Article Text

Abstract
OBJECTIVE To determine baseline predictors of tolerance to the α/β blocker carvedilol in everyday clinical practice.
DESIGN Retrospective analysis of tolerance to carvedilol in patients with chronic heart failure. Tolerance was defined as currently on carvedilol or on it at the time of death or heart transplantation. To meet the criteria for tolerance, carvedilol had to be prescribed at a stable dose for ⩾ 3 months.
SETTING Everyday clinical practice, comprising both hospital specialist practice and private practice. Tolerance was assessed in all patients prescribed carvedilol for chronic heart failure in those practices.
PATIENTS 808 consecutive patients in both hospital specialist (611 patients) and private practice (197 patients).
MAIN OUTCOME MEASURES Baseline predictors of tolerance assessed by proportional hazards analysis. Both univariate and multivariate analyses were performed.
RESULTS Within the entire cohort of 808 patients, 95 had stopped carvedilol, 606 were currently receiving the drug, 50 had died, and 44 had received a heart transplant. Overall, 88% of patients tolerated carvedilol (87% in the hospital specialist group, 92% in the private practitioner group). Factors that indicated impaired tolerance by univariate analysis were increased age in years (hazard ratio 1.01, 95% confidence interval (CI) 1.0 to 1.3), low diastolic blood pressure (hazard ratio 1.04, 95% CI 1.02 to 1.08), and raised plasma urea concentration (hazard ratio 1.04, 95% CI 1.02 to 1.05). New York Heart Association (NYHA) class was also a marker of tolerance (proportion not tolerated: 3% class I; 9% class II; 13% class III, 22% class IV). By multivariate analysis, no single baseline variable was an independent marker of inability to tolerate carvedilol. Tolerance was also assessed in relation to traditional precautions or relative contraindications to β blockade. Tolerance in these subgroups was: chronic obstructive airways disease/asthma 85% (89 patients), diabetes 86% (127 patients), peripheral vascular disease 84% (58 patients), concomitant amiodarone treatment 83% (230 patients), and heart rate < 70 beats/min 84% (184 patients).
CONCLUSIONS β Blocker treatment was well tolerated in everyday clinical practice, including non-hospital-based private practice. There was no single predictor of poor tolerance on multivariate analysis, although there was a clear association with NYHA class as well as age, diastolic blood pressure, and plasma urea on univariate analysis. Carvedilol was tolerated well among selected patients with traditional contraindications to β blockade in this situation.
- chronic heart failure
- β blockade
- carvedilol
Statistics from Altmetric.com
β Adrenoceptor blockers are of well established clinical benefit when added to angiotensin converting enzyme (ACE) inhibitors and diuretics (with or without digoxin) in patients with New York Heart Association (NYHA) class II and III systolic chronic heart failure.1 ,2 However, despite the extensive clinical trial data supporting their use in this setting, the uptake of β blockers has been relatively low. It is usually said that β blockers are contraindicated for the treatment of systolic chronic heart failure because of the possibility that they might cause deterioration of cardiac function. Furthermore, certain β blocking drugs such as carvedilol also possess vasodilator properties,3 which may add to physicians' concerns over the use of these agents in chronic heart failure.
These factors may make physicians reluctant to use agents such as carvedilol in this setting, despite the overwhelming evidence of clinical benefit. This reluctance might be alleviated if it was possible to predict in advance which patients with chronic heart failure are likely to have difficulty in tolerating β blocker treatment. At present, the data available to address this issue are double blind, placebo controlled clinical studies of the efficacy of β blockade.4-8 However, no independent baseline predictors of poor tolerance to β blockade have emerged from such studies.
The carvedilol in chronic heart failure clinical programme included an open label initiation of active treatment in both the American multicentre trial4 and the Australia/New Zealand trial,5 which may have led to a perception of bias in patient selection for the double blind phase of the trials. These considerations may have led some physicians to conclude that the clinical trial programme of β blockers in chronic heart failure does not reflect the true value of these agents. There are very few reports on tolerance to β blockade in everyday clinical practice outside of the controlled clinical trial environment. As carvedilol is the only β blocker approved in Australia for use by specialist physicians in the treatment of systolic chronic heart failure (and has not been approved for any other indication), this gave us the opportunity to examine the above issues in a clinical practice setting.
Our aim in this study was therefore to determine which patients were able to tolerate the initiation and up-titration of carvedilol and be maintained on it in everyday clinical practice, as determined from baseline demographic and cardiac variables.
Methods
PATIENT POPULATION
This was a retrospective analysis of all patients with systolic chronic heart failure who were initiated on open label carvedilol treatment in hospital outpatient clinics (two sites) and cardiological private practice (five sites) throughout Australia since the drug was approved in 1997. A minimum of 30 consecutive patients initiated on carvedilol was required at each individual site. Patients receiving carvedilol for indications other than chronic heart failure were excluded from the analysis. Patients had to have been receiving carvedilol for at least three months in order to contribute to the study. The only exception was patients in whom carvedilol had been discontinued within three months of starting the treatment; these patients were included in the data analysis and reasons for discontinuation ascertained.
STUDY DESIGN
Baseline (pre-carvedilol) demographic and cardiac status data were collected. Specifically, data on the following baseline variables were collected: demographics (age, sex, height, weight); cardiac status (baseline blood pressure, heart rate, NYHA class, ejection fraction (within the previous 12 months); six minute walk test (within the previous three months); heart rhythm; and plasma sodium, urea, and creatinine concentrations. Also recorded was the duration of heart failure, the presence of a permanent pacemaker, a history of ventricular arrhythmia, the need for intravenous heart failure drug treatment in the previous three months, and hospital admission for heart failure in the previous three months.
Comprehensive data were also collected on patient comorbidities and potential causes of heart failure. Specifically, data were collected on the presence or absence of systemic hypertension, diabetes, ischaemic heart disease, myocardial infarction, and valvar heart disease, as well as on previous alcohol intake, drug treatment, and other factors that may have contributed to the development of chronic heart failure. In addition, data were collected on other diseases relevant to the initiation of β blockade such as fixed airways disease, asthma, and peripheral vascular disease.
Data were collected on concomitant drug treatment taken by the patient at the time carvedilol was started. These included background chronic heart failure drugs, with their dosage, other cardiovascular drugs, and non-cardiovascular drugs.
Data were then obtained on the initiation and up-titration of carvedilol treatment. In particular, data were collected on the starting dose, the first stable carvedilol dose (defined as the first dose which was unchanged for three months), time to first stable carvedilol dose, and the ACE inhibitor and diuretic dose at the time of the first stable carvedilol dose.
Finally, data on current status of the patient were obtained—whether they were alive, dead, or had received a heart transplant. We were particularly interested in whether patients were on the drug (and the dose) at the time of death or transplantation, or whether they were alive and still on the drug. If patients were still taking carvedilol, the dose was recorded together with the dose of other concomitant drugs. If patients had stopped taking carvedilol, the dose at which the drug was discontinued and reasons for cessation were recorded.
STATISTICAL ANALYSIS
To address whether there were baseline differences between patients who tolerated carvedilol and those who did not, a proportional hazards regression model was fitted in which associations between baseline variables and time to discontinuation were tested. In the univariate analysis, each term was fitted separately, with time to discontinuation curves constructed and log rank tests performed. Continuous variables, for example blood pressure, were stratified by quartile in the proportional hazards regression model. Similarly, tolerance in relation to NYHA class was assessed by a proportional hazards analysis on time to discontinuation, with NYHA class fitted using indicator variables. Baseline variables that were univariate predictors of tolerance to carvedilol were subsequently fitted to a multiple proportional hazards regression model. A probability value of p < 0.05 was considered to be significant.
Results
Eight hundred and eight patients were recruited into the study: 86.6% were male and 13.4% were female; 76% were recruited from hospital specialist heart failure clinics and 24% from private cardiological practice. Their mean age was 58 years (range 0–91 years). The patients mostly had NYHA class II and III symptoms of chronic heart failure (NYHA class I/II/III/IV, 59/201/254/89). Fifty patients (6%) had died and 44 (5%) had received a heart transplant. Six hundred and six patients (75%) were current users of carvedilol and 95 (12%) had stopped use but were still alive and had not had a heart transplant.
Thus carvedilol was “tolerated” as defined in this study (currently on carvedilol for a minimum three months of treatment, or on carvedilol at time of death or transplant) by 88% of patients. The mean first stable dose was 19 mg twice daily (interquartile range 12.5–25 mg twice daily). The mean time to first stable dose was 89 days (interquartile range 32–191 days).
BASELINE PREDICTORS OF TOLERANCE
Discontinuation of carvedilol was significantly related to NYHA class, with 97% of class I patients able to tolerate carvedilol but only 78% of class IV patients tolerating the drug (fig 1). Other baseline variables that were significant predictors of inability to tolerate carvedilol on univariate analysis were increased age, low diastolic blood pressure, and high blood urea concentration. Hazard ratios for inability to tolerate carvedilol were: increased age in years, 1.01 (95% confidence interval (CI) 1.0 to 1.3); low diastolic blood pressure, 1.04 (95% CI 1.02 to 1.08); and high urea concentration, 1.04 (95% CI 1.02 to 1.05). However, when these univariate predictors of poor tolerance were fitted into a multivariate regression equation, no single independent predictor of poor tolerance emerged.

Per cent of patients unable to tolerate carvedilol treatment, grouped according to New York Heart Association (NYHA) functional class. Data analysed by proportional hazards analysis on time to discontinuation (intolerance), with NYHA class fitted using indicator variables.*Proportional hazards analysis on time to discontinuation (intolerance) with NYHA class fitted using indicator variables.
TOLERANCE ACCORDING TO DEMOGRAPHIC DATA
Demographic data in patients who were able to tolerate or could not tolerate carvedilol are summarised in table 1. Only diastolic blood pressure was a significant predictor of poor tolerance.
Selected demographic variables in patients who were able to tolerate or could not tolerate carvedilol
TOLERANCE ACCORDING TO PRESCRIBING PHYSICIAN
We categorised tolerance according to hospital heart failure specialist or private cardiology practitioner as managing physician. Among hospital specialists (603 patients), 87% of the patients tolerated carvedilol and 13% did not. Among private practitioners (192 patients), 92% of the patients tolerated carvedilol and 8% did not. We also compared tolerance among the first 50% of patients treated by practitioners—that is, the earliest experience of carvedilol—compared with the second 50%. More patients tolerated carvedilol among the second 50% (91% v 86%) but the difference was not significant by χ2 analysis.
TOLERANCE ACCORDING TO TRADITIONAL PRECAUTIONS IN PRESCRIBING β BLOCKERS
We were able to examine tolerance to carvedilol in relation to traditional relative contraindications to prescribing β blockers. These included chronic airways disease/asthma, diabetes, peripheral vascular disease, low heart rate, and the use of concomitant agents that may exacerbate adverse effects with β blockade, for example amiodarone. These data are summarised in fig 2.
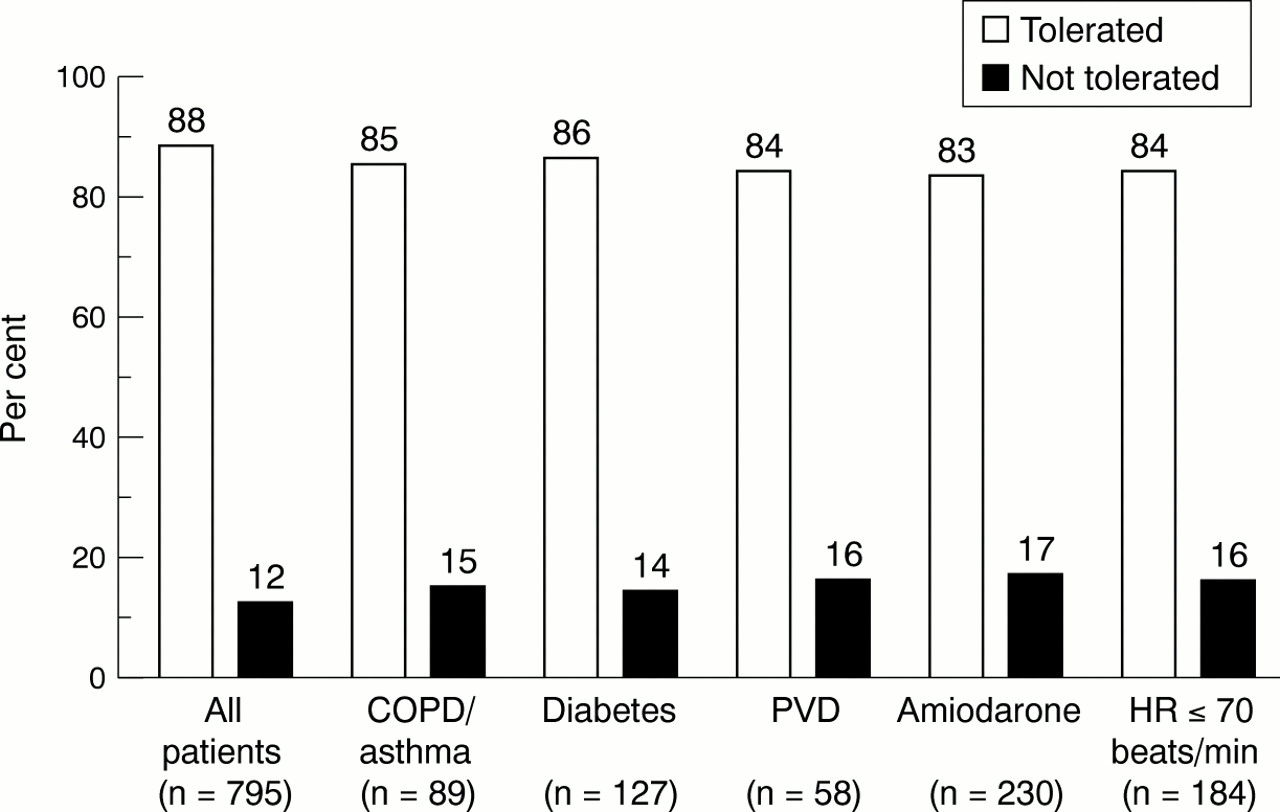
Per cent of patients able to tolerate carvedilol treatment, grouped according to traditional contraindications and precautions in prescribing a β blocker. COPD, chronic obstructive pulmonary disease; HR, heart rate; PVD, peripheral vascular disease.
OTHER DATA ON CARVEDILOL TOLERANCE
A breakdown of the first stable dose of carvedilol is presented in fig 3. Most patients were able to reach the standard target dose of 25 mg twice daily.
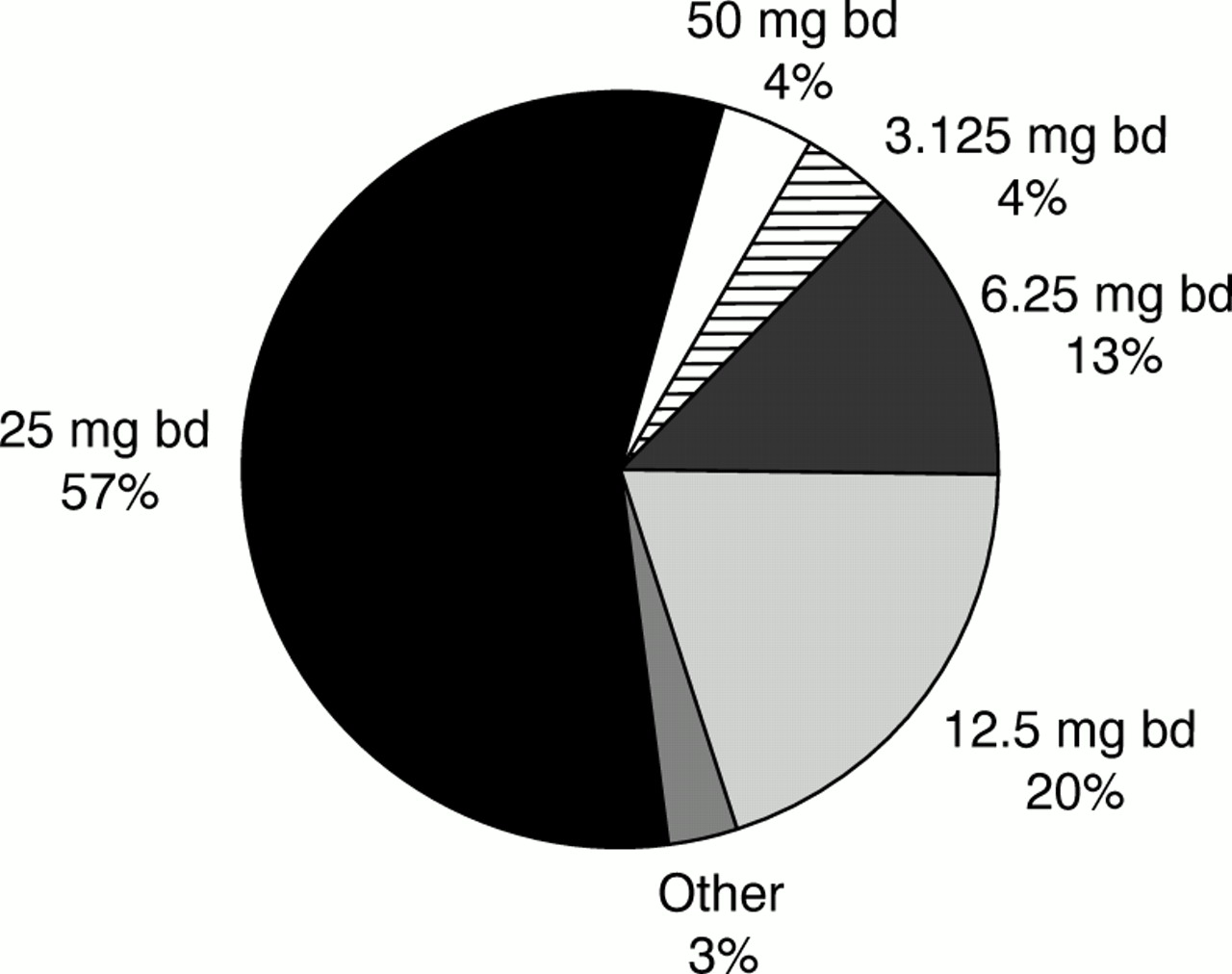
First stable dose of carvedilol achieved in study patients.
Reasons for discontinuation of carvedilol are shown in fig 4. These include expected reasons for discontinuation such as worsened heart failure, symptomatic hypotension and bradycardia, as well as tiredness and wheeze. A series of other reasons for discontinuation comprise a large proportion of the subset. These included cough, nausea, arrhythmia, renal dysfunction, diarrhoea, rash, and non-compliance.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Reason for discontinuation of carvedilol among study patients. CHF, chronic heart failure.
Discussion
In this study we sought to examine baseline variables that may predict tolerance to carvedilol in patients with chronic heart failure when the drug was initiated during everyday clinical management. We specifically sought to do this outside the clinical trial setting, as this drug is now approved for heart failure management and is widely prescribed. Furthermore, carvedilol is the only β blocker currently approved for use in systolic chronic heart failure in Australia, and it is not approved for any other indication. Thus it may be expected that an assessment of tolerance among all patients with systolic chronic heart failure who were prescribed this drug in everyday practice would closely reflect physicians' experience with initiating β blockade in this setting. The opportunity to examine tolerance during ordinary use (in contrast to during the conduct of clinical efficacy trials) would be expected to be particularly relevant for the prescribing physician.
Overall, our findings were that initiation of β blockade with carvedilol was extremely well tolerated. The tolerance observed among patients prescribed the drug in the private practice setting was at least as good as, if not better than, that seen in the hospital setting. It must be emphasised, however, that this study excluded analysis of patients who may have been eligible to receive carvedilol treatment but who were not started on the drug by their treating physician. As we did not analyse such patients, it was not possible to assess the degree of patient selection undertaken by the physicians contributing patients to this study. However, in the recent BRING-UP study (β blockers in patients with congestive heart failure: guided use in clinical practice),9 a “real world” study conducted in Italy, 47.2% of patients considered for β blockade did not ultimately receive these agents.
Very few baseline variables predicted the inability of patients to tolerate carvedilol. Those that were predictive statistically on univariate analysis (advanced age, low diastolic blood pressure, high urea, and advanced NYHA class) are to be expected, on the basis that they reflect patients more vulnerable to the effects of cardiovascular drugs in general (advanced age), those with more severe disease (low diastolic blood pressure and advanced NYHA class), or those with multiple organ impairment (high urea concentration). Because these factors tend to cluster within certain individuals (colinearity), it was not surprising that none of the baseline variables that were predictive on univariate analysis remained as independent predictors when entered into a multivariate model.
The finding that no baseline variable could predict inability to tolerate β blocker treatment is consistent with data from recent clinical trials which were also generally unable to find baseline predictors of poor tolerance.4-8
An important finding in the present study was that patients with comorbidities that would represent a relative contraindication to β blocker treatment were in fact able to tolerate carvedilol remarkably well. These comorbidities include diabetes, chronic airways obstruction, and peripheral vascular disease, as well as other relative contraindications to β blocker treatment. There was very little further reduction in the percentage of patients able to tolerate carvedilol in comparison with the cohort as a whole. These findings may reflect a degree of patient selection in that physicians will only have prescribed the drug to patients whom they thought capable of tolerating β blocker treatment. This is supported by the observation in the BRING-UP study9 that the main reason for non-selection of a patient for β blockade is a perceived contraindication to giving the drug. Nevertheless the findings of our present study suggest that if a clinically guided selection of patients with such comorbidities is made by the treating physician, tolerance to the drug can be expected to be reasonably good.
Because β blocker treatment is up-titrated from relatively low doses in the management of patients with chronic heart failure, another marker for tolerance to these agents is the first stable dose achieved. In this analysis, 61% of patients were able to reach a dose of carvedilol of 25 mg twice daily or more, again reflecting excellent tolerance of the drug. Thus only a minority of patients were unable to reach the target dose of treatment. Indeed, all but 4% of patients were able to reach 6.25 mg twice daily, which is where clinical benefit begins to be observed with the drug.10 The figures on the percentage reaching target dose compare favourably with those observed with ACE inhibitors in clinical trials11 and in everyday practice.12
CONCLUSIONS
Carvedilol treatment for systolic chronic heart failure was extremely well tolerated in this retrospective analysis of carvedilol initiation, up-titration, and ongoing treatment. The majority of patients were able to achieve target doses of drug, and the tolerance observed in the hospital setting was preserved in private practice. Furthermore, there was little fall off in tolerance among selected patients with relative contraindications to β blocker treatment. Univariate predictors of poor tolerance reflected a general increase in the risks of receiving cardiovascular drugs or having more advanced disease. However, on multivariate analysis there were no independent predictors of inability to tolerate carvedilol treatment.
Acknowledgments
Supported by a grant from F Hoffmann-LaRoche Ltd, Basel, Switzerland. The study was conceived, designed, and conducted by the authors, independent of the study sponsors. We wish to acknowledge the expert statistical support of Dr Andrew Martin, Roche Biometrics, Dee Why, NSW, Australia, in assisting with analysis of this study. Study sites: Victoria (H Krum, D Ninio, D Rose), NSW (P MacDonald), Tasmania (M Loughead), Western Australia (M Ireland). Study Coordinators: J Hankin, T James, J Ferguson.