Article Text

Abstract
OBJECTIVE To clarify the relative contribution of resting haemodynamic profile and pulmonary function to exercise capacity in patients with heart failure.
SETTING Cardiology department and cardiac rehabilitation unit in a tertiary centre.
DESIGN 161 male patients (mean (SD) age 59 (9) years) with heart failure (New York Heart Association class II–IV, left ventricular ejection fraction 23 (7)%) underwent spirometry, alveolar capillary diffusing capacity (DLCO), and mouth inspiratory and expiratory pressures (MIP, MEP, respectively, in 100 patients). Right heart catheterisation and a symptom limited cardiopulmonary exercise test were performed in 137 patients within 3–4 days.
RESULTS Mean peak exercise oxygen consumption (V˙o 2) was 13 (3.9) ml/kg/min. Among resting haemodynamic variables only cardiac index showed a significant correlation with peakV˙o 2. There were no differences in haemodynamic variables between patients with peakV˙o 2 ⩽ or > 14 ml/kg/min. There was a moderate correlation (p < 0.05) between several pulmonary function variables and peak V˙o 2. Forced vital capacity (3.5 (0.9) v 3.2 (0.8) l, p < 0.05) and DLCO (21.6 (6.9) v 17.7 (5.5) ml/mm Hg/min, p < 0.05) were higher in patients with peakV˙o 2 > 14 ml/kg/min than in those with peak V˙o 2 ⩽ 14 ml/kg/min. Using a stepwise regression analysis, the respiratory and haemodynamic variables which correlated significantly with peakV˙o 2 were DLCO, MEP, and cardiac index, with an overall R value of 0.63.
CONCLUSIONS The data confirm previous studies showing a poor correlation between resting indices of cardiac function and exercise capacity in heart failure. However, several pulmonary function variables were related to peak exerciseV˙o 2. In particular, lung diffusing capacity and respiratory muscle function seem to affect exercise tolerance during heart failure.
- heart failure
- exercise
- pulmonary function
- alveolar–capillary diffusing capacity
Statistics from Altmetric.com
Exercise intolerance is one of the most common clinical features of patients with chronic heart failure. Different mechanisms may contribute to the poor functional capacity of these patients, such as an altered haemodynamic response during exercise,1 ,2 abnormalities of skeletal muscle structure and function,3 ,4 a reduced vasodilator capacity of peripheral vessels,5 ,6 and neurohormonal changes.7 Several abnormalities of pulmonary function have also been described in heart failure patients8, but no clinical relevance was initially attached to these findings, as arterial oxygen desaturation does not usually appear during exercise in these patients.9However, recent studies have shown that some measures of lung function—such as forced vital capacity and lung diffusing capacity to carbon monoxide—are significantly related to exercise tolerance, as expressed by oxygen uptake (V˙o 2) measured at peak exercise in heart failure patients.10 ,11Accordingly, in this study we attempted first, to assess the presence of pulmonary function abnormalities; second, to evaluate their role in determining the exercise capacity, as expressed by peakV˙o 2; and third, to compare their contribution to peak V˙o 2 with that of the resting haemodynamic profile, as assessed by right heart catheterisation, in a group of patients with heart failure.
Methods
STUDY GROUP
We studied 161 male patients (mean (SD) age 59 (9) years, range 21–75 years) with chronic heart failure of at least six months' duration caused by left ventricular systolic dysfunction. Mean left ventricular ejection fraction was 23 (7)% (range 10–40%), as assessed by mean cross sectional echocardiographic values. The aetiology of heart failure was chronic coronary artery disease in 91 patients (56.5%) and idiopathic dilated cardiomyopathy in 70 (43.5%). One hundred and eight patients were in New York Heart Association (NYHA) functional class II, 48 in class III, and five in class IV. A smoking history was present in 115 patients (71%), but none was a current smoker at the time of the study.
Patients were studied when they were clinically stable, without any changes in drug treatment during the previous three weeks. All patients were on diuretics and most of them (n = 144, 89%) were on an angiotensin converting enzyme (ACE) inhibitor; 100 (62%) were receiving digoxin and 80 (50%) were on oral or transdermal nitrates. Amiodarone was being taken by 20 patients (12.5%). None of the patients was on treatment with β adrenergic blocking agents, calcium channel blockers, or bronchodilators. We excluded patients unable to exercise because of non-cardiac limitations, those with reduced exercise tolerance caused by major ventricular arrhythmias or myocardial ischaemia, those with recent (⩽ 3 months) myocardial infarction or acute myocarditis, with valvar or congenital heart disease, or awaiting myocardial revascularisation, and those requiring intravenous inotropic agents or mechanical circulatory support. Seventeen women with chronic heart failure were also evaluated; however, they were older than the men (mean age 75 (6) years), had a higher left ventricular ejection fraction (> 45% in nine), and only eight and nine underwent right heart catheterisation and exercise testing, respectively. Accordingly, we decided to not include their data in the analysis.
PULMONARY FUNCTION TESTS
Dynamic lung volumes were measured in the sitting position using a pneumotachograph with a volume integrator (Medical Graphics, St Paul, Minnesota, USA). The best of three consecutive tests was used. Lung volumes were expressed in litres and as a percentage of the predicted normal values according to age, sex, height, and weight.12The alveolar–capillary carbon monoxide diffusing capacity (DLCO) was measured by the single breath technique according to the European Respiratory Society guidelines.13 While the subject was breathing through a mouthpiece, five tidal volumes were recorded. After expiration to residual volume, the mouthpiece was connected to a source of test gas (0.3% carbon monoxide, 0.5% neon, 21% oxygen, 78.25% nitrogen); the patient then inhaled to total lung capacity, holding his breath for 10 seconds, and then rapidly exhaled to residual volume. The first 750 ml of expired gas was discarded as washout volume, followed by collection of the next 600 ml for gas analysis. The DLCO was expressed both as an absolute value in ml/mm Hg/min and as a percentage of the predicted normal value; the reproducibility of DLCO was ±5% in our laboratory.14
Maximum inspiratory pressure (MIP) was measured at lung functional residual capacity, and maximum expiratory pressure (MEP) was measured at total lung capacity in 100 patients, using a mouthpiece with a small leak connected to a pressure transducer. After education in the technique, several recordings were made until at least three tracings with reproducible pressure profiles were obtained. The best values of MIP and MEP sustained for at least one second were used in the analysis.15
EXERCISE TESTING
All patients underwent a symptom limited exercise test on a bicycle ergometer, in the upright position, with 10 W/min increments, within 2–3 days from the time of the pulmonary function tests. Respiratory variables were continuously monitored using a commercial instrument (Marquette 1100 medical gas analyser, Milwaukee, Wisconsin, USA). Peak exercise V˙o 2 was obtained by averaging the last 30 seconds of the incremental test.
CARDIAC CATHETERISATION
Right heart catheterisation was performed in 137 patients within three to four days of the pulmonary function and exercise tests, using a triple lumen Swan-Ganz catheter introduced percutaneously through the right internal jugular vein and positioned in the pulmonary artery to obtain right heart pressures. Cardiac output was measured in triplicate by the thermodilution method. Arterial blood pressure was measured by cuff sphygmomanometry. Derived haemodynamic variables were calculated using standard formulae.16
STATISTICAL ANALYSIS
All data are expressed as mean (SD). Differences between groups were assessed using unpaired t test, analysis of variance, or χ2 analysis. A probability value of p < 0.05 was considered significant. Correlations between peakV˙o 2 and haemodynamic or pulmonary variables were assessed by univariate linear regression analysis, Spearman rank order analysis, and multivariate stepwise regression analysis as appropriate.
Results
The haemodynamic and pulmonary function variables of patients with heart failure are presented in tables 1 and 2, respectively. Compared with normal values, the resting haemodynamic profile of these patients was characterised by a moderate increase in right heart pressures, a pronounced increase in left atrial pressure (as assessed by pulmonary artery wedge pressure), and a reduction in cardiac index (table 1). Indices of pulmonary function were also abnormal, as indicated by the data expressed as percentage of predicted values; in particular, heart failure patients showed a reduction in DLCO, MIP, and MEP (table2).
Resting haemodynamic profile in patients with chronic heart failure
Pulmonary function tests in patients with chronic heart failure
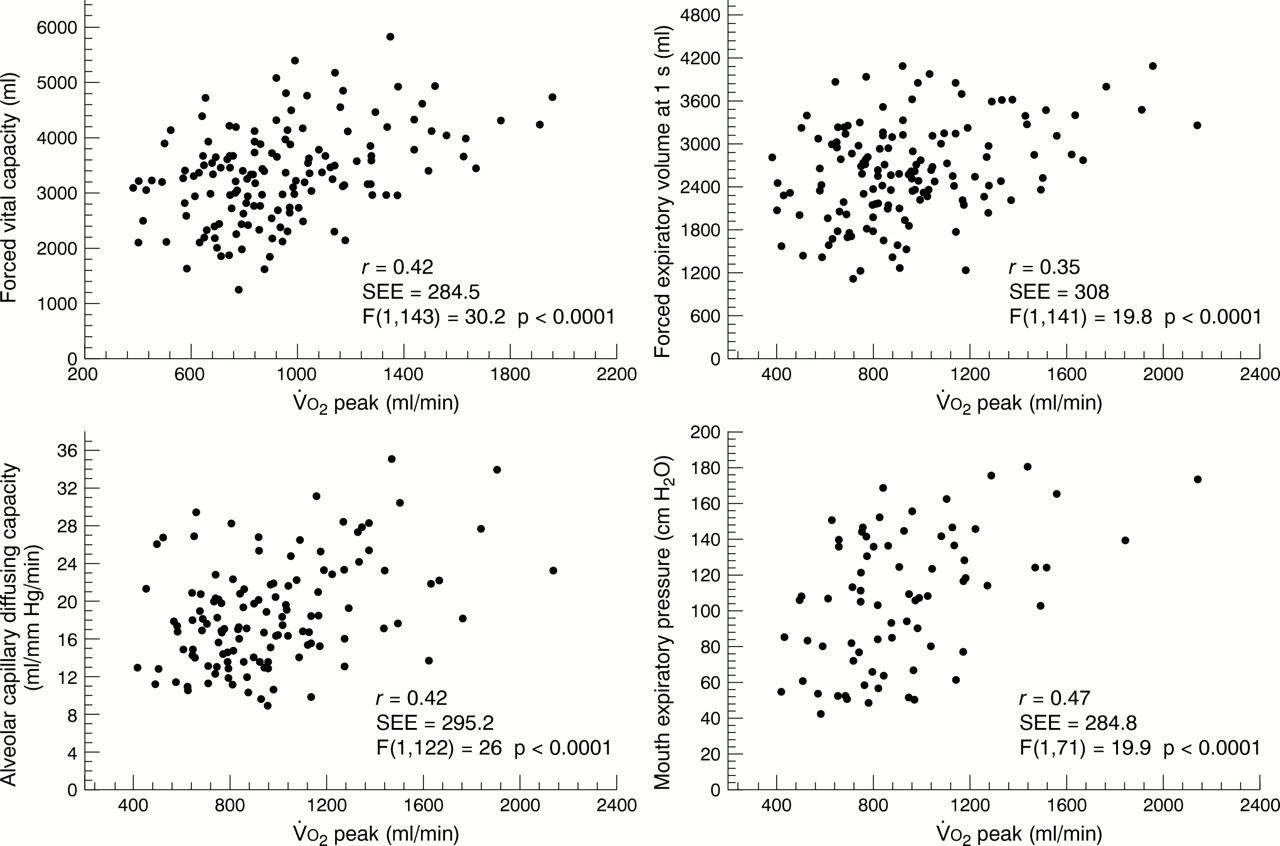
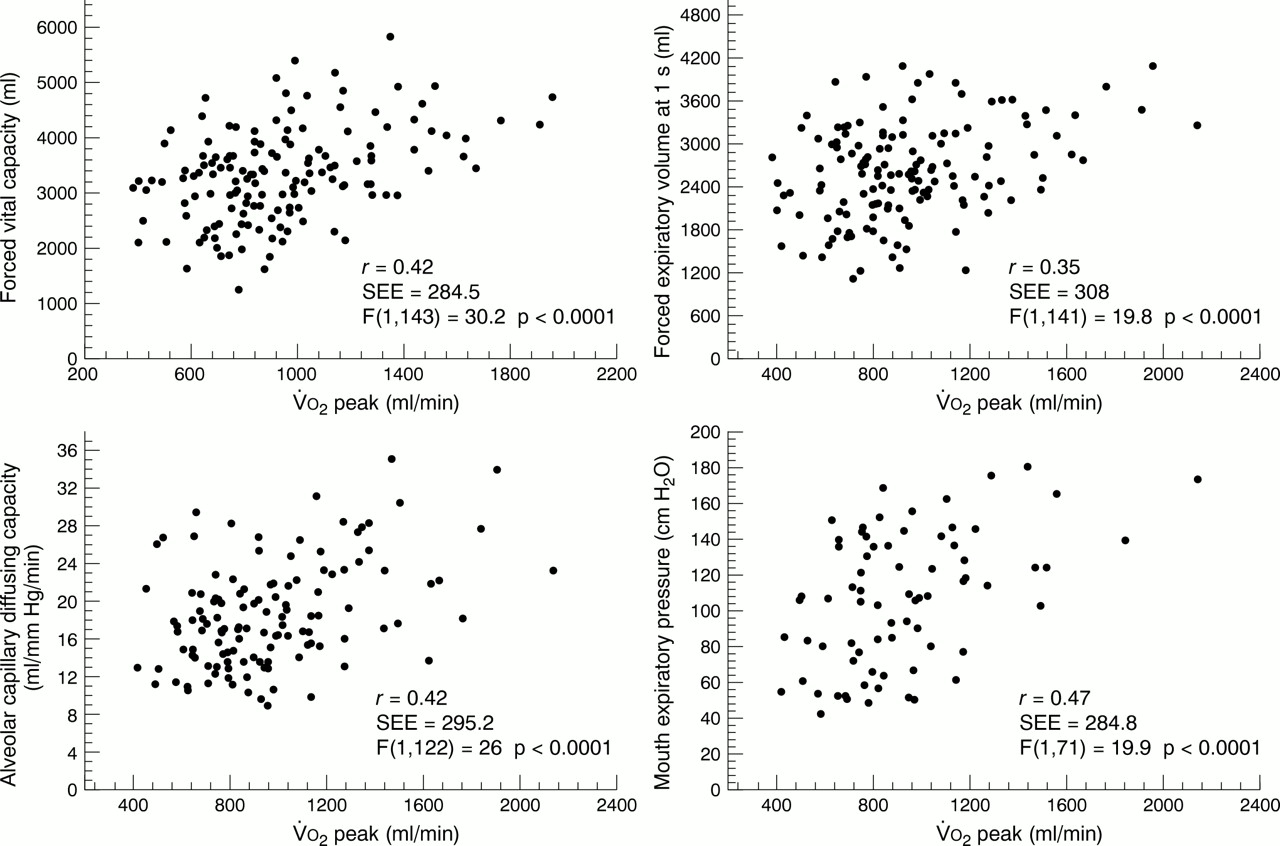
Exercise testing showed a moderate to severe reduction in exercise tolerance, as indicated by a mean (SD) value ofV˙o 2 at peak exercise of 13 (3.9) ml/kg/min (range 7–22 ml/kg/min). Among the resting haemodynamic variables, only the cardiac index showed a significant correlation, though of very low degree, with peak exerciseV˙o 2 (table 3, fig 1); furthermore, the haemodynamic profile showed no difference between the 95 patients with a moderate to severe reduction in functional capacity (peakV˙o 2 ⩽ 14 ml/kg/min, group 1) and the remaining 42 patients with a mild reduction in exercise tolerance (peakV˙o 2 > 14 ml/kg/min, group 2) as shown in table 1. On the other hand, we found significant differences in some lung function variables between patients divided according to the value of peak V˙o 2. In fact, group 1 patients (peak V˙o 2 ⩽ 14 ml/kg/min) showed a significantly lower value of forced vital capacity and DLCO than group 2 patients (peak V˙o 2 > 14 ml/kg/min), as shown in table 2. Furthermore, a significant correlation was found between peak V˙o 2 and several pulmonary function variables (table 3, fig 2).
Linear regression analysis for haemodynamic and pulmonary function variables versus peak exerciseV˙o 2 in patients with chronic heart failure

Linear regression analysis between peak exercise oxygen uptake (V˙o2 peak) on the x axis and several haemodynamic variables on the y axis. See text for details.
{kind=link}
{kind=link}
Linear regression analysis between peak exercise oxygen uptake (V˙o2 peak) on the x axis and lung function indices on the y axis. See text for details.
Forward stepwise linear regression analysis was performed using those variables that were significantly correlated with peakV˙o 2 on univariate analysis. It was found that peak V˙o 2 could be best predicted by DLCO and MEP; the combination of those two variables yielded an overallR value of 0.59, and anR 2 value of 0.35 (p < 0.001), accounting for more than one third of the variance in peak exerciseV˙o 2; cardiac index was the only haemodynamic variable entering in stepwise analysis, and accounted for only a minimal increase in overall R (0.63) and R 2 values (0.39).
The distribution of drug treatment between the patients with moderate to severe (group 1) and mild reduction of exercise tolerance (group 2) was similar; in particular, all patients in both groups were on diuretics, and 100 of 109 group 1 patients (91%) compared with 44 of 52 group 2 patients (84%) were on ACE inhibitors (NS). Among the 20 patients on chronic treatment with amiodarone, 14 (13%) were in group 1 and six (11%) in group 2 (NS). Furthermore, mean values of resting haemodynamic variables and pulmonary function indices were unchanged when patients on amiodarone were excluded.
Discussion
The results of our study, obtained in a relatively large group of heart failure patients, confirm data from previous studies showing that there is a poor relation, or no relation at all, between resting indices of central haemodynamic function and exercise capacity.6 ,17-19 It has also been reported that the haemodynamic improvement obtained with inotropic or vasodilator drugs is unable to produce an immediate change in exercise tolerance,20 thus confirming the limited role of the resting haemodynamic profile as a determinant of exercise capacity in heart failure. On the other hand, we found that several lung function variables showed some relation to exercise tolerance, confirming results of recent studies.10 ,11 ,21 ,22 In particular, spirometric variables—such as forced vital capacity and forced expiratory volume in one second, DLCO, and respiratory muscle function (as measured by MIP and MEP)—were found to be significantly related with peak exerciseV˙o 2.6Furthermore, forced vital capacity and lung diffusion were significantly lower in patients with a more pronounced reduction in functional capacity, as expressed by a peakV˙o 2 value of ⩽ 14 ml/kg/min, than in those with a peak V˙o 2 of > 14 ml/kg/min. Finally, on stepwise analysis the combination of two lung function variables, DLCO and MEP, accounted for at least one third of the variance in peak V˙o 2, with only one haemodynamic variable, the cardiac index, minimally contributing to the variance itself.
PATHOPHYSIOLOGY AND POTENTIAL CLINICAL RELEVANCE
The pathophysiological basis of the relation between the abnormalities of lung function and maximum exercise tolerance is not yet well defined. It has been shown that the alteration of DLCO in heart failure depends on the respective changes of its two components—that is, the diffusing capacity of the membrane and the pulmonary capillary blood volume; pulmonary congestion usually increases capillary blood volume, whereas interstitial oedema and thickening of the alveolar–capillary membrane reduces diffusion through the membrane, with disparate effects on DLCO.11 ,23 An inverse relation between membrane diffusing capacity and pulmonary vascular resistance has been reported,11 ,23 suggesting that these two variables reflect the same pathological process—that is, the pulmonary microvascular damage resulting from long standing pulmonary hypertension in heart failure.24 Also, Puri and co-workers11 found a better correlation between peak exercise V˙o 2 and membrane diffusing capacity (r = 0.72), than we found using total DLCO, which also includes pulmonary capillary blood volume (r = 0.42), supporting the hypothesis of a contributing role of abnormalities of alveolar–capillary structure and function to exercise capacity in heart failure patients. It is of interest that two indices of cardiac function indirectly related to lung diffusing capacity were also significantly related to exercise tolerance: one was the filling pattern of the left ventricle, as assessed by Doppler study of transmitral blood flow,25 ,26which reflects the level of left atrial pressure and hence pulmonary capillary pressure, with consequences for the lung blood–gas barrier24; the other was right ventricular systolic function, as assessed by right ventricular long axis excursion on echocardiography, which depends on several factors including afterload—that is, the level of pulmonary vascular resistance and hence the abnormality of the lung interstitial space.26
The knowledge of interactions between pulmonary haemodynamics and structure and function of alveolar–capillary membrane and airways, and their variations induced by pharmacological or non-pharmacological interventions, may have clinical relevance. Puri and colleagues recently showed that acute intravascular expansion impairs alveolar–capillary membrane function and increases airflow obstruction (the latter probably through engorgement of bronchial vessels and bronchial hyperresponsiveness) in patients with left ventricular dysfunction, in comparison with normal subjects27; it has also been reported that the inhalation of a vasoconstrictor drug such as methoxamine, or a bronchodilator agent such as salbutamol or ipratropium bromide, reduces bronchoconstriction and improves exercise capacity28-30; however, this effect has not been confirmed by other investigators.31 Furthermore, Guazzi and colleagues showed that in heart failure patients treatment with the ACE inhibitor enalapril caused improvement in DLCO, and particularly in the membrane component of DLCO, independently of changes induced in the resting haemodynamic profile; the increase in peakV˙o 2 observed in their patients with enalapril correlated with the change induced in DLCO.32 ,33 On the other hand, the same investigators recently reported that chronic treatment with carvedilol, a β adrenergic blocking agent, resulted in an improvement in left ventricular function but did not reverse pulmonary dysfunction in heart failure patients, and it also improved exercise performance.34 The hypothesis that treatment directed at correcting lung impairment might determine an increase in exercise capacity requires further study.
The reduction in MIP and MEP, expressed as per cent of normal predicted values, and the significant correlation with peakV˙o 2 observed in our patients support the hypothesis that abnormalities of respiratory muscle function might reflect a generalised involvement of skeletal muscle as a result of chronic heart failure,21 and might contribute, at least in part, to the peripheral limitation of exercise tolerance of heart failure patients.6 Interestingly, it has recently been reported that selective respiratory muscle training enhances submaximal and maximal exercise capacity and decreases the subjective sensation of dyspnoea during daily activities in heart failure patients.35 This finding has obvious clinical relevance.
STUDY LIMITATIONS
First, we did not measure the two components of DLCO separately—that is, the membrane diffusing capacity and pulmonary capillary blood volume. As a result, it was not possible to state which factor was responsible for the reduction in DLCO observed. However, diffusion through the alveolar–capillary membrane and capillary volume usually modify DLCO in opposite ways, the former reducing it and the latter increasing it; furthermore, in treated patients with heart failure the pulmonary capillary blood volume has been found to be normal or even increased, compared with normal subjects11 ,23 ,30; thus a low DLCO indicates an even larger reduction in membrane diffusing capacity.
Second, we did not evaluate changes in pulmonary functionduring physical activity. Smith and colleagues recently reported that DLCO increases during exercise both in normal subjects and in patients with heart failure, but the increase observed was significantly less in heart failure36; this may have pathophysiological importance and therapeutic relevance.
Finally, in this study we did not consider several other factors potentially contributing to exercise tolerance of heart failure patients, such as abnormalities of the peripheral circulation, skeletal muscle metabolism and contractile protein composition, impairment of reflex activity, altered left ventricular diastolic filling, and reduced right ventricular systolic function. These seem to account for more than 60% of the variance in peak exerciseV˙o 2 that remains after lung function abnormalities have been taken into account.
Acknowledgments
We wish to thank Dr Marco Guazzi, University of Milan, Italy, for his invaluable editorial assistance.