Article Text

Abstract
OBJECTIVE To investigate whether viral infection acts as a trigger factor for the development of dilated cardiomyopathy in genetically predisposed individuals with a family history of disease.
SETTING Patients attending the cardiomyopathy unit in a cardiac tertiary referral centre.
DESIGN Nested polymerase chain reaction (nPCR) was used to determine whether enteroviral, adenoviral, or cytomegaloviral nucleic acids were detectable in the myocardium of 19 asymptomatic relatives of patients with dilated cardiomyopathy; all these relatives had echocardiographic abnormalities thought to represent early disease. Explanted hearts from patients with end stage dilated cardiomyopathy were also studied and were compared with 25 controls (ischaemic heart disease (21), valvar heart disease (2), hypertrophic cardiomyopathy (1), restrictive cardiomyopathy (1)). Myocardial tissue from two fatal cases of culture positive coxsackie myocarditis was used as a positive control.
RESULTS No viral nucleic acid was detected in any group other than in those with myocarditis. Spiking of random wells with purified recombinant viral nucleic acids confirmed the sensitivity and reproducibility of the assays.
CONCLUSIONS Myocardial viral infection is not detectable in relatives of patients with dilated cardiomyopathy who are suspected of having early disease. There is no evidence that viruses act as a trigger factor for initiating the dilated cardiomyopathy in these patients.
- viral infection
- dilated cardiomyopathy
Statistics from Altmetric.com
Dilated cardiomyopathy has an annual incidence of 5–8/100 000 and a prevalence of 40/100 000.1 It accounts for up to 50% of indications for heart transplantation. At the time of diagnosis, the disease is often advanced, with up to 90% of patients being in New York Heart Association (NYHA) class III/IV heart failure.2Partly because of this, the pathogenesis is poorly understood. There has been much interest in viruses as possible causative agents in dilated cardiomyopathy, especially enteroviruses and more recently adenoviruses.3-19
The mechanism whereby a common viral infection might cause cardiac disease in a select population is unknown. Studies in mice have shown that not all strains of coxsackie viruses are cardiovirulent.20 Alternatively, host factors may determine susceptibility, as shown by the variable susceptibility of specific murine strains.21 In prospective studies in man it has been found that dilated cardiomyopathy may be familial in up to 50% of cases. While various mutations involving cytoskeletal or nuclear envelope proteins have been identified as being aetiological, in the majority of cases the cause remains unknown and viral infection in genetically predisposed individuals cannot be excluded. Furthermore, there is evidence of inflammatory mechanisms in the pathogenesis of familial disease, including an HLA association22 and the presence of circulating organ and disease specific cardiac antibodies.23
If infection initiates disease, the timing of the investigation may be critical, as ongoing damage may not depend on the persistence of virus. However, early investigation is often not feasible, especially when the condition is advanced at the time of presentation. Prospective family studies in which asymptomatic relatives are evaluated provide a unique opportunity to study early disease. In such studies 10% of relatives are found to have left ventricular enlargement, defined as a left ventricular diastolic diameter of more than 112% of that predicted for age and body surface area by Henry's formula,24 with preserved systolic function. The hypothesis that left ventricular enlargement may represent an early stage of dilated cardiomyopathy was borne out by a follow up study by Baig and colleagues,25in which 30% of these patients developed symptomatic dilated cardiomyopathy over a three year period. If viral infection causes familial dilated cardiomyopathy through a mechanism of genetic predisposition, this should be detectable in relatives with left ventricular enlargement.
Our aim in this study was to determine whether enteroviral, adenoviral, and human cytomegalovirus infection initiates dilated cardiomyopathy in genetically predisposed individuals and whether these agents persist to the time of transplantation.
Methods
PATIENTS STUDIED
Early disease
We studied right ventricular biopsies from 19 patients with left ventricular enlargement who had a family member with dilated cardiomyopathy.26 Evaluation of asymptomatic relatives was done with local ethics committee approval and has been described in detail elsewhere.25
Left ventricular enlargement was defined as an unexplained left ventricular end diastolic dimension (LVEDD) of more than 112% of predicted values in the presence of a shortening fraction of more than 25%. Predicted left ventricular end diastolic dimension (LVEDDc) was calculated using Henry's formula24: LVEDDc = [45.3 × BSA0.3]− [0.03Age] − 7.2, where BSA = body surface area (m2) and age is in years. The measured LVEDD was then expressed as a percentage according to the ratio: LVEDD% = LVEDD/LVEDDc.
Exclusion criteria were the same as for the patients with dilated cardiomyopathy. Prognosis varied between the families. None of these 19 patients came from families in which premature conduction disease, clinical skeletal myopathy, non-compaction, or sensory neural deafness was a recognised manifestation of the phenotype. The genetic aetiology was unknown in these patients.
End stage dilated cardiomyopathy
Explanted hearts from 24 patients with end stage dilated cardiomyopathy—21 with ischaemic heart disease, two with valvar disease, one with hypertrophic cardiomyopathy, and one with restrictive cardiomyopathy—were studied for the presence of viral nucleic acids. Dilated cardiomyopathy was defined according to World Health Organization criteria,26 excluding patients with coronary artery disease, hypertension, valvar heart disease, or a regular alcohol intake of more than 21 units/week in men and more than 14 units/week in women.
The hearts were obtained from consecutive transplants performed over a period of three years. Pedigree information was not available in these patients. The inclusion of the end stage dilated cardiomyopathy explants in this study served to broaden the message of the presence or absence of viral infection in both early and late stages of the disease. We only included hearts collected immediately after transplantation and we did not use any hearts that had been investigated before.7
Patients with myocarditis
Two cases of coxsackie virus B3 (CVB3) culture positive myocarditis—a 10 day old infant and a 6 month old infant—who had died of myocardial dysfunction were included as positive controls.
PROCEDURES
Myocardial biopsy
A programme to perform endomyocardial biopsy as part of the evaluation of relatives with left ventricular enlargement received local ethics committee approval. Following informed consent, patients and relatives had a fluoroscopically guided right ventricular biopsy through the right internal jugular vein. For polymerase chain reaction (PCR) studies, the tissue obtained was snap frozen immediately in liquid nitrogen. Specimens for histological analysis were stored in formalin or snap frozen in OCT (Merck, Leicester, UK) in a cryo mould.
Immunohistochemistry
Cryostat sections (4 μm) were first fixed in acetone and then incubated with mouse monoclonal antibodies to CD3. Affinity purified biotinylated goat antibodies to mouse immunoglobulin G (Southern Biotechnology, Birmingham, Alabama, USA) were then applied, followed by fluorescein isothiocyanate conjugated streptavidin. A nuclear stain (propideum iodide) was added. The number of CD3 positive cells present in the tissue per unit area was counted with a Zeiss Aioplan photomicroscope with ultraviolet epi-illuminator. For biopsies, the whole of the tissue area was counted. For samples taken from explanted hearts, randomly selected fields (square microns in area) were counted until a stable number of CD3 positive cells per field was obtained.
Extraction of nucleic acids and PCR amplification
Using sterile cutting equipment, 2–3 mm2 samples were cut from the left ventricle and the septum of explanted hearts immediately after transplantation and frozen at −80°C. Tissue obtained from suspected cases of myocarditis was processed in a separate facility. To extract RNA, the frozen samples were homogenised on ice in Trizol (Gibco-BRL, Paisley, UK) using RNAse-free disposable pestles, and processed according to manufacturer's instructions. RNA extraction from biopsied material was carried out using Glassmax RNA isolation kit (Gibco-BRL). DNAzol (Gibco-BRL) was used for DNA extraction from cardiac tissue.
Reverse transcription (RT) was carried out using the superscript-II kit and random hexamers (Gibco-BRL). After cDNA synthesis, the superscript was inactivated and the RNA template treated with 1 μl of Escherichia coli RNAse H. Nested PCR was carried out using taq polymerase (Gibco-BRL) in a hot start reaction. A 2 μl sample of product from the first round of amplification was used as a template for the nested reaction. The primers used for PCR detected a wide spectrum of coxsackie B virus serotypes,9 including B2, B3, B5, B11, and B30. Primer sequences and the reaction conditions are shown in table 1. Samples found positive in the nPCR reaction were subjected to sequencing using Big Dye Tm Terminator cycle sequencing kit (PE Applied Biosystem, Warrington, UK) on ABI PRISM automated sequencing system. Amplification of cytomegalovirus and adenovirus sequences was carried out separately as nested PCR reactions, using the primers and conditions described in table 1. The primer sets used for adenovirus nested PCR27were specific for 18 different serotypes of the virus, and those used for cytomegalovirus nested PCR were designed to amplify sequences from the UL83 region of the genome (accession No x17403).
Primer sequences and reaction conditions used for amplification of viral and myoglobin sequences (Y = C + T)
The positive controls used for the enterovirus PCR included RNA extracted from culture grown CVB3 as well as from CVB3 infected murine hearts. The latter was a generous gift from Professor Bernhard Maisch (department of internal medicine-cardiology, University of Marburg, Marburg, Germany), donated as part of a collaborative international study on standardisation of enteroviral nucleic acid detection strategies. A third positive control used was a dilution of a plasmid (pBlue Script) containing the complete cDNA sequence for CVB3. The plasmid was donated by Dr R Kandolf (department of pathology, University of Tubingen, Tubingen, Germany) and was used at dilutions containing 5 and 0.5 copy numbers of viral nucleic acid per reaction tube. Positive controls were the AD169 strain of cytomegalovirus and adenovirus dl309, cultured in human embryo lung fibroblasts (HELF). Amplification of the recombinant ppUL83 gene of cytomegalovirus from pMV100 vector construct at 100 and 10 gene copies per reaction, and of the adenovirus vector pJM1728at 10 and 5 gene copies per reaction was also done. All positive samples were handled in a separate laboratory, but amplified alongside the human hearts in the same thermocycler.
Negative controls included RNA and DNA extracted from uninfected HELF, as well as murine hearts and reaction tubes containing no nucleic acids. The myoglobin gene was used as the housekeeping gene to assess the success of the nucleic acid extraction and reverse transcription. Primers used for amplification were derived from exons 1 and 3 of the gene.29
Results
The mean (SD) age of asymptomatic relatives undergoing biopsy was 29.7 (13.7) years. Eleven were male and eight female. Twelve of the relatives were from 10 families that fulfilled WHO criteria for familial disease, and seven were non-familial by these criteria. Left ventricular end diastolic dimension was 62 (2.8) mm, representing 117.5 (4.4)% of that predicted by the formula of Henry and colleagues,25 and fractional shortening was 31.1 (4.9)%. Histopathological examination of the biopsy samples showed features consistent with dilated cardiomyopathy in five cases. With less than 14 CD3 positive cells/mm2 tissue, there was no evidence of myocarditis in any of the familial samples examined.
We studied 49 patients who received heart transplants at St George's Hospital: 24 cases of dilated cardiomyopathy, 21 of ischaemic heart disease, two of valvar disease, one with restrictive cardiomyopathy, and one with hypertrophic cardiomyopathy. The mean (SD) age of the patients with dilated cardiomyopathy was 41.2 (8.1) years, and of the controls, 50.1 (5.7) years. There were no differences between patients and controls with respect to NYHA class (median 3), left ventricular end diastolic dimension (71 mm v 73 mm), or fractional shortening (12.2% v 12.4%). There was no evidence of myocarditis in any of the dilated cardiomyopathy samples examined.
Nested enteroviral RT-PCR was performed on left ventricular and septal tissue obtained from the explanted hearts and on 19 biopsies obtained from patients with familial early dilated cardiomyopathy. None of the samples was found to carry viral sequences (fig 1A). Sequences consistent with the presence of CVB3 were identified in neonatal heart tissues obtained from two cases of culture positive, enterovirus associated deaths. In all 98 explant samples and 19 biopsies studied, a positive myoglobin RT-PCR confirmed the presence of intact RNA and verified that successful reverse transcriptions had taken place (fig1B).

(A) Nested enteroviral reverse transcription polymerase chain reaction (PCR), performed on left ventricular and septal tissue obtained from explanted hearts and biopsies taken from patients with familial early dilated cardiomyopathy. Representative data are shown in lanes 9 to 14. Other lanes are: culture grown coxsackie virus B3 (CVB3; lane 2), CVB3 infected mouse heart (lane 3), 5 and 0.5 copies of pBlue script plasmid carrying CVB3 cDNA (lanes 4 and 5, respectively), and CVB3 infected human hearts (lanes 15 and 16); molecular weight markers are shown in the first and last lanes; reagent contamination controls from first and second rounds of PCR amplification are shown in lanes 7 and 8, respectively; an uninfected mouse heart used as negative control is shown in lane 6. (B) Amplification of the myoglobin housekeeping gene following reverse transcription. The order of samples as for panel (A).
As the abundance of the myoglobin gene is very high compared with the lower copy numbers of viral nucleic acids that may be present in cardiac tissue, the sensitivity of the nested RT-PCR was tested with selected positive controls. This was done to ensure that the negative findings were not caused by low detection sensitivities. Routine controls included cell culture grown CVB3 as well as an infected murine heart. These were tested at limiting dilutions such that positive findings were only obtained after a nested reaction (fig 1A). In addition, a plasmid construct containing CVB3 cDNA at 5 and 0.5 copy numbers per reaction tube was included as control. The sample containing 5 copies of CVB3 cDNA was consistently positive but that with 0.5 copies produced sporadic positives. Detection of such low copy numbers of the plasmid also confirmed that treatment of cDNA samples with RNAse H following complementary strand synthesis did not affect the sensitivity of the PCR reactions. Negative control samples included uninfected mouse hearts processed alongside the human tissue. To check for contamination of the reagents and compliance with clean procedures, negative controls containing water instead of RNA were also included in each run. The assays were consistently sensitive and no contamination occurred during the period of this study.
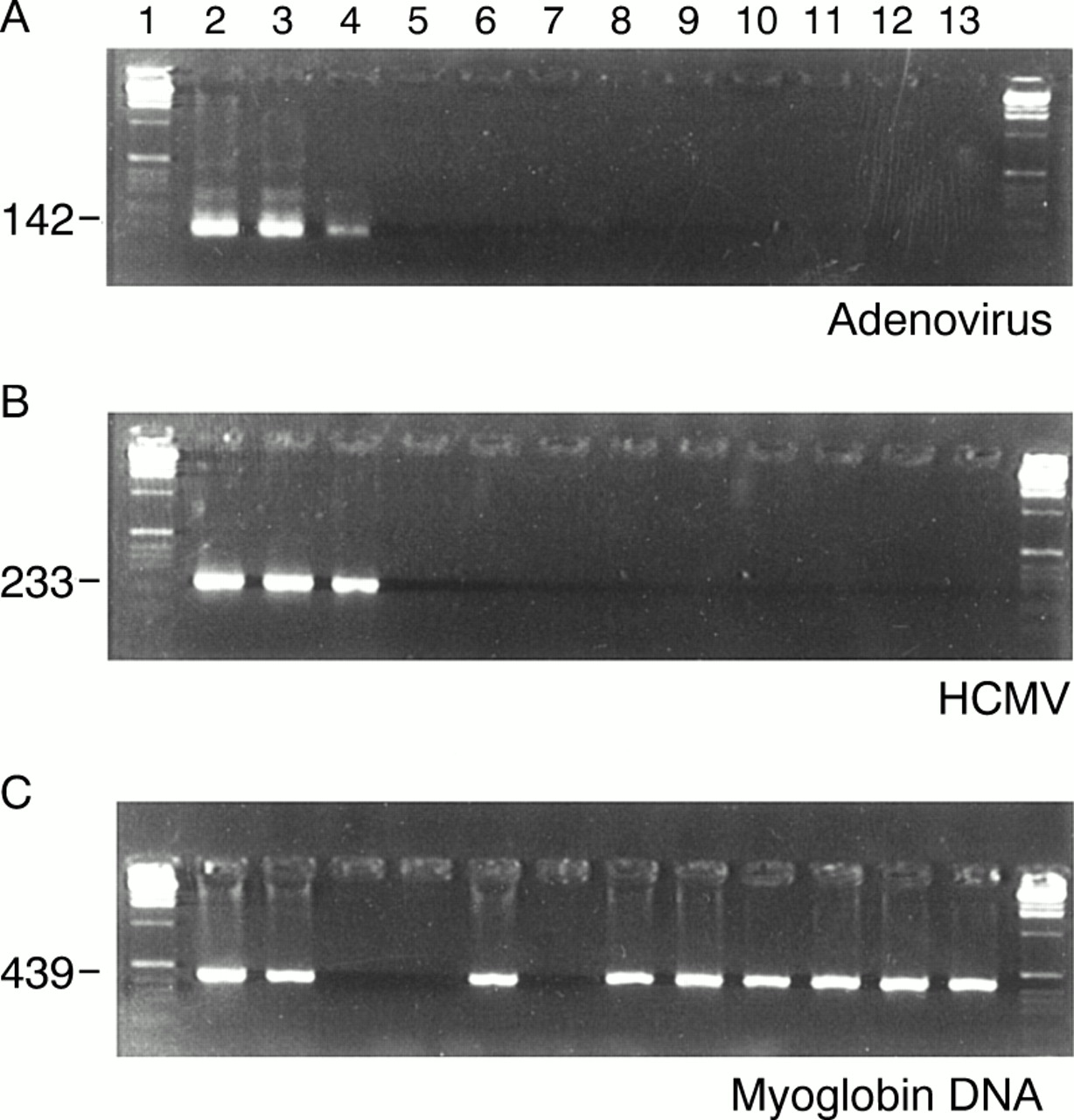
DNA samples obtained from the explanted hearts and early dilated cardiomyopathy biopsies were tested in nPCR for the presence of adenoviral and cytomegalovirus sequences. Multiplex procedures were avoided. No viral nucleic acids were detected in the 117 samples analysed (fig 2A). The presence of intact DNA was confirmed by successful amplification of the myoglobin gene in all the samples tested (fig 2C). Positive controls included cell culture grown virus used at dilutions such that positive signals were only seen after the second round of amplification. To assess the sensitivity of the cytomegalovirus nPCR, we used a plasmid (pMV100) constructed in our laboratories, carrying the coding sequence for the ppUL83 protein of cytomegalovirus.27 Ten copies of the plasmid construct were consistently detectable when used as a spike in nRCR assays (fig2B). An adenovirus plasmid vector, pJM17,28 was used as spike to assess sensitivity of the adenovirus nPCR. Dilutions of the construct were tested and found to be consistently reactive at 5 copies per reaction (fig 2A).
{kind=link}
{kind=link}
(A) Nested polymerase chain reaction (PCR) amplification of adenovirus, performed on left ventricular and septal tissue obtained from explanted hearts and biopsies taken from patients with familial early dilated cardiomyopathy. Representative data are shown in lanes 8–13. Other lanes are: molecular weight markers in the first and last lanes; culture grown adenovirus (lane 2), 10 and 5 copies of plasmid pJM17 carrying adenovirus sequences used for sensitivity assessments (lanes 3 and 4, respectively), uninfected mouse heart (lane 5), reagent contamination controls for first and second round of PCR amplification (lanes 6 and 7, respectively). (B) Nested PCR amplification of human cytomegalovirus (HCMV). The order of presentation of samples is as for panel (A). Culture grown HCMV is shown in lane 2. The sensitivity controls used were 100 and 10 copies of the plasmid pMV100 carrying HCMV sequences (lanes 3 and 4, respectively). (C) Amplification of the myoglobin gene from DNA. Cardiac samples are shown in wells 8 to 13. Adenovirus and HCMV cell cultures are shown in wells 2 and 3, respectively. Uninfected murine heart is shown in well 6 and the reagent negative control in well 7. No samples were loaded in wells 4 and 5.
Discussion
Our aim in this study was to investigate viruses as trigger mechanisms for initiating dilated cardiomyopathy in predisposed individuals, and to look for the sustained presence of these agents in late disease. No evidence was found that patients harboured enteroviral, adenoviral, or cytomegaloviral nucleic acids in the myocardium at either early or late stages of the disease. The studies performed allowed repeatable amplification of small copy numbers of viral RNA or DNA, ensuring consistent sensitivity of the assays.
Prospective cardiovascular evaluation of over 700 asymptomatic first degree relatives from over 180 families at our institution has shown asymptomatic left ventricular enlargement in approximately 15% of cases. A significant proportion of these progress to overt dilated cardiomyopathy during follow up. As susceptibility to cardiotropic viral infection and subsequent immunological responses may be genetically determined, this provided a unique opportunity to study the relevance of infection in early disease. Immunohistochemical investigations in patients identified as having familial predilated cardiomyopathy were consistent with the presence of low grade inflammation. However, no viral nucleic acids were found in the myocardium. In addition, no data were available suggesting that any of these patients had, in the past, experienced an infection that might have triggered the myocardial inflammation. As with all infection related cases, the study would have been more informative if patients with end stage disease had been compared with their immediate relatives, but this is difficult to justify on ethical grounds.
The mechanisms whereby viruses, and in particular enteroviruses, may cause myocyte damage leading to dilated cardiomyopathy have been investigated,30-32 but there is disagreement about the chronic presence of viral nucleic acids in the myocardium.
In meta-analyses of the reported cases, excluding studies without controls, enteroviral RNA in dilated cardiomyopathy was found in 12 studies,12 13 17 and adenoviral DNA in one.14 Among negative studies, in nine there were either no enteroviruses or equal proportions of cases and controls were infected.11 15 17 Where sequence analysis has been carried out, one group found that amplification products from all patients carried the same sequence,33 while others found that individual patients carried unique sequences.11-13 18 Such sequence comparisons have been verified as reliable means for ruling out contamination with laboratory control viruses.18 However, there is a possibility, albeit small, that in laboratories working with multiple variants of enteroviruses, contaminants may be genotypically different.
Negative studies have traditionally relied on the amplification of a housekeeping gene for control. This strategy does not exclude low sensitivity of PCR reactions. Consistent amplification of small copy numbers of viral nucleic acids in the present study confirms the sensitivity of the assays and validates the negative findings. This is in agreement with the data reported by Muir and colleagues,9 who found no association between enteroviruses and end stage dilated cardiomyopathy using an assay with a detection sensitivity of 10–100 copy numbers of viral RNA. Despite such sensitivities, consideration must be given to sampling errors that may occur. If the infected region of the heart is limited to a small area, large numbers of samples may need to be analysed to verify negative results.
In addition to technical difficulties, clinical considerations may influence results. A major determinant of whether viral persistence can be detected may be the time in the course of the disease at which the investigation is performed. In animal models of viral myocarditis, virus becomes progressively less detectable as disease advances.34 In man, Why and colleagues found that virus positive cases of dilated cardiomyopathy were of shorter disease duration than negative ones.19 This may partly explain the discrepancy between this study of explanted hearts in end stage dilated cardiomyopathy and work published by others showing the presence of adenoviral and enteroviral genome in individuals undergoing biopsy following a diagnosis of idiopathic left ventricular dysfunction.14
CONCLUSIONS
Using highly sensitive PCR procedures, no viral nucleic acids were detected in patients with either early or end stage dilated cardiomyopathy. Although the results obtained from this study may suggest that viruses do not play a pathological role in the initiation of disease in predisposed individuals with familial dilated cardiomyopathy, the hypothesis of a minor role of viral infection in chronic idiopathic and familial dilated cardiomyopathy may not be completely ruled out.
Acknowledgments
British Heart Foundation grant CH/92013 supported this work.
References
Footnotes
-
↵* N G Mahon and B Zal contributed equally to this work