Article Text

Abstract
Objective: To examine the effect of tetrahydrobiopterin (BH4), an essential cofactor for nitric oxide synthase, on coronary artery endothelial function in hypercholesterolaemic patients.
Design: Quantitative coronary angiography and Doppler flowmetry were used to examine the effects of intracoronary infusion of BH4 on vascular response to acetylcholine (ACh).
Setting: Tertiary cardiology centre.
Patients: 18 patients with angiographically normal coronary arteries, of whom nine had hypercholesterolaemia and nine had noromocholesterolaemia.
Interventions: ACh (3 and 30 μg/min) was infused for two minutes into the left coronary ostium. ACh was then simultaneously infused with BH4 (1 mg/min) before and after infusion of L-NG-monomethyl-L-arginine (L-NMMA) (40 μmol/min for five minutes).
Main outcome measures: Diameter of the epicardial coronary arteries and coronary blood flow.
Results: In hypercholesterolaemic patients, BH4 attenuated the ACh induced decrease in coronary diameter (p < 0.05) and restored the ACh induced increase in coronary blood flow (p < 0.05). In normocholesterolaemic patients, BH4 did not affect the ACh induced changes in coronary diameter or coronary blood flow. In both groups, L-NMMA decreased the baseline coronary diameter (p < 0.05) and baseline coronary blood flow (p < 0.05). In hypercholesterolaemic patients, L-NMMA inhibited both the BH4 mediated attenuation of the ACh induced decrease in coronary diameter (p < 0.05) and the BH4 mediated enhancement of the ACh induced increase in coronary blood flow (p < 0.01).
Conclusions: Intracoronary infusion of BH4 restores coronary endothelial function by improving the bioavailability of endothelium derived nitric oxide in hypercholesterolaemic patients.
- coronary artery
- tetrahydrobiopterin
- nitric oxide
- hypercholesterolaemia
- ACh, acetylcholine
- BH4, tetrahydrobiopterin
- L-NMMA, L-NG-monomethyl-L-arginine
Statistics from Altmetric.com
Patients with various coronary risk factors, such as hypercholesterolaemia, have been shown to have impaired coronary artery endothelium dependent vasodilatation in response to acetylcholine (ACh), which is characterised by reduced endothelium derived nitric oxide bioavailability.1–5 It has been reported that tetrahydrobiopterin (BH4) serves as an essential cofactor for endothelial nitric oxide synthase6, 7 and that reduced bioavailability of BH4 during activation of nitric oxide synthase decreases nitric oxide production, while simultaneously increasing formation of oxygen derived free radicals.8–10 In addition, a recent study suggested that BH4 may serve as a scavenger of oxygen derived free radicals.11 Therefore, intracellular BH4 concentrations in endothelial cells may be decreased in patients with impaired endothelial function. In support of this hypothesis, recent studies have shown that supplementation of BH4 improves impaired endothelial function under various pathological states in vivo, including hypercholesterolaemia and smoking.12, 13 In addition, Maier and colleagues14 reported that BH4 improves impaired coronary vascular responses to ACh in the coronary arteries of patients with coronary artery disease. However, most of the patients involved in these studies had multiple coronary risk factors or coronary artery disease. To date, no study has investigated the effect of BH4 on impaired coronary nitric oxide bioavailability in patients with hypercholesterolaemia.
We carried out this study to examine the effect of BH4 on coronary vascular responses to ACh in hypercholesterolaemic patients without other major coronary risk factors who have not yet developed coronary artery disease. In addition, we examined whether endothelium derived nitric oxide contributes to the coronary vascular response to BH4 by using L-NG-monomethyl-L-arginine (L-NMMA), a nitric oxide synthase inhibitor.
METHODS
Study population
Between January 1999 and January 2001, we studied nine patients with hypercholesterolaemia (seven men and two women, mean (SD) age 61 (9) years, range 46–70 years) and nine age matched patients with normocholesterolaemia (seven men and two women, mean (SD) age 59 (9) years, range 45–70 years). All of the patients had angiographically normal epicardial coronary arteries and normal coronary flow reserve, determined at the time of diagnostic coronary angiography for the investigation of atypical chest pain. Chest pain was atypical for effort angina in all of the patients. The patients were not receiving any antihypertensive drugs, including angiotensin converting enzyme inhibitors, any drugs known to affect lipid metabolism, or any vitamin supplements for at least eight weeks before cardiac catheterisation. Hypercholesterolaemia was defined as a fasting total cholesterol concentration > 6.2 mmol/l without the use of antihypercholesterolaemic drugs. In addition, there was no medical evidence indicating the presence of either hypertension or diabetes mellitus in any of the patients. None of the patients involved in this study had smoked for the preceding 15 years. Patients with severe left ventricular dysfunction and those with valvar heart diseases were excluded from the study. Furthermore, patients with angiographically documented coronary spasm (> 50% luminal narrowing) after intracoronary infusion of ACh were excluded. Written consent was obtained from each patient and the protocol was approved by the Hiroshima University School of Medicine Ethics Committee.
Study design
The study design has previously been described in detail.15, 16 In brief, cardiac medications were withheld for at least 48 hours before cardiac catheterisation. A 6 French gauge guide catheter was introduced into the left main coronary artery. A 0.014 inch Doppler flow guide wire (Flowire, Cardiometrics, Mountain View, California, USA) was then advanced into the proximal segment of the left anterior descending coronary artery and positioned in a straight segment of the vessel to acquire an adequate flow velocity signal.
Study protocol
A schematic representation of the study protocol is shown in fig 1. After baseline conditions were established, incremental doses of ACh (3 and 30 μg/min, intracoronary concentration 10−7 and 10−6 mol/l, respectively) were infused into the left coronary artery for two minutes at five minute intervals. Fifteen minutes later, when baseline conditions had been reestablished, BH4 (1 mg/min, intracoronary concentration 3.3 × 10−5 mol/l) was infused into the left coronary artery for two minutes. This dose was based on the doses required for dilating human forearm vessels12 and was found to increase the concentration of BH4 in the coronary sinus from 2.5 (0.3) ng/ml to 232.4 (43.7) ng/ml in preliminary studies. Therefore, we expected that this dose of BH4 would provide sufficient amounts of BH4 for increasing nitric oxide bioavailability in the coronary endothelial cells. Incremental doses of ACh were then simultaneously infused with BH4 for two minutes. Fifteen minutes later, an intracoronary infusion of L-NMMA (40 μmol/min for five minutes) was started and the co-infusion of ACh with BH4 was repeated. Finally, glyceryl trinitrate (200 μg) was given as an intracoronary injection. All of the drugs were infused with an infusion pump (Terufusion, Terumo, Tokyo, Japan) at a rate of 1 ml/min.

Schematic representation of the study protocol. ACh, acetylcholine; BH4, tetrahydrobiopterin; GTN, glyceryl trinitrate; L-NMMA, L-NG-monomethyl-L-arginine.
Coronary angiograms were performed at baseline and at the end of each drug infusion. The coronary blood flow velocity was monitored continuously by a 12 MHz pulsed Doppler velocimeter (FloMap, Cardiometrics). Arterial pressure, heart rate, and ECG were monitored continuously and recorded with a multichannel recorder (Polygraph 1600, NEC, Tokyo, Japan).
Quantitative coronary angiography and determination of coronary blood flow
Coronary angiograms were acquired and analysed using a digital image acquisition (HICOR x ray system, Siemens, Forchheim, Germany) and analysis systems (CAAS II QCA system, Pie Medical, Maastricht, Netherlands). The coronary segment 2 mm distal to the Doppler wire tip was selected for quantitative analysis. The average of three measurements of the luminal diameter was used for analysis. A strong correlation for intraobserver measurements was noted (r = 0.996, p < 0.001). Analysis of interobserver measurements also showed high reproducibility (r = 0.987, p < 0.001). Coronary blood flow velocity was measured at baseline and under steady state conditions for each drug infusion. Blood flow was quantitatively estimated from the Doppler flow velocity and the arterial diameter by the following equation: Changes in coronary diameter and coronary blood flow are expressed as the percentage change from the control value.
Changes in coronary diameter and coronary blood flow are expressed as the percentage change from the control value.
Drug preparations
ACh chloride was purchased from Daiichi Pharmaceutical Co (Tokyo, Japan) and glyceryl trinitrate was purchased from Nihonkayaku Co (Tokyo, Japan). L-NMMA and BH4 were purchased from Sigma Chemical Co (St Louis, Missouri, USA) and sterilised at the Pharmacy Department of Hiroshima University Hospital. All drugs were dissolved in oxygen-free saline immediately before use.
Statistical analysis
Data are expressed as the mean (SEM) unless otherwise indicated. Differences in categorical variables between the two groups were analysed by Mann-Whitney U test. Serial responses of haemodynamic variables, coronary diameter, and coronary blood flow to various drugs were compared using a one way analysis of variance. If the analysis of variance showed a significant difference between the mean values, the level of significance was determined by contrast. Serial percentage changes in coronary diameter and coronary blood flow were compared using a two way analysis of variance for repeated measures. A probability value of p < 0.05 was considered to be significant.
RESULTS
Clinical characteristics and haemodynamic variables
Table 1 shows plasma lipoprotein concentrations of the patients studied. Total cholesterol and low density lipoprotein cholesterol concentrations at the time of the study were higher in hypercholesterolaemic patients than in normocholesterolaemic patients. Body mass index, blood pressure, and serum glucose were similar in both groups (table 1). The intracoronary administration of ACh, BH4, or L-NMMA did not significantly alter the baseline mean arterial pressure or heart rate in either group. Glyceryl trinitrate decreased the mean arterial pressure but increased the heart rate compared with control values (data not shown).
Patient characteristics
Effect of intracoronary infusion of ACh or BH4 on coronary response
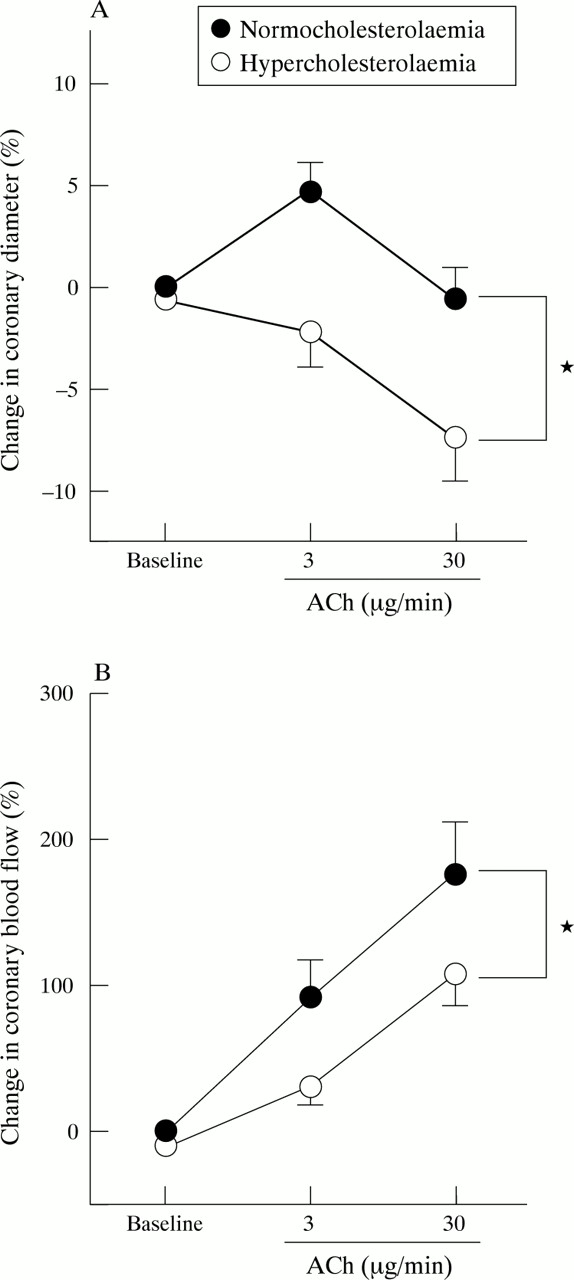
A high dose of ACh (30 μg/min) decreased the coronary diameter in hypercholesterolaemic patients (p < 0.01) while a low dose of ACh (3 μg/min) dilated the epicardial coronary arteries in normocholesterolaemic patients (p < 0.05) (table 2, fig 2). ACh produced dose dependent increases in coronary blood flow in both groups but the increase in coronary blood flow was significantly smaller in hypercholesterolaemic patients than in normocholesterolaemic patients (p < 0.05 between the two groups; table 2, fig 2). In both groups, BH4 infusion alone did not cause any significant changes in either coronary diameter or coronary blood flow (table 2).
Change in coronary diameter and coronary blood flow
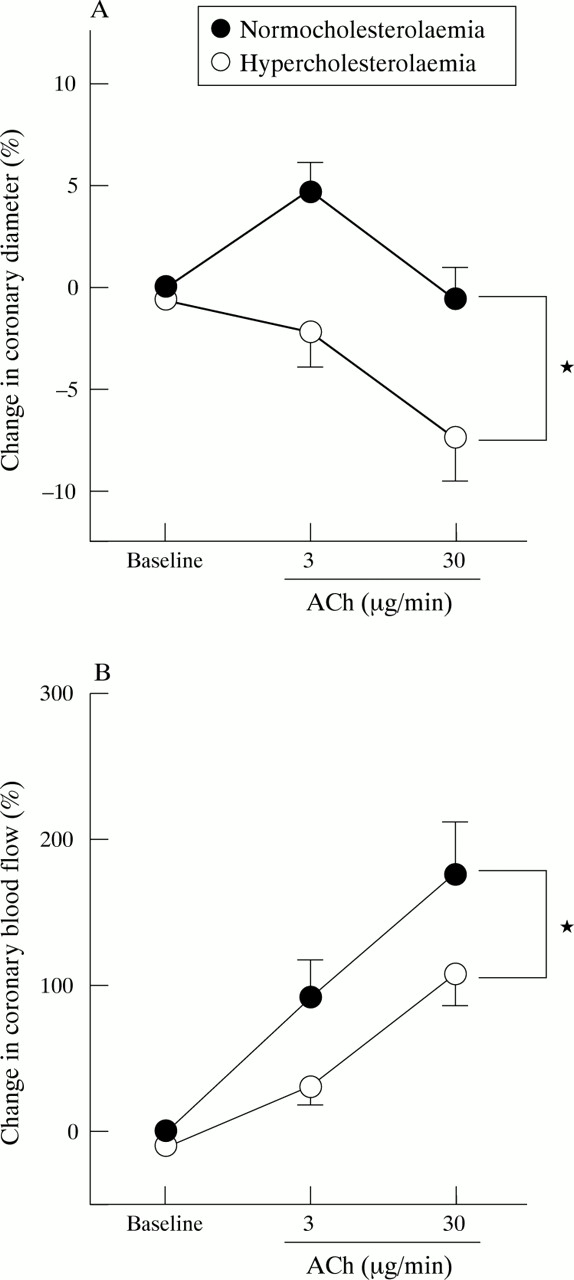
Percentage change in (A) coronary diameter and (B) coronary blood flow in response to acetylcholine (ACh) in hypercholesterolaemic and normocholesterolaemic patients. Vertical bars represent SEM. *p < 0.05.
Effect of BH4 on ACh induced coronary response
In hypercholesterolaemic patients, co-infusion of BH4 and ACh attenuated the ACh (3 and 30 μg/min) induced constriction of the epicardial arteries (−0.1 (1.6)% and −2.3 (1.3)%, respectively, p < 0.05 v ACh alone; table 2, fig 3). In addition, in hypercholesterolaemic patients, co-infusion of BH4 and ACh restored the ACh induced increase in coronary blood flow (83.7 (19.5)% and 181.2 (26.4)%, p < 0.05 v ACh alone; table 2, fig 3). In contrast, in normocholesterolaemic patients, BH4 did not affect the ACh induced changes in coronary diameter or coronary blood flow (table 2, fig 4).
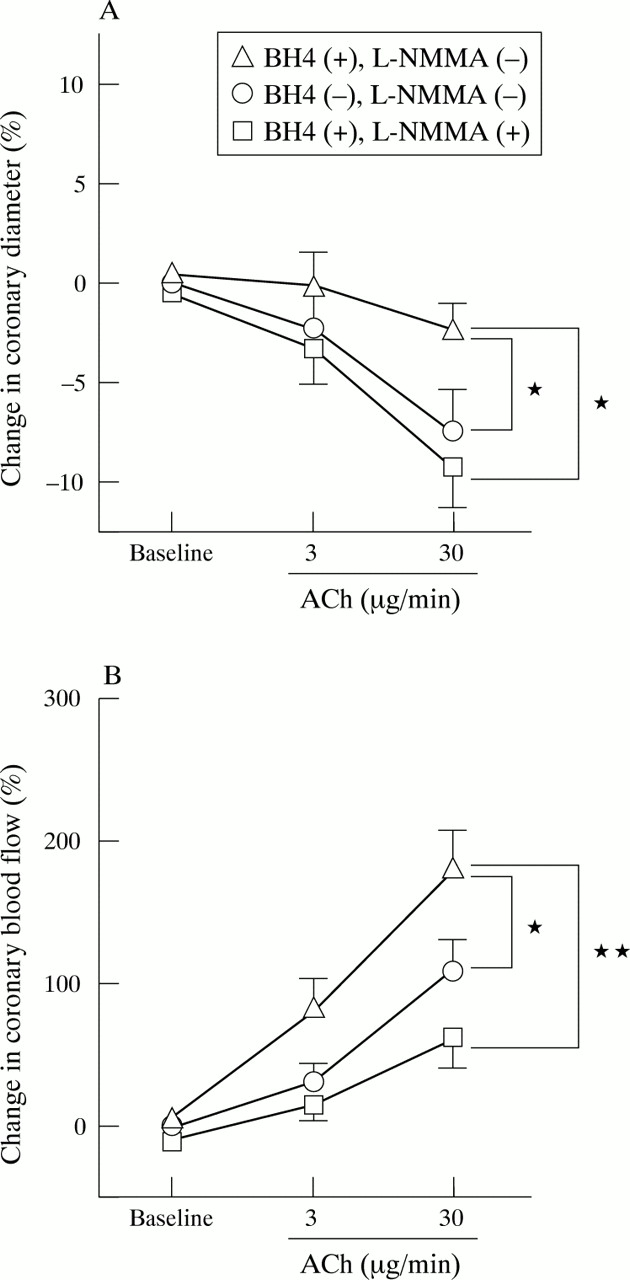
Percentage change in (A) coronary diameter and (B) coronary blood flow in response to ACh with BH4 (open triangles), without BH4 (open circles), or with BH4 after L-NMMA infusion (open squares) in hypercholesterolaemic patients. Vertical bars represent SEM. *p < 0.05; **p < 0.01.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
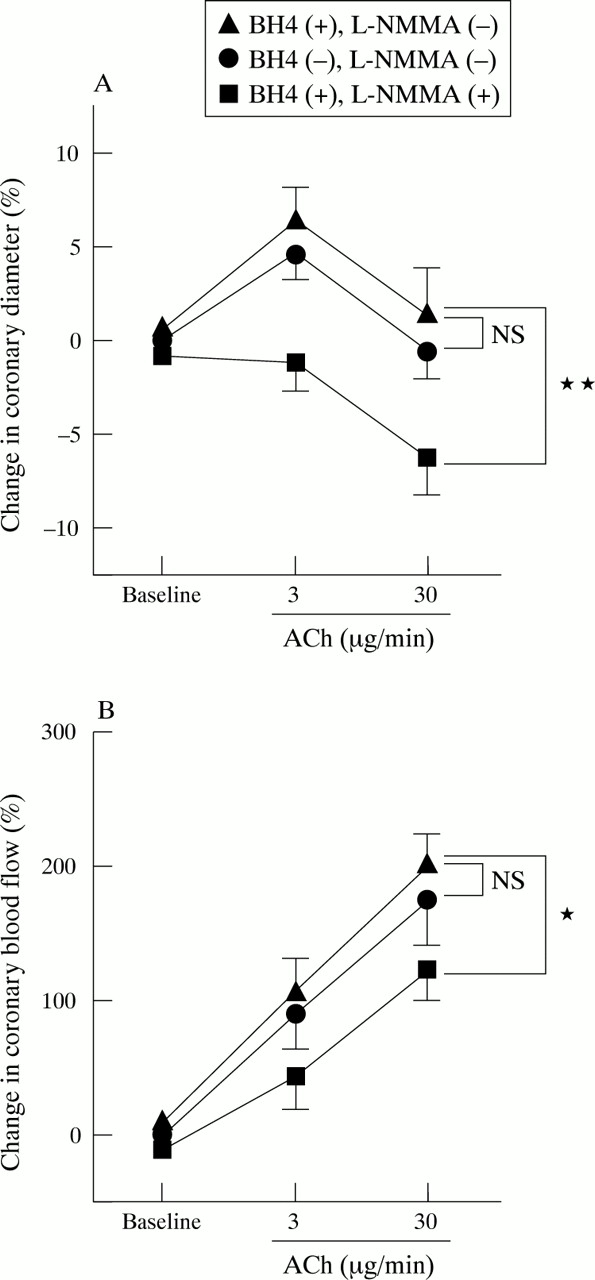
Percentage change in (A) coronary diameter and (B) coronary blood flow in response to ACh with BH4 (solid triangles), without BH4 (solid circles), or with BH4 after L-NMMA infusion (solid squares) in normocholesterolaemic patients. Vertical bars represent SEM. *p < 0.05; **p < 0.01.
Effect of L-NMMA on ACh induced coronary response in the presence of BH4
Intracoronary infusions of L-NMMA significantly decreased both the baseline coronary diameter and the baseline coronary blood flow in both groups (table 2). In hypercholesterolaemic patients, L-NMMA inhibited both the BH4 mediated attenuation of the ACh induced decrease in coronary diameter (−3.3 (1.8)% and −9.3 (2.0)%, p < 0.05 v after co-infusion of BH4 and ACh; table 2, fig 3) and the BH4 mediated enhancement of the ACh induced increase in coronary blood flow (14.7 (9.3)% and 61.3 (20.3)%, p < 0.01 v after co-infusion of BH4 and ACh; table 2, fig 3). In normocholesterolaemic patients, ACh in combination with BH4, which did not affect the coronary diameter or coronary blood flow before infusion of L-NMMA, decreased the coronary diameter (p < 0.01 v after co-infusion of BH4 and ACh; table 2, fig 4) and coronary blood flow (p < 0.05 v after co-infusion of BH4 and ACh; table 2, fig 4) after the infusion of L-NMMA.
Effect of glyceryl trinitrate on coronary response
Intracoronary infusion of glyceryl trinitrate caused increases in coronary diameter and coronary blood flow in both groups. There were no significant differences in the glyceryl trinitrate induced increases in coronary diameter or coronary blood flow between the hypercholesterolaemic and normocholesterolaemic groups (table 2).
DISCUSSION
The present study showed that BH4 restores impaired coronary arterial responses in hypercholesterolaemic patients who have not yet developed coronary artery disease. The effects of BH4 on the vascular responses to ACh were inhibited by L-NMMA, an inhibitor of nitric oxide synthase. These findings suggest that BH4 improves coronary artery endothelial dysfunction by increasing nitric oxide bioavailability.
Hypercholesterolaemia and endothelial dysfunction
Endothelial cells contribute to the regulation of vascular tone by releasing vasoactive compounds, including nitric oxide, prostacyclin, and endothelium derived hyperpolarising factor.17–19 Although it remains to be determined whether the relative contribution of these factors to endothelium dependent vasodilatation varies according to vessel size in humans, nitric oxide has been shown to be responsible for endothelium dependent vasodilatation of the epicardial and resistance arteries. Therefore, impaired coronary vasoresponse to ACh, an agonist of nitric oxide, is characterised by reduced nitric oxide bioavailability. The differences in vascular response to ACh between the hypercholesterolaemic and normocholesterolaemic patients observed in this study also indicate that ACh induced dilatation of the epicardial and resistance arteries was reduced in hypercholesterolaemic patients. This is in keeping with previous reports of changes in endothelium dependent vasorelaxation of coronary arteries before the development of atherosclerotic lesions.1–5
Several mechanisms by which hypercholesterolaemia may impair endothelial function have been proposed. Firstly, substrate deficiency may reduce nitric oxide bioavailability.20 Secondly, several abnormalities in the signal transduction pathway that carries the message from membrane receptors to nitric oxide synthase may contribute to the depressed endothelial responsiveness in the setting of hypercholesterolaemia.21, 22 Thirdly, oxidised low density lipoprotein, which is associated with hypercholesterolaemia, may cause oxidative stress in endothelial cells and attenuate endothelial nitric oxide bioavailability.23 Fourthly, increased concentrations of asymmetric dimethyl L-arginine, an endogenous inhibitor of nitric oxide synthase, may be associated with attenuated endothelium dependent vasodilatation in hypercholesterolaemic patients.24 In addition to these mechanisms, our data, as well as findings in the forearm circulation,12 indicate that reduced bioavailability of BH4 may also contribute to the impairment of endothelial nitric oxide bioavailability in hypercholesterolaemic patients.
Mechanisms of impaired BH4 bioavailability in hypercholesterolaemic patients
Intracellular BH4 may be either absolutely or relatively deficient in the endothelial cells of hypercholesterolaemic patients. Hypercholesterolaemia is associated with the production of oxygen derived free radicals, which cause oxidative stress in the endothelial cells. Oxidative stress may alter the redox state of endothelial cells and thereby impair the biosynthesis of BH4, which requires a normal cellular redox state. Increased formation of oxygen derived free radicals may inhibit the biosynthesis of BH4 or prevent recycling of BH4.25 Another possibility is that nitric oxide synthase activity may be up regulated in the presence of hypercholesterolaemia, leading to a net reduction in the bioavailability of BH4 in the endothelial cells.
Effect of BH4 on endothelial function in humans
In this study, acute administration of BH4 attenuated the vasoconstrictive responses to ACh and increased the coronary blood flow response to ACh in hypercholesterolaemic patients, in keeping with recent observations in patients with coronary artery disease.14 These observations suggest that BH4 may enter endothelial cells, replenishing stores during short term administration of BH4. In addition, the effects of BH4 on the vascular responses to ACh were inhibited by L-NMMA, indicating that BH4 restores the vasorelaxant responses to ACh through modulation of the L-arginine-nitric oxide pathway and that the vasorelaxant responses to ACh are mediated by nitric oxide. Because BH4 appears to serve as a scavenger of oxygen derived free radicals as well as an essential cofactor for nitric oxide synthase,11 BH4 presumably restored the vasorelaxant response to ACh in hypercholesterolaemic patients by increasing nitric oxide bioavailability or by decreasing nitric oxide breakdown by oxygen derived free radicals.
BH4 did not significantly affect the coronary arterial responses to ACh in normocholesterolaemic patients, suggesting that the BH4 concentration in endothelial cells is not a rate limiting factor for nitric oxide synthesis in the normocholesterolaemic group. In addition, BH4 alone did not change the coronary diameter or blood flow in either group, consistent with recent observations in the forearm and coronary circulations.12, 14 This observation suggests that BH4 does not influence the basal nitric oxide bioavailability of endothelial cells and allows us to speculate that the amount of BH4 required for the augmentation of nitric oxide bioavailability differs between the basal and the stimulated states.
Study limitations
There are several limitations to the present study. None of the patients had angiographically significant stenotic lesions. However, intravascular ultrasound, which can be used to evaluate wall thickening, was not performed in the present study. Zeiher and colleagues26 reported that there is a significant correlation between the vascular response to ACh and atherosclerotic wall thickening in hypercholesterolaemic patients. Therefore, further studies are necessary to assess intimal hyperplasia and structural alterations of the vascular wall using intravascular ultrasound.
Because previous investigators have used oxygen-free saline to dissolve BH4 in in vivo studies,12–14 we used oxygen-free saline to dissolve BH4 in the present study. However, Walter and colleagues27 reported that BH4 dissolved in bicarbonate buffered solution increases myocardial blood flow in healthy volunteers. Although it is possible that solvents can affect the redox state of BH4, it remains to be determined whether the solvent can influence the effect of BH4 on the vascular response.
The intracoronary injection of contrast medium increased coronary blood flow. Therefore, the infusion of contrast medium may have caused flow induced vasodilatation. However, contrast medium was infused at a fixed rate for a total of 8 ml. Therefore, we believe that influences of flow induced vasodilatation on the coronary diameter are similar for each infusion of contrast medium.
Oral administration of BH4 causes a threefold increase in the concentration of BH4, leading to enhanced vasorelaxation in long time smokers.28 In our preliminary study, intracoronary infusion of BH4 caused approximately a 100-fold increase in the concentration of BH4 in the coronary sinus. Heitzer and colleagues13 showed that the effects of BH4 on vascular responses to ACh were abolished by pretreatment with an antioxidant, suggesting that functional depletion of BH4 caused by enhanced BH4 oxidation accounts at least in part for endothelial dysfunction in chronic smokers. Furthermore, treatment with vitamin C significantly increased concentrations of the BH4 in cultured human umbilical vein endothelial cells.29 Therefore, it is important to examine the possibility that lower doses of BH4 and pretreatment with an antioxidant can restore coronary endothelial function in hypercholesterolaemic patients.
Although no single assay accurately reflects the production of oxygen derived free radicals, 8-iso-prostaglandin F2α has been shown to be a sensitive and specific marker of oxidative stress.30, 31 However, we did not measure any markers of oxidative stress. Therefore, we cannot exclude the possibility that the direct antioxidant effect of BH4 may contribute to the improvement of endothelial dysfunction in hypercholesterolaemic patients.
Conclusions
The present findings indicate that intracoronary BH4 infusion restores endothelial nitric oxide bioavailability in the epicardial and resistance arteries in hypercholesterolaemic patients. BH4 supplementation may be therapeutically useful in restoring endothelial nitric oxide bioavailability, thereby attenuating the development of coronary endothelial dysfunction.
Acknowledgments
We are grateful to Nobuo Shiode MD, Masaya Kato MD, Yukihito Higashi MD, Hidekazu Hirao MD, Fumiharu Miura MD, and Kenya Sakai MD of the First Department of Internal Medicine, Hiroshima University, and to Takashi Akata MD of the Department of Anesthesiology, Kyusyu University for their technical assistance and helpful comments. We thank Miss Yuko Omura for her secretarial assistance. We also thank Dr Shigeaki Arai and Dr Masahiko Sakai for the preparation of BH4, L-NMMA, and oxygen-free saline.