Article Text

Abstract
Objectives: To determine the effects of atrial septal defects (ASD) and their closure on systolic and diastolic right and left ventricular function; and by comparing surgical closure with transcatheter device closure, to establish differences attributable to cardiopulmonary bypass.
Design: Cross sectionally guided M mode echocardiographic ventricular long axis function was measured prospectively before and within one week after ASD closure by device in 17 patients and by surgery in 12 patients, and compared with 18 normal subjects.
Results: All indices of right ventricular function were impaired after surgery: mean total excursion, −1.89 cm (95% confidence interval (CI), −2.18 to −1.59); peak shortening rate, −9.09 cm/s (−10.82 to −7.35); peak lengthening rate, −9.26 cm/s (−11.09 to −7.43). Total excursion and peak lengthening rate were preserved after device closure, at −0.12 cm (−0.28 to 0.05) and 0.01 cm/s (−2.29 to 2.31), respectively. Left ventricular free wall function was unchanged after closure by either method, while all septal measurements were reduced after closure by either method (changes ranging from −3.51 to −0.32; 95% CI ranging from −4.90 to −0.13).
Conclusions: Left ventricular free wall function is unaffected by ASD closure, whereas septal function is impaired, irrespective of the method of closure. Right ventricular function, both systolic and diastolic, is impaired by cardiopulmonary bypass but preserved after device closure. These findings support the transcatheter approach to ASD closure in anatomically suitable defects.
- atrial septal defect
- cardiopulmonary bypass
- congenital heart disease
- therapeutic cardiac catheterisation
Statistics from Altmetric.com
- atrial septal defect
- cardiopulmonary bypass
- congenital heart disease
- therapeutic cardiac catheterisation
The deleterious effects of cardiopulmonary bypass on ventricular performance are increasingly reported.1,2 While the left ventricle may be relatively spared, abnormalities of interventricular septal motion are common, and there are several studies showing right ventricular dysfunction.3–5 We have recently demonstrated acutely impaired right ventricular contractility after cardiopulmonary bypass using an intraoperative conductance catheter method,6 confirming findings obtained by echocardiography.7 Conventional indices of ventricular function have largely been derived from assessment of short axis changes in the basal segment, which is maintained by the circumferential muscle layer.8–10 There is increasing evidence that the function of the longitudinal component of myocardial fibres is specifically disturbed by ischaemia,11 conduction abnormalities, or other diseases.12 These fibres are subendocardial in location, and form the main bulk of the muscle that controls the function of the right ventricle.13
Since the first use of transcatheter atrial septal defect (ASD) device occlusion in 1976,14 it has been possible to avoid cardiopulmonary bypass during the closure of these congenital heart defects. However, the theoretical benefits of this approach have not been explored. Our aim in this study was to measure echocardiographic indices of right and left ventricular function prospectively in patients undergoing ASD closure by device and by surgery, to define the contribution to changes in ventricular function attributable to cardiopulmonary bypass.
METHODS
Patients
Between August 1997 and September 1999, we studied cross sectionally guided M mode echocardiographic ventricular long axis function prospectively in 17 patients undergoing device closure and in 12 patients undergoing surgery, both before ASD closure and before hospital discharge after closure of the defect. The study was approved by the Royal Brompton Hospital research ethics committee.
All patients had right ventricular volume overload, but were otherwise unselected, other than on the basis of agreeing to participate in the study. Selection for surgery at that time was largely on the basis of patient or parental choice, or unsuitability for device closure because of the proximity of atrioventricular valves or pulmonary or systemic veins.
The mean (SD) defect diameter measured echocardiographically was 13.8 (5.1) mm in the device group, and 17.3 (4.1) mm in the surgical group. Left to right shunt sizes were measured oxymetrically in the device patients at the time of implantation; the pulmonary to systemic flow ratio was 2.2:1 (0.8:1). The pulmonary artery systolic pressure in the device group was 22.3 (4.9) mm Hg.
All device occlusions in this study were performed with the Amplatzer septal occluder (AGA Corporation, Golden Valley, Minnesota, USA). Surgical repairs were performed using a patch of autologous pericardium in all patients. We compared the results obtained with a group of 18 normal subjects in whom we had measured the same echocardiographic variables. The median age of the 17 device patients was 8.0 years, mean (SD) 8.0 (3.1) years; six were male and 11 female. In the surgical group of 12 patients, median age was 5.2 years and mean (SD) 6.2 (3.2) years; three were male and nine female. Median age of the 18 normal children was 7.3 years, mean (SD) 7.0 (0.2) years; nine were male and nine female.
ECGs were recorded on the day before intervention and again before discharge in both patient groups, using a Hewlett-Packard ECG page writer (Agilent Technologies, Palo Alto, California, USA) with built in analysis software. In all patients, echocardiographic studies were done on the day before the procedure, and again within seven days of closure (median, 1 day after the procedure in the device group, 4 days in the surgical group). At these times, satisfactory closure of the defects was confirmed echocardiographically in all patients, with no haemodynamically important residual shunts.
Technique of ASD device occlusion
All device implantations were conducted under general anaesthesia, with transoesophageal echocardiographic guidance and intermittent fluoroscopy. Following standard right heart catheterisation and haemodynamic measurements, an exchange guide wire was placed in a left pulmonary vein. A sizing balloon was passed into the left atrium, and the stretched diameter of the ASD determined. The sizing balloon was then exchanged for the appropriate size of device delivery sheath, and following de-airing in the inferior caval vein, the appropriate sized Amplatzer septal occluder device was deployed, and released across the defect. The correct siting of the device, and the presence of any residual shunting, were assessed by transoesophageal echocardiography of the atrial septum.
Echocardiographic assessment of ventricular function
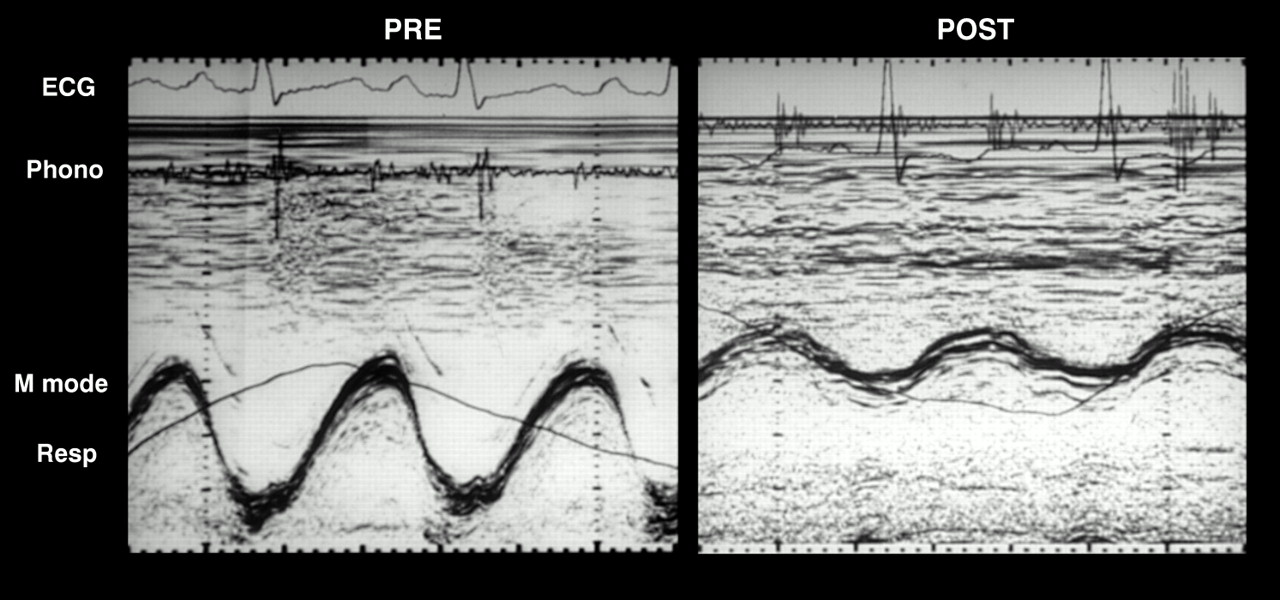
All studies were performed with the subject lying in the semilateral supine position, using a 3.5–5.0 MHz transducer linked to a Hewlett-Packard Sonos 2000 machine (Agilent Technologies). Long axis M mode recordings of the right ventricle, interventricular septum, and left ventricular free wall were made simultaneously with superimposed ECG, respiration phase, and phonocardiogram. Long axis recordings were obtained from the apical four chamber view with the M mode cursor positioned through the lateral angle of the tricuspid valve annulus, central fibrous body (septal), and the left angle of the mitral valve annulus, respectively. The resulting M mode traces of right ventricular, septal, and left ventricular long axis function were recorded on photographic paper at 100 mm/s speed, and later digitised at end expiration to obtain peak shortening and lengthening rates, using dedicated computer software. Aortic and pulmonary valve closure sounds (A2 and P2) were identified as the high frequency components of the second heart sound on the phonocardiogram and confirmed against the aortic and pulmonary Doppler flow, respectively. From each M mode recording, parameters from three beats were measured, and the mean values calculated. Heart rates during echocardiographic studies were calculated directly from the simultaneous ECGs. Examples of actual M mode recordings obtained from the right ventricular are shown in figs 1 and 2.

Echocardiographic M mode long axis recording of the right ventricle. PRE: before closure; POST: after closure by device. Phono, phonocardiograph; Resp, respiration.

Echocardiographic M mode long axis recording of the right ventricle. PRE: Before closure; POST: after surgical closure. Phono, phonocardiograph; Resp, respiration. Note the considerable reduction in total excursion following closure of atrial septal defect, as compared with fig 1.
Measurements
Electrocardiography
From the 12 lead ECG recordings, heart rate, PR interval, QRS duration, and axis were automatically measured using the inbuilt software. The reproducibility of ECG measurements in our department has been described previously.15
Echocardiography
Total ventricular long axis excursion was taken from the innermost point (at end systole) to the outermost point (at end diastole) of right and left atrioventricular valve ring movement. Peak shortening (in systole) and peak lengthening (diastolic) rates were derived from the digitised traces. Tricuspid regurgitation, when present, was used to estimate right ventricular–right atrial pressure drop using continuous wave Doppler.
Statistical methods
Between-group comparisons of M mode echocardiographic variables were made with unpaired Student's t tests (table 1, figs 3–5). Mean differences following ASD closure by either technique were compared using one sample t tests against a test value of zero (figs 3–5). Fisher's exact probability test was used to compare the frequency of disturbances (outside 95% confidence intervals) of total excursion, peak shortening rate, and peak lengthening rate in the device and surgical groups. A probability (p) value of 0.05 was considered significant in all cases. Values are given as mean (SD).
M mode ventricular long axis function in 18 normal children, compared with 17 device and 12 surgical patients, before intervention
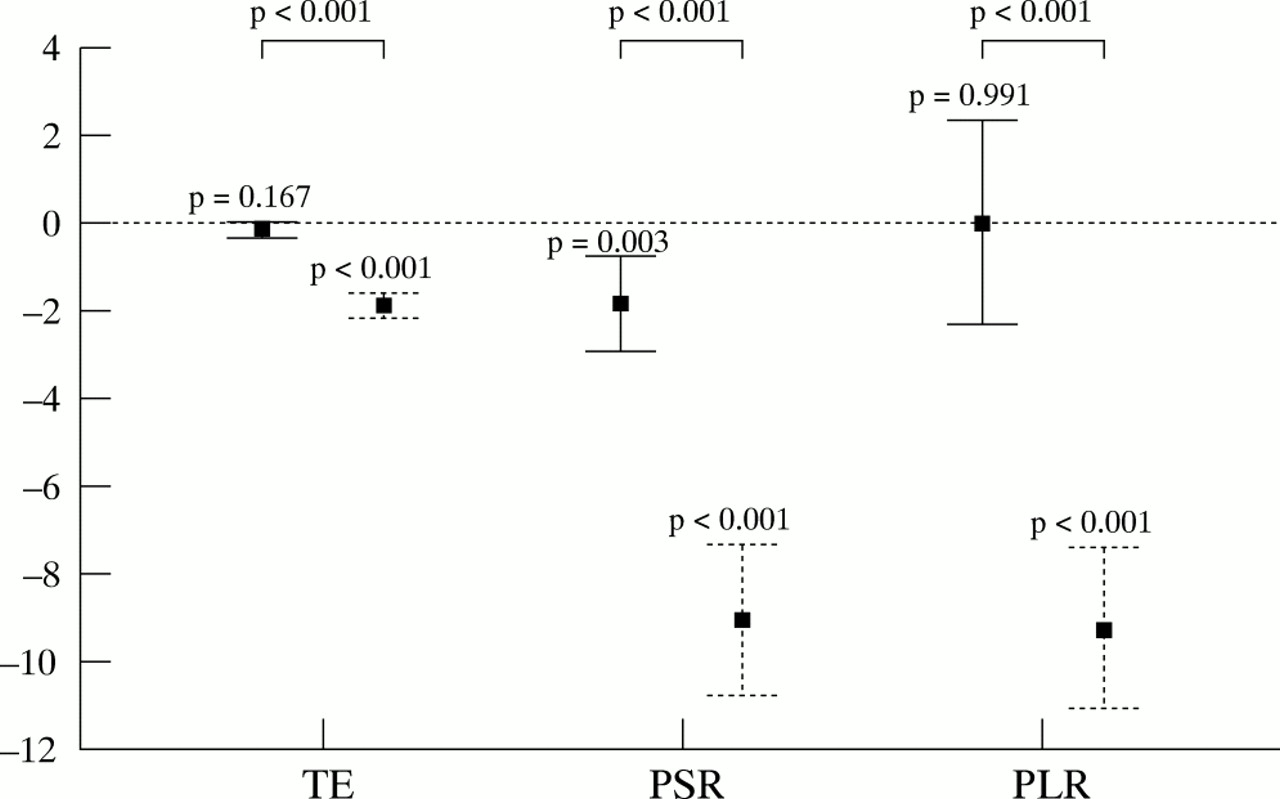
Changes in right ventricular function following closure of atrial septal defect. Measurements are presented as means with 95% confidence intervals. Solid fill/lines, device closure; solid fill and dashed lines, surgical closure. PLR, peak lengthening rate (cm/s); PSR, peak shortening rate (cm/s); TE, total excursion (cm). Statistical comparisons: individual, difference from zero; bracketed, between-group differences.

Changes in septal function following closure of atrial septal defect. Measurements are presented as means with 95% confidence intervals. Solid fill/lines, device closure; solid fill and dashed lines, surgical closure. PLR, peak lengthening rate (cm/s); PSR, peak shortening rate (cm/s); TE, total excursion (cm). Statistical comparisons: individual, difference from zero; bracketed, between-group differences.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
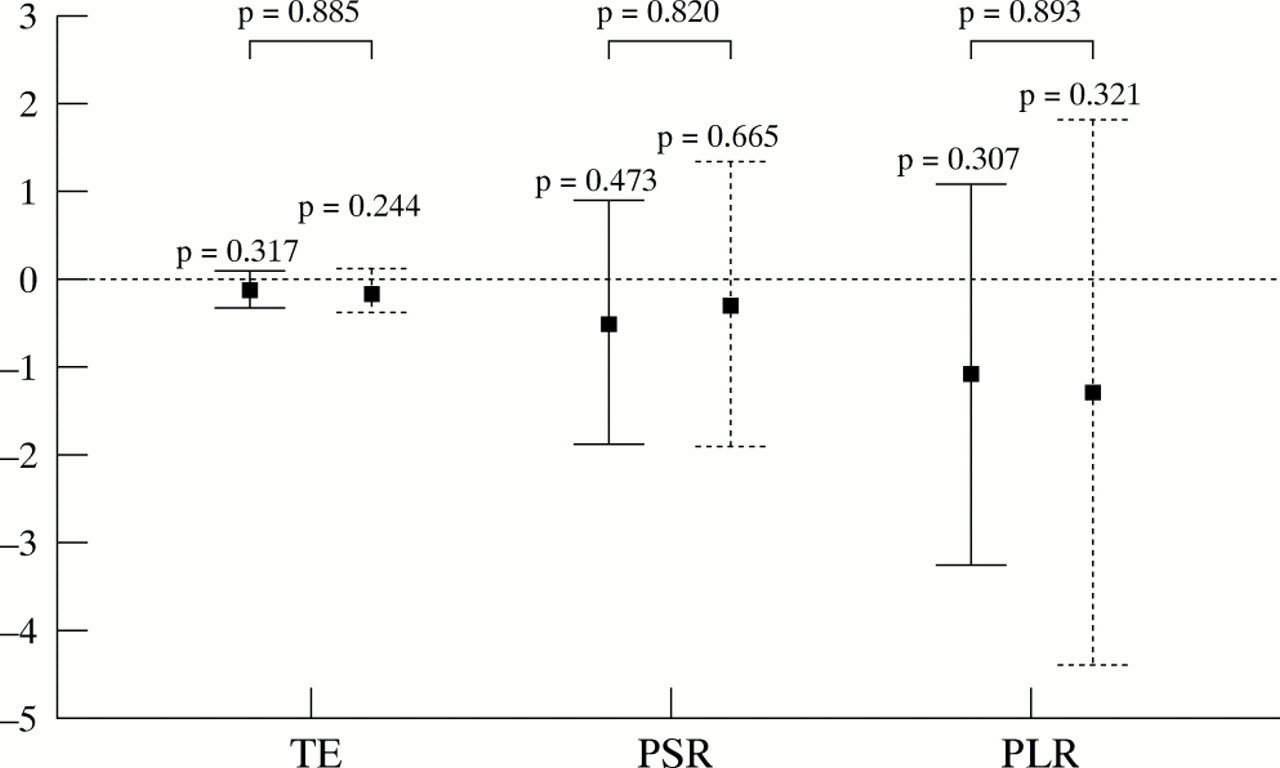
Changes in left ventricular function following closure of atrial septal defect. Measurements are presented as means with 95% confidence intervals. Solid fill/lines, device closure; solid fill and dashed lines, surgical closure. PLR, peak lengthening rate (cm/s); PSR, peak shortening rate (cm/s); TE, total excursion (cm). Statistical comparisons: individual, difference from zero; bracketed, between-group differences.
RESULTS
Electrocardiography
The mean heart rate at the time of echocardiographic assessment was 91.9 (15.3) beats/min pre-device, 90.9 (16.7) beats/min post-device, 99.5 (10.0) beats/min preoperatively, and 91.8 (12.9) beats/min postoperatively. Thus heart rate did not change after ASD closure, regardless of the method used. Of the measured ECG variables, the mean frontal QRS axis changed from 82 (8)° to 77 (3)° (p = 0.04) after ASD device closure, but was not affected by surgical closure. The PR interval and QRS duration did not change following ASD closure, irrespective of the method employed.
Echocardiography
Before intervention
Both groups of patients were compared with the 18 normal children and between themselves (table 1). Before any intervention, right ventricular total excursion and peak lengthening and shortening rates were higher in both patient groups than in the normal controls (p < 0.001 to 0.035). Right ventricular total excursion and peak shortening rate were higher in the surgical group than in the device patients (p = 0.020 and 0.012, respectively). Septal measurements did not differ from the normal controls in either treatment group. Although left ventricular free wall measurements did not differ from normal in the device patients, left ventricular total excursion and peak lengthening rate were lower than normal in the surgical patients (p = 0.030 and 0.015, respectively). The peak Doppler tricuspid regurgitant velocity was measurable in 12 of the 17 device patients and nine of the 12 surgical patients. The right ventricular to right atrial pressure drop thus estimated did not differ between the device group (22.4 (5.1) mm Hg) and the surgical group (23.3 (2.6) mm Hg).
After intervention
Changes in measurements after ASD closure are illustrated in figs 3–5. Right ventricular excursion and peak lengthening did not change with device closure. Peak shortening rate, however, fell (p = 0.003), as did all three septal indices (p = 0.002 to 0.005). The left ventricular free wall was unaffected by device implantation. Following surgery, all three right ventricular and septal systolic and diastolic measurements fell (p < 0.001). Left ventricular free wall function was spared. All indices of right ventricular function were much more impaired by surgery than by device occlusion (p < 0.001). Right ventricular function before and after device closure is illustrated by fig 1, with corresponding changes relating to surgical repair in fig 2.
To examine the observed disturbances in ventricular function further, we noted the frequency of each disturbance in the two patient groups. Right ventricular excursion did not fall below the 95% confidence interval in any patient after device implantation, while right ventricular peak shortening and lengthening rates each fell below this interval in only one of the 17 patients. In contrast, impairment of right ventricular function was almost invariable after surgery, affecting total excursion in all 12 patients, and peak shortening and lengthening rates each in 11 of the 12 patients (p < 0.001). The frequency of disturbances of total excursion and peak shortening and lengthening rates did not differ for septal and left ventricular free wall measurements between the two patient groups. The peak Doppler tricuspid regurgitant velocity was measurable in 10 of the 17 device patients and in eight of the 12 surgical patients. The estimated mean right ventricular to right atrial pressure drop was 22.0 (4.4) mm Hg in the device group, and 23.5 (3.9) mm Hg in the surgical group (NS).
DISCUSSION
The reported effects of atrial septal defects on the left ventricle are variable. In most echocardiographic studies, left ventricular systolic function was normal in patients with ASD, despite right ventricular volume overload.8,10,16,17 However, a reduced left ventricular ejection fraction has been found in patients with ASD and severe right ventricular volume overload,9 and cineangiographic studies suggest abnormalities of left ventricular function affecting systole18 and diastole.19,20 The effects of an ASD on right ventricular function appear to be more consistent. Volume overload of the right ventricle is usual in patients with significant left to right shunts. Although delayed right ventricular contraction has been detected with radionuclide studies (in the absence of conduction defects),21 echocardiographic assessment has shown right ventricular systolic function to be normal or exaggerated.3,22 Abnormal septal motion occurs in the majority (up to 86%) of patients with an ASD,17,19 but this appears to resolve with exercise23,24 and after surgical repair.25
Following surgical repair of an ASD, echocardiographic assessment suggests an increase in left ventricular volume,25 and in one study left ventricular function was normal both before and one year after repair.8 Persistence of right ventricular dilatation after ASD repair is commonly reported,8 affecting more than 80% of patients up to five years after repair.3 Although impairment of right ventricular systolic function has previously been reported after cardiopulmonary bypass3,7—including our invasive assessment of acute changes6—an echocardiographic study comparing surgical repair of ASD with device closure failed to detect a change in right ventricular volume or function after closure by either technique.22
Surgical repair of ASD is well established, with a low morbidity and a mortality approaching zero. However, potential advantages of ASD device closure include avoidance of the chest opening, adverse inflammatory responses,26–28 and transiently impaired cardiac output that accompany cardiopulmonary bypass.1,2 This facilitates ASD closure in older children without disruption of schooling, and in elderly or sick adults. Hospital inpatient stay is typically much shorter after device closure than after surgery, with a return to school or work in days instead of weeks. Pericardial effusions, occasionally fatal, are well described following surgical ASD repair,29 but not after device closure.
In keeping with previous work,8 our findings showed that left ventricular free wall function was not affected by surgical ASD repair. It is not surprising, therefore, that ASD device closure also left ventricular function intact. On the other hand, in both device and surgical groups all indices of right ventricular function were similarly increased before the intervention compared with the normal controls. As previously observed,30 all these indices fell after cardiopulmonary bypass. After device occlusion, right ventricular total excursion and peak lengthening rate were preserved. Although the right ventricular peak shortening rate was reduced, the effect of surgery on this measure was significantly more marked. Before the intervention, septal function did not differ from normal in either patient group. Interestingly, all septal measurements were significantly reduced by both surgery and device occlusion.
The supranormal right ventricular function before intervention in ASD patients most probably reflects right ventricular volume loading. Similarly, the reduction in right ventricular peak shortening rate following ASD device occlusion is likely to reflect volume unloading of the right ventricle, as the measured values were not different from normal control values. In surgical patients, the right ventricular total excursion and peak lengthening rate were also reduced after ASD repair, suggesting an independent effect of cardiopulmonary bypass on right ventricular systolic and diastolic function. The right ventricle is particularly susceptible to the problems of cardiopulmonary bypass and intraoperative ischaemia. As the right ventricular free wall is composed largely of longitudinal muscle fibres, the compensatory response to intraoperative injury by circumferential fibres—as in the case of the left ventricle—may be lacking, although previous studies have failed to show a difference in short axis indices following ASD closure with or without cardiopulmonary bypass.22 The distribution of cardioplegic solution is rarely uniform,4,5 and the effect of higher myocardial temperature, because of its exposed position in the mediastinum during surgery, also contributes to postoperative right ventricular dysfunction.
The reasons for the impairment of septal systolic and diastolic function following surgery and device occlusion are not clear, but in the relative absence of ECG changes it may reflect the imposition of a non-contractile element within the atrial septum, affecting excursion of the ventricular septum beneath it. All measurements (total excursion, peak shortening rate, lengthening rate) were below normal in both groups. As these disturbances were shared equally by the two groups, they may represent a transitional stage for the septum, functioning as a component of the right ventricle before ASD closure, and of the left ventricle afterwards.
The relevance of the observed differences in right ventricular performance, dependent on the mode of ASD closure, deserves further consideration. Although left to right shunt sizes and pulmonary artery pressures were determined at the time of cardiac catheterisation in all device patients, it was not possible to obtain these measurements in the surgical group, and right ventricular volume might have differed between groups. However, shunt sizes are related to defect diameter. The 3.5 mm mean difference in defect diameter was statistically insignificant and cannot explain the reduction in right ventricular function following cardiopulmonary bypass. Furthermore, we compared the same variables before and after ASD closure. The higher preprocedural right ventricular total excursion and peak shortening rate in the surgical patients compared with the device group is consistent with a higher right ventricular preload in the surgical group, despite the non-significant difference in defect diameter. However, the more profound depression of these measures of right ventricular systolic function following surgery achieves an even greater importance in the light of the preprocedural observations. As measurements were objectively obtained using a highly reproducible technique,31 we do not believe that technical error was responsible for these findings. Although long term data were not available at the time of this analysis, our previous data suggest that functional performance is normal late after surgical repair,32 and we are unable to predict whether these changes in ventricular function will persist. Nonetheless, right ventricular dysfunction can be added to the list of undesirable effects of cardiopulmonary bypass which may be avoided by transcatheter closure of atrial septal defect.
Conclusions
In individuals with ASD, the measured echocardiographic indices of right ventricular systolic and diastolic function are supranormal, consistent with the increased pulmonary blood flow, while those of the left ventricle and septum are within the normal range. Following ASD closure, left ventricular function is preserved but there is impairment of septal function, irrespective of the method of closure. Surgical repair of ASD is associated with impaired systolic and diastolic right ventricular function, while these are preserved following device closure. Although it remains to be seen whether these abnormalities of ventricular function will persist on long term follow up, the short term preservation of right ventricular function supports transcatheter closure of anatomically suitable oval fossa defects as the method of choice.