Article Text

Abstract
OBJECTIVE To assess the feasibility of measuring left atrial (LA) function with acoustic quantification (AQ) and then assess the effects of age and sex on LA reservoir, conduit, and booster pump function.
PATIENTS AND SETTING 165 subjects without cardiovascular disease, 3–79 years old, were enrolled by six tertiary hospital centres.
INTERVENTIONS Continuous LA AQ area data were acquired and signal averaged to form composite waveforms which were analysed off-line.
MAIN OUTCOME MEASURES Parameters of LA performance according to age and sex.
RESULTS Signal averaged LA waveforms were sufficiently stable and detailed to allow automated analysis in all cases. An age related increase in LA area was noted. LA reservoir function did not vary with age or sex. All parameters of LA passive and active emptying revealed a significant age dependency. Overall, the passive emptying phase accounted for 66% of total LA emptying ranging from 76% in the youngest to 44% in the oldest decade. LA contraction accounted for 34% of atrial emptying in all subjects combined with the older subjects being more dependent on atrial booster pump function. When adjusted for atrial size, there were no sex related differences in LA function.
CONCLUSIONS LA reservoir, conduit, and booster pump function can be assessed with automated analysis of signal averaged LA area waveforms. As LA performance varies with age, establishment of normal values should enhance the evaluation of pathologic states in which LA function is important.
- aging
- atrium
- echocardiography
Statistics from Altmetric.com
Left atrial (LA) performance is complex and includes functioning as a reservoir, conduit, and booster pump at different stages of the cardiac cycle. Abnormalities of LA performance are clinically important and found in a wide variety of common clinical conditions such as atrial fibrillation, dilated cardiomyopathy, diastolic dysfunction, and valvar heart disease.1-5 Detailed evaluation of LA function has been performed using a variety of invasive methods which combine LA pressure with volume measurement to generate pressure-dimension loops.6 ,7 This approach is limited by the need for direct LA pressure recordings which precludes routine clinical use.
The most commonly used non-invasive technique to evaluate LA performance is Doppler echocardiography. However, Doppler echocardiography is limited since it provides no information about LA size and, although the use of this technique to evaluate LA booster pump function has been described, it is not suitable for the assessment of the reservoir and conduit phases of LA function. Measurement of LA size at different phases of the cardiac cycle has proven to be useful for evaluating LA performance. However, the assessment of LA volume by two dimensional (cross sectional) echocardiography requires tedious hand tracing of endocardial borders.
Acoustic quantification (AQ), an automated border detection technique, provides on-line continuous cardiac chamber area or volume over time and has been used extensively to study the left ventricle.8-10 Individual AQ waveforms can be noisy due to random and physiologic variations, but the use of signal averaging of AQ waveforms reduces this variation.11 Initial studies applying AQ to the LA chamber have not used signal averaging and additionally have been limited by the need to identify manually the different cardiac phases which is tedious and subjective.4 ,5 ,12-14 Although abnormalities in disease states such as hypertension and atrial fibrillation have been demonstrated with this technique, the small number of normal subjects has limited systematic conclusions about these findings. Before evaluating LA reservoir, conduit, and booster pump function in pathologic states, a thorough understanding of LA physiology as assessed by AQ in a large group of normal subjects over a wide age range is essential.
This study sought to: (1) assess the feasibility of measuring LA reservoir, conduit, and booster pump function with computer automated analysis of signal averaged LA area waveforms; (2) assess the effects of age and sex on LA reservoir, conduit, and booster pump function; and (3) establish normal values for parameters of LA performance as determined from AQ.
Methods
SUBJECTS
One hundred and seventy one subjects (81 males and 90 females) aged 3–79 years old were enrolled from six participating centres. Subjects were required to have a transthoracic window adequate for performing automated border detection. Entry criteria included: (1) no clinical history of cardiovascular disease; (2) normal sinus rhythm; (3) absence of left bundle branch block; (4) normal blood pressure; (5) absence of wall motion abnormality on two dimensional echocardiographic screening; (6) no more than trivial aortic insufficiency or mild mitral, tricuspid or pulmonic regurgitation; (7) normal left ventricular mass determined using the area–length formula; (8) ejection fraction of ⩾50% calculated from manual tracings of end systolic and end diastolic frames using the method of discs.
ACOUSTIC QUANTIFICATION
AQ is an automated online technique that analyses the ultrasound backscatter to identify the blood–tissue interface of cardiac chambers and generate area or volume waveforms within a defined region of interest.8-10 Using a SONOS 5500 (Hewlett Packard, Andover, Massachusetts, USA) images were obtained from the apical four chamber window taking care to maintain a non-foreshortened, maximally sized view of the left atrium. The automated border detection system was activated and optimised, as previously described,15 by adjusting the total gain, time gain compensation, and lateral gain. A region of interest was then drawn around the left atrium excluding the pulmonary veins. The LA area waveform was displayed and visual confirmation of consistent stable waveforms made (fig 1). Forty five seconds of LA area versus time data were acquired to magneto-optical disk. All acquisitions were made during quiet respiration without breath holding.

Apical four chamber view with acoustic quantification activated and optimised for the left atrium. The bottom of the figure shows the LA AQ area waveform (green).
ANALYSIS
All atrial AQ waveforms were analysed off-line using custom software. All 45 seconds of LA waveform data were signal averaged resulting in a single composite waveform. Signal averaging reduces noise and variability of the AQ waveforms.11 From this signal averaged waveform the first derivative of LA area was computed. The custom software automatically identified the phases on the LA waveform using morphologic criteria of the area and derivative curves. The minimum area (LAmin), maximum area (LAmax), and the area at the onset of atrial emptying (LAoae) were then determined (fig2).

Signal averaged AQ LA area (top) and LA derivative (middle) waveforms. Left ventricular (LV) volume waveforms (bottom) are shown for reference. The phases of the cardiac cycle are labelled: R, reservoir; C, conduit; B, booster pump; LAmin, minimum area; LAmax, maximum area; LAoae, onset atrial emptying area; PFR, peak filling rate; PPER, peak passive emptying rate; PAER, peak active emptying rate.
LA reservoir function was assessed using filling area (LAmax − LAmin), expansion index (LAmax − LAmin)/LAmin*100, and the peak rate of filling (PFR). The overall diastolic emptying index was calculated as (LAmax − LAmin)/LAmax*100. LA conduit function was assessed by calculating: the passive emptying percentage of total emptying (PE) = (LAmax − LAoae)/(LAmax − LAmin)*100, passive emptying index (PEI) = (LAmax − LAoae)/LAmax*100, and peak passive emptying rate (PPER). Parameters of atrial booster pump function included: active emptying percentage of total emptying (AE) = (LAoae − LAmin)/(LAmax − LAmin)*100, active emptying index (AEI) = (LAoae − LAmin)/LAoae*100, and peak active emptying rate (PAER). All area derivative peak rates were expressed in absolute units (cm2/s) and normalised by the maximum atrial area (LAmax/s).
STATISTICAL ANALYSIS
Subjects were grouped by decades for comparison. Normally distributed variables were expressed as mean and standard deviation and non-normally distributed variables as median and interquartile range. Analysis of variance was performed to assess for age related changes in AQ parameters of LA function. Non-normally distributed parameters were compared with a Kruskal-Wallis test. Values for male and female subjects were compared with an unpaired ttest. A probability value of p < 0.05 was considered significant.
Results
LA AQ data acquired in 6/171 subjects were unusable because of inadequate ECG tracings which prevented signal averaging. The age distribution of study subjects is shown in table 1. The signal averaged LA waveforms were sufficiently stable and detailed to allow automated analysis in all cases. The normal values of all LA area AQ parameters are presented by age and sex in tables 1 and2.
Normal values for AQ LA
Sex differences in AQ LA parameters
The general morphology of the LA area waveforms revealed an increase in area during ventricular systole (reservoir phase) followed by three diastolic stages. The initial diastolic portion of the LA area waveform was noted to have a rapid decline in area (conduit phase) followed by a period of relative stable area (diastasis) and, finally, a second rapid area decline occurring during atrial contraction (booster pump phase). The LA derivative waveform demonstrated peaks during the reservoir, passive, and booster pump phases. The diastolic phase of the LA area derivative curve has a morphology similar to that of Doppler mitral inflow, as the rate of change in LA size is proportional to transmitral blood flow.
ATRIAL SIZE
The average values for LA size are shown in table 1. Age related differences in LA area were noted. The youngest subjects had smaller LA minimum, maximum, and onset atrial emptying areas. From the third to the seventh decade no significant change in LA areas were noted; however, subjects in the oldest decade had increased LA sizes. This increase in LA area in the eighth decade was not accounted for by differences in body surface area. Male subjects had statistically larger LAmax and LAoae compared to female subjects (table 2). However, after accounting for differences in body surface area, there were no sex related differences in indexed LA areas.
LEFT ATRIAL FUNCTION
LA reservoir function, assessed by the area change during LA filling and the peak rate of atrial filling, was reduced in the first two decades of life and then remained unchanged during adult life (table 1). However, when the peak rate of atrial filling was normalised for LA size by dividing by the maximum area, no age related changes in LA reservoir function were noted. Overall, the LA expanded 83% during ventricular filling with a wide spread in this parameter (range 30–560%) caused by the variation in minimum LA areas. The systolic expansion index did not vary with age. Male subjects had larger area changes and peak rates of filling that were rendered insignificant when the larger male LA areas were controlled for.
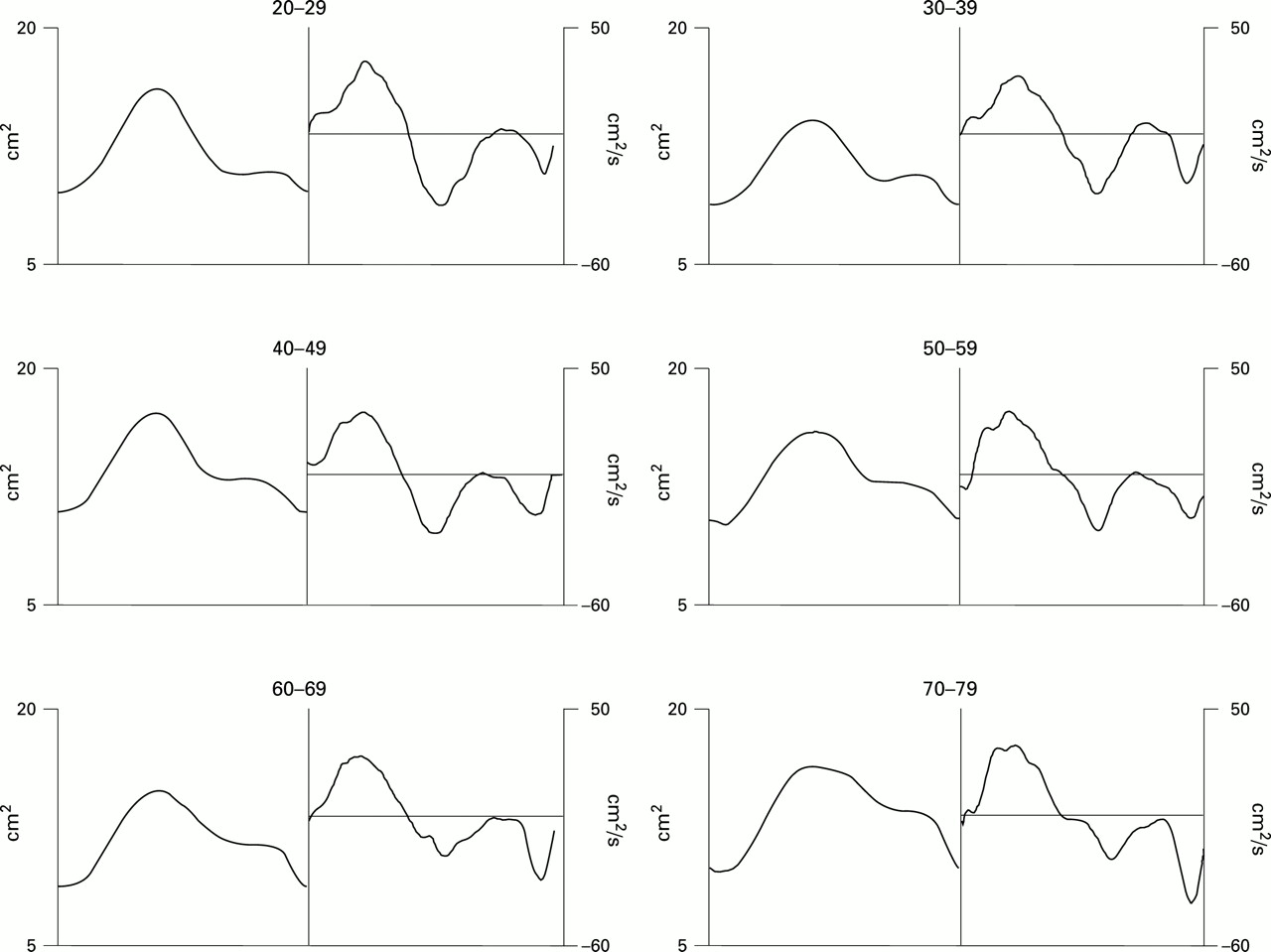
No age related difference in the overall diastolic emptying index was noted. When diastolic LA emptying was divided into passive and active components all AQ parameters revealed a significant age dependency (table 1). These changes are visually apparent when viewing composite LA waveforms generated for each decade of adult life (fig 3). The age related changes in AQ parameters of LA diastolic emptying persisted after accounting for age related changes in heart rate.

Composite LA waveforms generated by time normalising and averaging 10 subjects from each decade. There is an obvious morphologic change in the LA area and derivative waveform from the third to the eighth decade of life. Note the progressive decline in passive emptying and augmented active atrial booster pump function with age.
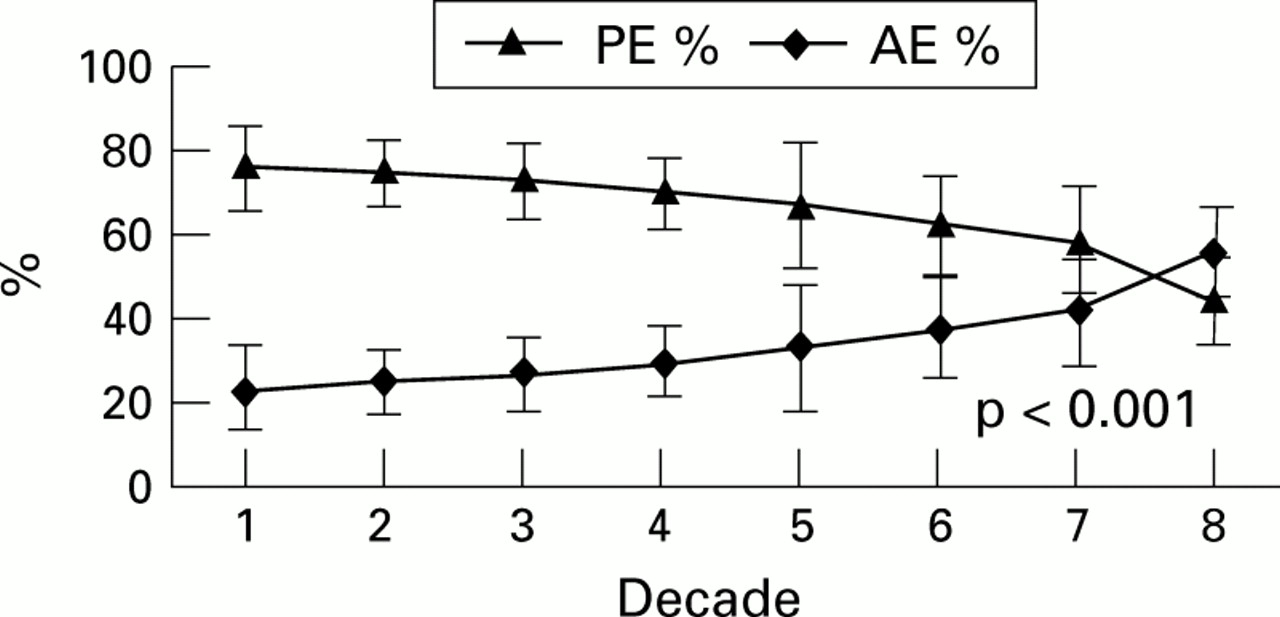
Overall, the passive phase accounted for 66% of total LA emptying. The contribution toward left ventricular (LV) filling of passive LA emptying was significantly decreased in the older three decades, reaching a low of 44% in subjects in the eighth decade (fig 4). Passive LA emptying appeared reduced in the youngest and oldest decades when assessed by the peak rate of passive emptying. However, after normalisation for LA size, this difference persisted only for the oldest subjects. LA passive function was also reduced in the oldest decade studied when measured as the passive emptying index. When adjusted for atrial size, there are no sex related differences in LA passive function.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Age related changes in the passive and active contributions to total LA emptying in normal subjects.
LA contraction accounted for 34% of atrial emptying in all subjects combined. The older three decades were more dependent on the atrial booster pump to complete LV filling compared to younger subjects as demonstrated by a larger contribution of atrial contraction to overall atrial emptying (fig 3). The peak rate of atrial emptying was reduced in the youngest subjects, but this was eliminated after correction for their smaller atrial areas. The peak atrial emptying rate and atrial emptying index were dependent on age, but when grouped by decades there were no differences compared to the third decade of life. When adjusted for atrial size, there were no sex related differences in LA booster pump function.
Discussion
ASSESSMENT OF LEFT ATRIAL FUNCTION
Although sophisticated techniques have been used to assess LA function,1 ,6 ,16 these methods require invasive determination of LA pressure to generate pressure–dimension loops. Several modalities such as nuclear scintigraphy and angiography have been used to assess LA performance by measuring changes in LA volume over time.17 ,18 These techniques are limited by their expense, low temporal resolution, geometric assumptions, the need for contrast or radiopharmaceutical agents, and cumbersome acquisition. Hand drawn LA areas from two dimensional echocardiographic images are easier to acquire and have demonstrated abnormalities of LA function in patients with hypertension and dilated cardiomyopathy.2 ,19-22 Manually traced two dimensional echocardiographic LA areas are limited by poor temporal resolution (typically 2–3 area values per cardiac cycle) and tracing of LA endocardial borders on a frame-frame basis is labour intensive and tedious.
Doppler echocardiography has also been used to evaluate LA function. Several reports have suggested using pulmonary venous systolic flow as an indicator of LA reservoir function.23 ,24 The peak velocity of mitral inflow during atrial contraction together with the atrial filling fraction have been used as non-invasive markers of LA booster pump function.25 ,26 These mitral inflow Doppler indices, however, provide no information on atrial size or reservoir and conduit function. Pulsed wave Doppler can be combined with mitral orifice area to compute LA ejection force27; however, this parameter likewise only assesses LA active contractile function.
AQ provides LA area measurements throughout the cardiac cycle and, unlike other techniques, can be used to assess non-invasively LA size as well as the reservoir, conduit, and booster pump function of this chamber. The LA border determined with the AQ algorithm has fine irregularities; these average out, however, to provide an accurate estimation of LA area compared to hand drawn measurements.7 ,12 ,14 Although AQ of the LA has previously been combined with LA pressure measurements to assess LA function,3 ,7 ,13 ,28 this remains primarily a research technique.
LA AQ has been used to evaluate LA performance in atrial fibrillation, postcardiac transplant, and other cardiac pathologic states.4 ,5 ,12 ,14 In addition, LA AQ has shown promise as an adjunct to Doppler echocardiography for the assessment of diastolic dysfunction in hypertensive patients.29 However, these early studies have been limited by the small number of subjects and lack of systematic comparison of all components of LA performance with a normal age matched reference population. In addition, these initial reports are hindered by the use of single LA waveforms, which demonstrate beat to beat variability, as well as the need for subjective manual analysis of these waveforms.
This study showed that continuous LA area waveforms could be signal averaged to reduce noise and variability, allowing automated detection and detailed analysis of the different phases of LA function. These signal averaged area waveforms also provide more reliable area derivative waveforms which provide additional parameters of LA performance. LA reservoir function, which reflects the ability of the LA to fill during ventricular systole, has been difficult to assess non-invasively. AQ allowed calculation of several parameters of LA reservoir function. The expansion index of 83% is similar to the previously reported values of 81% and 99% in smaller studies.5 ,12 Atrial conduit and booster pump function likewise were also quantitatively assessed with several automatically computed parameters. On average, this study demonstrated that 66% of atrial emptying occurs during the passive phase whereas 34% occurs during atrial contraction. The peak rate of emptying during the conduit phase is higher than that of the booster pump phase, and averages 1.7 times that of peak active emptying.
AGE DEPENDENCY OF LEFT ATRIAL SIZE AND FUNCTION
An age related increase in LA size has been noted previously using two dimensional echocardiography.20 Wang and colleagues, however, did not note an increase in LA size with age30but that study only included subjects under age 65, which is consistent with our results demonstrating no change in atrial size until the eighth decade. No prior reports have assessed the age related changes of all aspects of atrial performance in a large group of normal subjects. These age related changes are qualitatively apparent when inspecting the LA area waveforms from the different decades of life (fig 3). This study provides normal values of LA AQ parameters, which quantify these physiologic changes that occur in the LA area waveforms over age.
The use of AQ allowed calculation of several parameters reflecting the reservoir function of the LA. These parameters remained stable over the six decades of adult life evaluated in this study. The preserved LA expansion during the reservoir phase is important to maintain adequate LV filling. As the mitral valve is closed during ventricular systole, LA pressure is determined by both the magnitude of LA filling and atrial compliance. By maintaining LA filling, the early diastolic atrioventricular gradient required to fill the LV during passive filling is preserved. In addition, preserved atrial filling helps maintain the LA size at the onset of atrial contraction (atrial preload) which also augments LV filling.
In contrast to atrial filling, the characteristics of atrial emptying change with age. This study demonstrated a decline in LA passive emptying with age in normal subjects. This likely represents an age related change in LV properties leading to diastolic dysfunction which impairs passive atrial emptying during early diastole. However, there is an increase in atrial booster pump function with age which compensates for the decrease in early diastolic filling. This finding has been previously recognised using Doppler echocardiography.31-33 The observed augmentation in LA contractile function may be in part mediated via a Starling effect, as this study has demonstrated atrial size at the onset of LA contraction (atrial preload) is larger in older subjects. LA size at the onset of atrial contraction is a major determinant of LA ejection force.20 The passive and active emptying indices of 32% and 23% are different than previously reported (25% and 26%)5 but this is likely due to the older age range in that study (31–63 years old).
LIMITATIONS
Not all subjects can be evaluated with this technique since automated border detection, similar to other ultrasound based imaging techniques, requires an adequate two dimensional image. However, in our experience 85% of subjects have adequate windows to obtain LA AQ waveforms. The patients studied did not represent a true random selection of the general population. Although the analysis in this study was performed off-line, the signal averaging and automated analysis have been recently incorporated into a prototype ultrasound system (HP SONOS 5500) to provide on-line evaluation of LA performance.
CONCLUSIONS
The results of this study, obtained in a large group of normal subjects, demonstrated that LA reservoir, conduit, and booster pump function can be assessed with automated analysis of signal averaged LA area waveforms. These results also demonstrate that LA performance, as assessed by AQ, varies with age. This age dependency has important implications for future studies involving LA pathophysiology whether based on AQ or other modalities. The normal values established in this study should enhance the evaluation of pathologic states in which LA function is assessed with AQ.