maintained or increased (ΔEF+) and decreased (ΔEF−) ejection fraction on follow up on medical treatment

Correlation of contractile reserve with change of ejection fraction (EF) over follow up in patients treated medically (A) or with valve replacement (B).
Relation between change in ejection fraction on follow up on medical treatment and contractile reserve at baseline
These changes in ejection fraction were unrelated to changes in end diastolic volume with exercise; patients who maintained their ejection fraction on follow up showed a 17 cm3 (9%) decrease in the mean end diastolic volume, similar to a 12 cm3 (9%) decrease in the group with the latent left ventricular dysfunction (NS). However, the postexercise end systolic volume in the maintained ejection fraction group decreased by 23% compared with a 2% increase in end systolic volume in the latent left ventricular dysfunction group (p < 0.01). The group with maintained ejection fraction had a positive contractile reserve of 7 (4)% with exercise at baseline, while the group with the latent left ventricular dysfunction had a negative contractile reserve of −3 (8)% with exercise at baseline (p < 0.001).
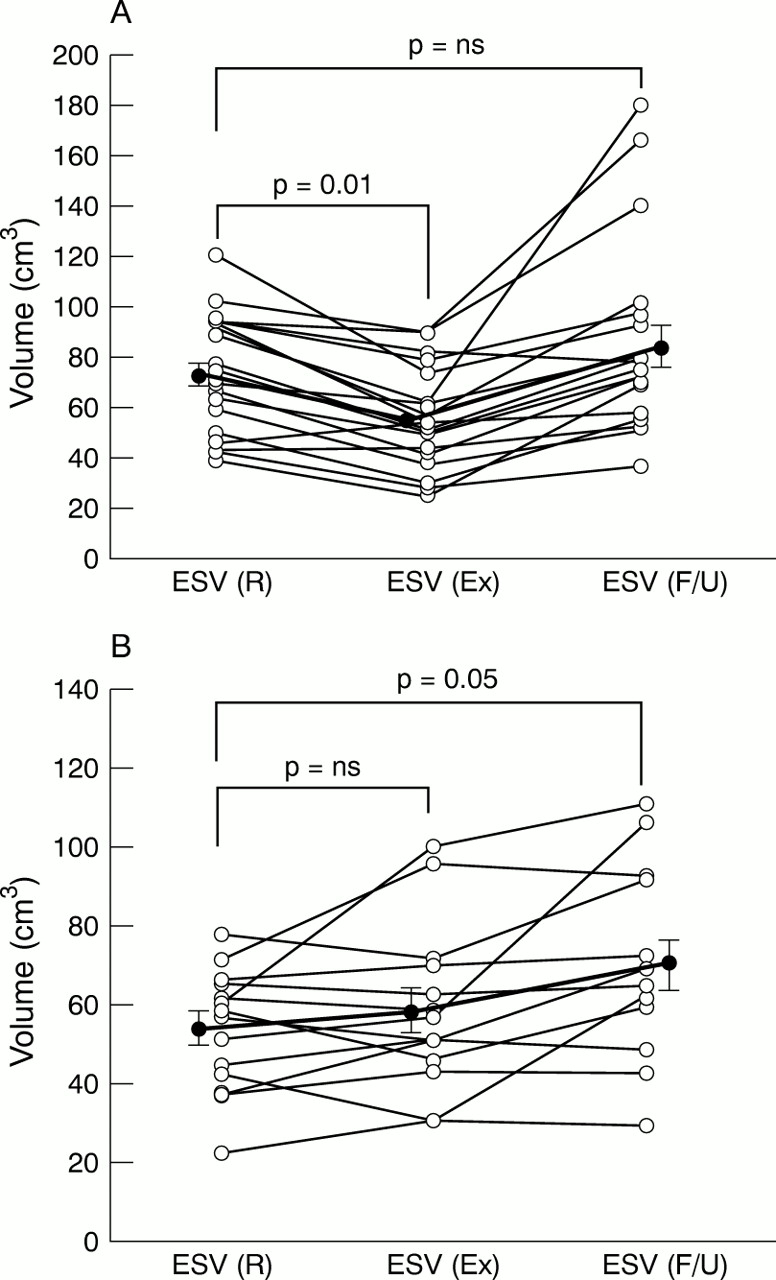
Figure 2 shows the responses of end systolic volume to exercise and follow up in individual patients. Patients with maintained ejection fraction on follow up (fig 2A) showed a significant decrease in the mean end systolic volume with exercise at the baseline study. No difference in the resting end systolic volume at baseline and follow up was observed, suggesting well preserved left ventricular systolic function. On the other hand, patients whose ejection fraction deteriorated during follow up (fig 2B) showed no augmentation in their end systolic volume with exercise, and had a significant increase in their resting end systolic volume on follow up.

Change in left ventricular end systolic volume (ESV) with exercise (Ex) and on follow up (F/U) compared with baseline at rest (R), in patients with maintained left ventricular function (A) and latent dysfunction (B).
Figure 3A compares the accuracy of change in end systolic volume with exercise and the contractile reserve for prediction of the change in ejection fraction on follow up in medically treated patients. Contractile reserve was slightly more sensitive (64%) compared with change in end systolic volume (43%). Both had a similar high specificity of 93%. Thus contractile reserve had a marginally better accuracy (74% v 64%) for predicting preserved left ventricular function than change in end systolic volume alone with exercise (NS). The ROC curve in fig 4A shows the sensitivity and specificity of contractile reserve for predicting change in left ventricular ejection fraction on follow up. At the optimal cut off (contractile reserve 4%), the sensitivity and specificity of predicting subsequent left ventricular dysfunction were both 77%.

Accuracy of contractile reserve (CR) and change in end systolic volume (▵ESV) with exercise as predictors of follow up ejection fraction, in patients followed up on medical treatment (A) and undergoing an aortic valve replacement (B).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Receiver operating characteristic curves relating levels of contractile reserve to sensitivity and specificity for predicting left ventricular dysfunction at follow up in patients treated medically (A) and with valve replacement (B).
FOLLOW UP OF PATIENTS UNDERGOING AORTIC VALVE REPLACEMENT
Patients undergoing aortic valve replacement were reassessed by transthoracic echocardiography after a mean follow up of 6 (8) months. Sixteen patients (62%) showed an improvement of ejection fraction and 10 patients (38%) showed a reduction of ejection fraction after surgery. There were no significant differences in the baseline clinical and exercise characteristics or in resting left ventricular dimensions in patients with and without a change of ejection fraction on follow up (table 5).
Baseline characteristics of groups with maintained or increased (ΔEF+) and decreased (ΔEF−) ejection fraction on follow up after aortic valve replacement
Changes in ejection fraction during follow up in patients who underwent valve surgery were unrelated to changes of end diastolic volume with exercise; patients with both improved and worsening ejection fraction on follow up showed 9% decrease in the mean end diastolic volume after exercise. Results for end systolic volume were different; patients with improved ejection fraction had a 19% decrease in end systolic volume compared with a 4% increase in the group with a worsening ejection fraction (p < 0.01). The group with the improved ejection fraction had a positive contractile reserve of 6 (2)% with exercise at baseline, while the group with the worsening ejection fraction after surgery had a negative contractile reserve of −7 (2)% with exercise at baseline (p < 0.001).
As in the patients with aortic regurgitation treated medically, the preserved contractile reserve on exercise was significantly correlated (r = 0.71, p < 0.001) with the change in left ventricular ejection fraction following aortic valve surgery (fig 1B). All of the 13 patients with a positive contractile reserve at baseline had a preserved ejection fraction at follow up. On the other hand, out of the 13 patients with a negative contractile reserve at baseline, 10 showed a significant decrease in ejection fraction on follow up (χ2 = 15.2, p = 0.001) (table 6).
Relation between change in ejection fraction on follow up after aortic valve replacement and contractile reserve at baseline
Figure 2B compares the accuracy of change in end systolic volume with exercise and the contractile reserve for predicting the change in ejection fraction on follow up in patients with aortic regurgitation undergoing aortic valve replacement. Contractile reserve was significantly more sensitive (100%) as compared with change in end systolic volume (40%). Both had a similar high specificity of 81% and 94% (NS), respectively. Contractile reserve had a slightly better accuracy (88% v 73%) for predicting improvement in left ventricular function than change in end systolic volume alone with exercise (NS). Figure 4B gives ROC curves showing the sensitivity and specificity of contractile reserve for predicting change in left ventricular ejection fraction on follow up in patients undergoing aortic valve replacement. A negative contractile reserve of 2% or less had a sensitivity and specificity of 80% for predicting improvement in left ventricular ejection fraction at follow up.
In a stepwise multiple regression model involving resting and exercise indices of left ventricular function in all patients, contractile reserve was the only significant variable to predict the change in left ventricular ejection fraction on follow up (Δ ejection fraction = 0.81*CR + 3.48; p < 0.001).
Discussion
Our findings in this study indicate that in asymptomatic patients with aortic regurgitation and well preserved left ventricular function at rest, contractile reserve identified by exercise echocardiography can be useful in predicting the progressive deterioration of left ventricular function. This appears to be valid both in patients undergoing aortic valve replacement and in those with aortic regurgitation and normal resting left ventricular function on medical treatment. Specifically, failure to reduce end systolic volume or increase the ejection fraction after exercise were specific but of intermediate sensitivity for predicting left ventricular dysfunction at follow up, contractile reserve being marginally more accurate because of the contribution of smaller changes of diastolic volume with exercise. The conventional indices of left ventricular dimensions in diastole or systole, fractional shortening, and exercise indices—including duration of exercise, rate–pressure product, and workload—were not helpful in predicting follow up left ventricular function in either surgical patients or those treated medically. The lack of influence of resting variables probably reflects the fact that most individuals warranting surgery on these criteria proceeded to surgery without recruitment into the study.
DETECTION OF LEFT VENTRICULAR DYSFUNCTION IN AORTIC REGURGITATION
In patients with aortic regurgitation, irreversible impairment of myocardial contractility can be present in the absence of significant symptoms,26 and can adversely affect prognosis even after aortic valve replacement.4 ,14 Previous work has shown that fractional shortening ⩽ 25% and end systolic diameter ⩾ 55 mm may be used to guide the timing of surgery for aortic regurgitation.5 ,27 However, these measurements are relatively insensitive, especially compared with exercise ejection fraction and end systolic volume,26 ,28 and some surgical series have found them too restrictive, based on the postoperative course of symptomatic and asymptomatic patients.14 ,15
Although diastolic and systolic left ventricular dimensions are well correlated with the assessment of left ventricular volumes and function in ventricles of normal size, with increasing left ventricular diameter the relation becomes curvilinear, with pronounced widening of the 95% confidence intervals for the estimated volume.29 The presence of aortic regurgitation also leads to alterations in left ventricular geometry—the ventricle becomes more conical and wider at the base,30 which may lead to an overestimation of the left ventricular volume and ejection fraction if these are based on diameter alone. In our patients, baseline left ventricular dimensions were in the high normal range with a normal fractional shortening, yet patients showed varying functional responses to exercise and a decrease in ejection fraction on follow up. These results confirm the presence of myocardial dysfunction before the left ventricular systolic diameter exceeds 55 mm; in these patients direct measurement of change in left ventricular volumes and ejection fraction with dynamic exercise may add useful information.
LEFT VENTRICULAR RESPONSES TO STRESS IN AORTIC REGURGITATION
The results of this study suggest that a negative contractile reserve is correlated with a decrease in ejection fraction on follow up in both medical and surgical patients (fig 1). These data are concordant with previous reports (not specifically in aortic regurgitation) that inability to increase the ejection fraction and reduce the end systolic volume with stress can be regarded as reliable early markers for progressive deterioration of myocardial contractility.31 ,32
Previous data with aortic regurgitation are more confusing, however. In a study comparing the exercise response in patients with aortic regurgitation with controls,33 both groups showed a decrease in the end systolic volume index and an increase in ejection fraction with exercise. However, patients with symptomatic aortic regurgitation had a significant increase in end systolic volume and a decrease in ejection fraction with exercise, suggesting impaired myocardial contractility. In contrast, Goldman and colleagues found no correlation between the ejection fraction response to exercise and the resting left ventricular dimensions or ejection fraction in a group of patients with aortic regurgitation.34 The subgroup with an abnormal ejection fraction response to exercise was characterised by an increase in peak systolic wall stress. Our data may provide an explanation for these findings, in that while a negative contractile reserve is correlated with a decrease in ejection fraction on follow up, the outcome of patients with a positive contractile reserve is variable. Thus, although a positive contractile reserve confers a better prognosis, other contributing factors may influence outcome.
In asymptomatic patients with aortic regurgitation, Branzi and colleagues reported evidence of impaired myocardial contractility in the form of reduced systolic elastance and increased systolic wall stress in response to increased afterload.35 Again, only a small proportion of the patients had reduced fractional shortening or increased end systolic dimension at rest. In their series, angiotensin was used to increase afterload, but this also has a mild negative inotropic response. In contrast, exercise stress provides an index of effort tolerance in parallel with an augmentation of heart rate, blood pressure, and afterload similar to that invoked by normal daily activity.
Examination of the left ventricular responses to stress in aortic regurgitation has been applied clinically by Borer and colleagues,19, using radionuclide techniques. In minimally symptomatic patients with normal left ventricular function, these investigators found that the change in ejection fraction with exercise (normalised for the change in end systolic wall stress) was the strongest independent predictor of outcome. Indeed, even when this complex variable was not included in their model, change in ejection fraction with exercise could provide most of the independent prognostic information. These results are confirmed by our finding that the contractile reserve with exercise is a useful and reliable predictor of progressive left ventricular dysfunction on medical treatment and an even more significant predictor of improvement of left ventricular function after aortic valve replacement. The ability to gather these data with exercise echocardiography, which is more widely available than exercise nuclear ventriculography, represents an enhancement of the feasibility of this approach.
MEDICAL VERSUS SURGICAL PATIENTS
The results of this study indicate that loss of contractile reserve is quite specific as a harbinger of resting dysfunction, whether the patient undergoes valve surgery or not. The outcomes of patients with preserved contractile reserve are more variable, and are clearly influenced by other factors—for example, progression of the valvar lesion, coexistent myocardial disease, and ischaemia. Given the treatment of the valvar lesion and concomitant coronary surgery if necessary in the surgical group, these confounding factors are more prevalent in the medically treated group, and probably explain the greater variation in the relation between contractile reserve and evolution of left ventricular function.
LIMITATIONS
The results of the study need to be placed in the context of various considerations relating to the study design. First, the Cleveland Clinic Foundation is a referral institution for valve surgery and many patients were available for study because of referrals regarding the timing of surgery. This selection process may lead to overrepresentation of patients with difficult management problems such as severe regurgitation without gross left ventricular enlargement, but given the impact of contractile reserve in both medically and surgically treated groups, it is difficult to explain our findings on the basis of patient selection. Second, the duration of follow up was relatively short and further alterations in left ventricular function (and especially clinical condition) might have been seen if the group had been followed for longer. Third, while the patients of interest (asymptomatic, relatively small left ventricular cavity) are a subgroup of a large number of patients with aortic regurgitation, in absolute terms the numbers of patients are relatively small. Finally, the disadvantage of observational studies is that they present relations but neither prove causation nor explain the findings.
We believe that the impact of contractile reserve on outcome reflects the fact that the exercise response of the ventricle is more representative of left ventricular compromise than is resting function, but we cannot exclude the possibility that another mechanism is at work. Similarly, the finding that the increment of ejection fraction on follow up was greatest in patients with more enlarged ventricles preoperatively (table 3) most probably reflects the fact that the short follow up precludes the resolution of left ventricular enlargement. The volume changes following recovery of the myocardium in this situation may therefore have exceeded those in smaller ventricles. It is important to recognise that these patients did not have abnormal resting volumes at baseline, so this relation concerns volumes that are at the upper limit of normal. Alternative explanations may include changes in left ventricular geometry in patients with aortic regurgitation; loss of long axis function as the ventricle becomes more spherical may engender a reduction of ejection fraction despite preserved fractional shortening in a small but not in a larger ventricle.
CLINICAL IMPLICATIONS
Left ventricular function is a major determinant of long term prognosis,3 and the principal aim in the management of patients with chronic asymptomatic aortic regurgitation is to be able to predict and pre-empt the development of irreversible left ventricular systolic dysfunction. In this study of asymptomatic patients with normal resting left ventricular function, conventional indices of left ventricular size and function, exercise capacity, and clinical characteristics did not predict the latent left ventricular dysfunction on medical follow up or the improvement in left ventricular function after aortic valve replacement surgery. Contractile reserve and the decrease in end systolic volume with exercise measured by exercise echocardiography were predictive of progressive deterioration of left ventricular function in these patients.
Decision making with respect to the timing of surgery in aortic regurgitation may be difficult. Excessive delay risks irreversible left ventricular enlargement owing to the chronic volume load. However, unlike mitral regurgitation, valve repair is generally not feasible, so early surgery exposes the patient prematurely to the risks inherent in having a prosthetic valve. The decision to proceed with surgery in an asymptomatic patient is multifactorial, but the assessment of contractile reserve may be a useful adjunct to resting left ventricular size and function. This approach has the benefit of involving widely available exercise and echocardiographic equipment rather than requiring referral to a nuclear cardiology facility. While there is undoubtedly a learning curve in the performance of exercise echocardiography, image interpretation is less challenging to the observer than evaluation of regional wall motion abnormalities. New techniques such as tissue Doppler may be useful in quantifying the left ventricular response to stress and obviate the process of tracing systolic and diastolic contours to obtain the ejection fraction.