Article Text

Abstract
Objective: To investigate the central neural contribution to chest pain perception in cardiac syndrome X (angina-like pain, ECG changes during stress, angiographically normal coronary arteriogram).
Subjects: Eight syndrome X patients and eight healthy volunteers.
Methods: Dobutamine stress using echocardiography to assess myocardial function, and positron emission tomography to measure changes in regional cerebral blood flow, as an index of neuronal activity.
Results: During similar doses of dobutamine, syndrome X patients and controls showed comparable regional cerebral blood flow changes in the hypothalamus, thalami, right orbito-frontal cortex, and anterior temporal poles, associated with the sensation of a fast or powerful heart beat. In patients, but not controls, the stress also generated severe chest pain associated with increased activity in the right anterior insula/frontal operculum junction. There were ischaemia-like ECG changes in the syndrome X patients, but no left ventricular dysfunction on echocardiography. Activation of the right insula during chest pain clearly distinguished the syndrome X patients from a group of patients with known coronary disease.
Conclusions: Chest pain and ECG changes were not accompanied by demonstrable myocardial dysfunction in syndrome X patients, but altered central neural handling of afferent signals may contribute to the abnormal pain perception in these patients.
- syndrome X
- chest pain
- regional cerebral blood flow
Statistics from Altmetric.com
It is obvious that pain is an important issue in all branches of clinical medicine. However, the management of pain in general, and chest pain in particular, remains suboptimal in many instances. Improved understanding of the mechanisms of pain would be welcome. In particular, the role of central nervous system abnormalities in maintaining chronic pain syndromes deserves greater attention.1
We have previously studied angina pectoris as a model of visceral pain, by employing functional brain imaging with positron emission tomography (PET) and oxygen-15 labelled water (H215O), measuring regional cerebral blood flow as an index of regional synaptic activity during pharmacologically induced myocardial ischaemia.2 Using this approach, we were able to “map” the neural systems involved in the perception of anginal pain in patients with coronary artery disease.3 Subsequently, the technique was applied to investigate the difference between painful and silent myocardial ischaemia in patients with coronary artery disease.4 As the distinguishing feature between these two populations was cortical activation rather than any demonstrable differences in the heart or in the lower neuroaxis, we concluded that abnormal central nervous system handling of afferent signals might determine the perception of cardiac pain for comparable levels of afferent input. A corollary of this was our hypothesis that abnormal central nervous system handling of afferent signals might on its own produce a syndrome characterised by cardiac chest pain.
Cardiac syndrome X is characterised by angina-like chest pain and ST segment depression on the ECG during stress, although angiographically the coronary arteries appear normal. The quality of the pain and the ECG findings led earlier workers to hypothesise that myocardial ischaemia might account for the features of syndrome X.5 However, the aetiology of chest pain in cardiac syndrome X remains unclear.6 Some studies have shown that myocardial blood flow7 and left ventricular function8 can be within normal limits in this condition, regardless of chest pain or ECG changes, therefore casting doubts on the ischaemic origin of the pain. Additionally, abnormal visceral pain perception has been demonstrated consistently in most syndrome X patients, both in invasive studies9,10 and during pharmacological stress.11 While there is some evidence of autonomic dysfunction in syndrome X,12–14 whether abnormal handling of afferent stimuli by the central nervous system is involved in the perception of chest pain in these patients has not been investigated.
Our aim in the present study was thus to determine whether cardiac syndrome X patients have a distinct pattern of cortical activation during chest pain. To do this, we measured regional cerebral blood flow at rest and during dobutamine induced chest pain in a group of patients with syndrome X and an equal number of matched normal volunteers. The results were also compared with data from patients with known coronary artery disease.
METHODS
Study population
Syndrome X patients
Eight right handed patients (six women, two men; mean (SD) age, 59 (9) years) were recruited consecutively from our clinic over a period of one year. They were normotensive and had a history of typical angina15 on exertion in all cases; three patients also experienced pain at rest. Physical examination was normal in all cases, as were the resting ECG findings. All patients developed > 0.1 mV rectilinear or downsloping ST segment depression on the exercise ECG. Cardiac catheterisation showed angiographically smooth normal coronary arteries. We employed strict exclusion criteria for other cardiac or systemic pathology.7
Control subjects
Eight normal subjects (five women, three men; age 56 (11) years; p = NS v the syndrome X patients) were also studied. None had a history of cardiac or pulmonary disease, or risk factors for coronary artery disease. All had normal resting and stress ECGs and normal effort tolerance.
Stress echocardiography
A few days before PET scanning, patients underwent stress echocardiography with intravenous dipyridamole (0.56 to 0.84 mg/kg). The stress echocardiograms were performed outside the scanner suite under ideal conditions, and normal or enhanced ventricular function was found in all the syndrome X patients. During the PET scanning session, adequate views were obtained to exclude wall motion abnormalities at rest and during dobutamine stress.
PET scanning protocol
Patients refrained from any drug treatment for 24 hours before the scan; β blockers were stopped at least a week before. As we have described previously,3,4 six regional cerebral blood flow measurements were made for each patient using dynamic PET with H215O (regional cerebral blood flow is a reliable index of cerebral glucose consumption, which increases when a given cerebral territory is activated16; the glucose consumption is, in turn, coupled with Na/K dependent ATPase and with neuronal firing rates17,18).
For the patients, an ECAT 931-08/12 positron tomograph (CTI-Siemens, Knoxville, Tennessee, USA), was used. The tracer was given as inhaled C15O2. For each measurement, a 30 second background frame was recorded, then scanning was continued for a further two minutes, during which C15O2 was given at 500 ml/min and 6 MBq/ml activity.19
For the controls, we obtained access to a Siemens 953B positron tomograph (Erlangen, Germany) and used intravenous H215O (10 ml/min and 55 MBq/ml activity over two minutes).
For ethical reasons (radiation exposure using the 953B scanner was ∼5.5 mSv compared with slightly more than 12 mSv on the 931-081/12 scanner for the same protocol), all the controls were studied on the 953B scanner. However, the method of analysis (see below) allowed direct comparison of the various datasets.
All subjects underwent the same series of measurements as follows:
Baseline 1: subject lying on the scanner couch at rest.
Placebo: after six minutes of a placebo infusion of saline. The subjects, who were unaware of the nature of the infused substance, were warned of the possibility of chest pain or sensations in the chest because of the infusion, which was continued throughout the scan.
Baseline 2.
Low dose dobutamine: during an intravenous infusion of low dose dobutamine, 5 μg/kg/min for three minutes and then 10 μg/kg/min for three minutes, the latter continued throughout the scan. Subjects were again blind with respect to the infused substance and were warned as in (2).
High dose dobutamine: during infusion of high dose dobutamine, from 20 μg/kg/min up to a maximum of 35 μg/kg/min, increasing by 5 μg/kg/min increments every three minutes. If chest pain supervened or ischaemia-like ECG changes were noted, the infusion was maintained at the pain inducing (or ECG altering) dose and the PET acquisition was performed. The infusion was continued at this dose for the 2.5 minutes of scanning. (Dobutamine, a β1 agonist, is a positive inotrope and increases cardiac work; it has a short half life, ∼2.4 minutes,20 and it does not cross the blood–brain barrier.21)
Baseline 3: after chest pain had ceased and the ECG had returned to baseline. This was performed in all subjects at least 13 minutes after stopping dobutamine to allow for its complete clearance.
Analysis of PET images
The PET images were realigned and then transformed into a standard stereotactic space.22 The regional cerebral blood flow data were corrected for global regional cerebral blood flow changes and then compared between the different scans of the study by carrying out a series of t tests (or more precisely, a block design analysis of covariance) on a voxel by voxel basis by statistical parametric mapping (SPM™, MRC Cyclotron Unit, Hammersmith Hospital, London, UK).3,4
The regional cerebral blood flow changes induced by the high dose dobutamine infusion were compared with the mean of baselines 1 and 2; the changes induced by placebo and low dose dobutamine were also compared with baseline. Regional cerebral blood flow in the post chest pain phase (baseline 3) was compared with baselines 1 and 2 combined. After within-group analysis for the different groups, a direct comparison of the syndrome X and normal subjects was made. Differences between groups with respect to the areas of increased regional cerebral blood flow during chest pain were computed as interactions of between-group factors (syndrome X v normal controls) and the within-group conditions (high dose dobutamine scan v baselines 1 and 2). As the interaction effect could be predicted by the main effect (high dose dobutamine – baselines 1 and 2) in each group, a less harsh statistical threshold (p < 0.01, without Bonferroni correction) was used for the statistical maps. The resolution of the technique is such that only loci of less than approximately 6 mm cannot be distinguished.19
The same approach was used for a secondary comparison of the syndrome X patients with previously published data from a group of patients with stable angina caused by coronary artery disease3 (seven men, two women, age 61 (7) years; p = NS v the syndrome X patients).
Owing to the nature of the statistical analysis in this study and the signal changes in cerebral blood flow that were being measured (typically ∼5%), the results are considered in the form of pooled datasets for each group of subjects. Intra- and interindividual comparisons are not feasible within the methodology of the present study.
As the data from the coronary artery disease patients had been acquired about two years before those of the syndrome X patients, and those from the syndrome X patients about 1.5 years before those from the normal controls, it was necessary to achieve comparability between the study groups. The syndrome X and normal control data were manipulated in SPM 96, fitted to the SPM 95 template, whereas the secondary comparison between the syndrome X patients and the coronary artery disease patients was performed using SPM 91, the original software used in the first angina study.3 None of the controls in the present study were processed using SPM 91.
Assessment of chest pain
Chest pain was assessed in all subjects as their self rating of the presence and maximum severity of chest pain provoked by the placebo or dobutamine infusions. The pain score was recorded on an arbitrary scale from 0/10 (no chest pain) to 10/10 (unbearable chest pain).7
Ethical considerations
The project was approved by the research ethics committee, Hammersmith Hospital, and the UK Administration of Radioactive Substances Advisory Committee (ARSAC), and accorded with the principles of the Declaration of Helsinki.
RESULTS
Haemodynamic effects of the high dose dobutamine infusion
These data are presented in table 1. The dobutamine infusion was not accompanied by any echocardiographic sign of left ventricular dysfunction in the syndrome X patients.
Characteristics and haemodynamic and pain responses of patients and controls
Pain perception
High dose dobutamine
During the high dose dobutamine infusion, all the syndrome X patients experienced typical severe, retrosternal chest pain, with no radiation to any other site. Two control subjects felt mild throat tightness (but no frank pain). The patients reported that the sensation of chest pain dominated their attention. In contrast, the controls variously described any of the following: awareness of a strong fast heart beat (4/8); neck or throat tightness (2/8); shortness of breath (1/8); or no alteration in sensation (2/8).
In all patients, the severe chest pain experienced was accompanied by ST segment depression of > 0.1 mV on the ECG, whereas the controls' ECGs remained normal (table 1).
Low dose dobutamine
Three of the eight syndrome X patients but none of the controls experienced chest pain during the low dose dobutamine infusion.
Placebo
One syndrome X patient, but none of the controls, felt chest pain during the placebo infusion.
PET findings
Syndrome X
During the chest pain provoked by high dose dobutamine, activity increased in the brain stem, the midline cerebellum, hypothalamus, both thalami, the anterior pole of both temporal lobes, the left and right orbitofrontal cortex, the right insula, and the right premotor cortex (table 2). Low dose dobutamine produced activation in the right thalamus (18, −36, 4; Z = 4.3) and the right prefrontal cortex (46, 26, 8; Z = 4.4). In the baseline scan after the cessation of chest pain, activity was still increased in the left thalamus (−20, −26, 8; Z = 4.1) compared with the earlier baseline scans. There were no differences between the placebo scan and the baseline scans. In addition, the contrasts high dose dobutamine – placebo and high dose dobutamine – baselines 1 and 2 were comparable.
Coordinates of loci of maximum increases in regional cerebral blood flow during chest pain caused by high dose dobutamine compared with baseline (indicated by the highest Z score within each structure)
Controls
During high dose dobutamine, the controls showed activation in the left cerebellum, both thalami, dorsal cingulate cortex, left insular cortex, anterior pole of both temporal lobes, and left and right orbitofrontal cortex (table 2). Low dose dobutamine produced activation in the right thalamus (14, −38, 12; Z = 3.9), left orbitofrontal cortex (−38, 20, −28; Z = 4.4), and right anterior temporal pole (28, 22, −24; Z = 5.2). As with the patients, activity persisted in the left thalamus after cessation of dobutamine (18, −34, 8; Z = 3.7) but there were no differences between the placebo scan and the baseline scans. Also, the contrasts high dose dobutamine – placebo and high dose dobutamine – baselines 1 and 2 were comparable.
Comparison of areas of activation between syndrome X patients and controls
The activity changes evoked by high dose dobutamine compared with baseline in the patients and the control subjects were directly contrasted. The regions in which activations were similar in the two groups are shown in table 3. The main difference in the contrast syndrome X patients > control subjects (that is, areas with increased regional cerebral blood flow in the syndrome X patients but not in the controls) was in the right insular cortex at the junction with the frontal operculum (40, 20, 4; Z = 4.7), with a trend for greater activity in left orbitofrontal cortex (−28, 32, −16; Z = 3.6) (figs 1 and 2). In the contrast control subjects > syndrome X patients (that is, areas with increased regional cerebral blood flow in the controls but not in the syndrome X patients), significant differences were found in the left insula (−28, −6, 20; Z = 4.7) and right anterior cingulate (18, 26, 16; Z = 4.7).
Coordinates of loci of maximum increases in regional cerebral blood flow during high dose dobutamine infusion, common to both the syndrome X patients and the normal control subjects, compared with baseline (indicated by highest Z score within each structure)

Activation of the right anterior insula during dobutamine induced chest pain. This feature distinguishes the syndrome X patients from (on the left) patients with coronary artery disease and (on the right) normal controls. The images are obtained by projecting the results obtained from the SPM analysis onto an MRI template. The colour coding shows degree of statistical significance (Z score) and the physical extent of those volume elements (voxels) in which regional cerebral blood flow was significantly different between the patient groups for the comparison high dose dobutamine v rest. MRI, magnetic resonance imaging; L, left; R, right. For the stereotactic coordinates, see text.

Time course of regional cerebral blood flow changes in the right insula region of interest. The differences in activation between the syndrome X and coronary disease patients (left of figure) and between the syndrome X patients and the normal controls (right of figure) can be seen to occur maximally during day (dy) 5, the high dose dobutamine scan. (The sequence of dynamic scans, dy1–dy6, is as described in the text.) *p<0.001;**p<0.0001. CAD, coronary artery disease; SX, syndrome X.
An interaction test was performed between syndrome X patients and the normal control subjects for the effect of high dose dobutamine infusion compared with baseline, masked using the main effect in the syndrome X patients. The coordinates of loci of maximum increases in regional cerebral blood flow (indicated by highest Z score within each structure) were: brain stem (6, −14, −12; Z = 3.0), right insula at the junction with the frontal operculum (40,20,4; Z = 4.7), left lateral orbitofrontal cortex (−28, 32, −16; Z = 3.6), premotor cortex bilaterally (−56, 6, 20; Z = 3.6 and 50, 12, 8; Z = 4.1), and left medial temporal lobe (−14, 6, −20; Z = 3.3).
Comparison of syndrome X patients v patients with angina due to coronary artery disease
In our earlier study of patients with angina due to coronary artery disease,3 an identical protocol was used and the dobutamine dose given was comparable with that in the present study.
For the high dose dobutamine scan v baseline, activity was significantly greater in the right anterior insula in the syndrome X patients than in the previously studied patients with coronary artery disease. Lesser differences were seen in the cerebellum, right thalamus, and left orbitofrontal, right dorsal frontal, and bilateral prefrontal cortices (table 4; figs 1 and 2).
Syndrome X v coronary artery disease: coordinates of loci of differences in regional cerebral blood flow increases during chest pain caused by high dose dobutamine (indicated by the highest Z score)
DISCUSSION
The conception of cardiac syndrome X has gradually evolved from a paradigm centred upon myocardial ischaemia to one based upon differences in pain perception.23 However, the contribution of the central nervous system to the pain processing has not been examined up to now.
Summary of findings
Syndrome X patients and normal controls had comparable regional cerebral blood flow responses to dobutamine stress, with activation in the hypothalamus, thalami, right frontal cortex, and the anterior temporal poles, associated with the sensation of a fast or powerful heart beat. However, in the syndrome X patients, but not in the controls, the dobutamine stress also generated severe chest pain. This was associated with increased activity in the right anterior insula at the junction with the frontal operculum. Conversely, there was greater activity in the left insula and the right cingulate cortex in the controls. A comparison with our earlier published data from patients with angina due to coronary artery disease3 also showed greater right anterior insular activity in the syndrome X patients during the high dose dobutamine infusion. We therefore believe that activation of the right insula has a significant role in the perception of chest pain in syndrome X. (The insula is known to receive cardiopulmonary inputs; its circuitry and functional correlates have been extensively reviewed by Augustine.24)
The complete absence of echocardiographic evidence of left ventricular dysfunction during the chest pain in the syndrome X patients would argue against the presence of myocardial ischaemia, despite the presence of ST segment depression on the ECG (the significance of which remains uncertain).
Regional differences in brain activation in relation to differences in sensory experience
The sensations experienced in response to dobutamine were different in the normal controls and the syndrome X patients. The former were aware of a rapid heart rate, a percept normally associated with exertion, excitement, or fear, to which subjects would be expected soon to habituate. In contrast, the syndrome X patients had substantial pain. Pain is usually associated with tissue injury and so the perception of pain is likely to be associated with a greater emotional response (fear and anxiety), to which the subject will habituate slowly, if at all. The differences in sensory percepts between groups are likely therefore to be reflected in the different patterns of increased regional cerebral blood flow.
If we had confined our data analysis to a comparison of the syndrome X patients and the normal controls, it might be inferred that this key symptomatic difference—that is, the presence or absence of chest pain—accounted for all the differences in regional cerebral blood flow. However, our comparison of the syndrome X patients with our earlier coronary artery disease patient group,3 all of whom experienced angina of similar severity to that of the syndrome X patients, is crucial. The fact that the differences in regional cerebral blood flow remained significant in this latter comparison shows that the changes were not simply a result of the presence or absence of pain.
Hypothesis about the mechanism of cardiac pain perception
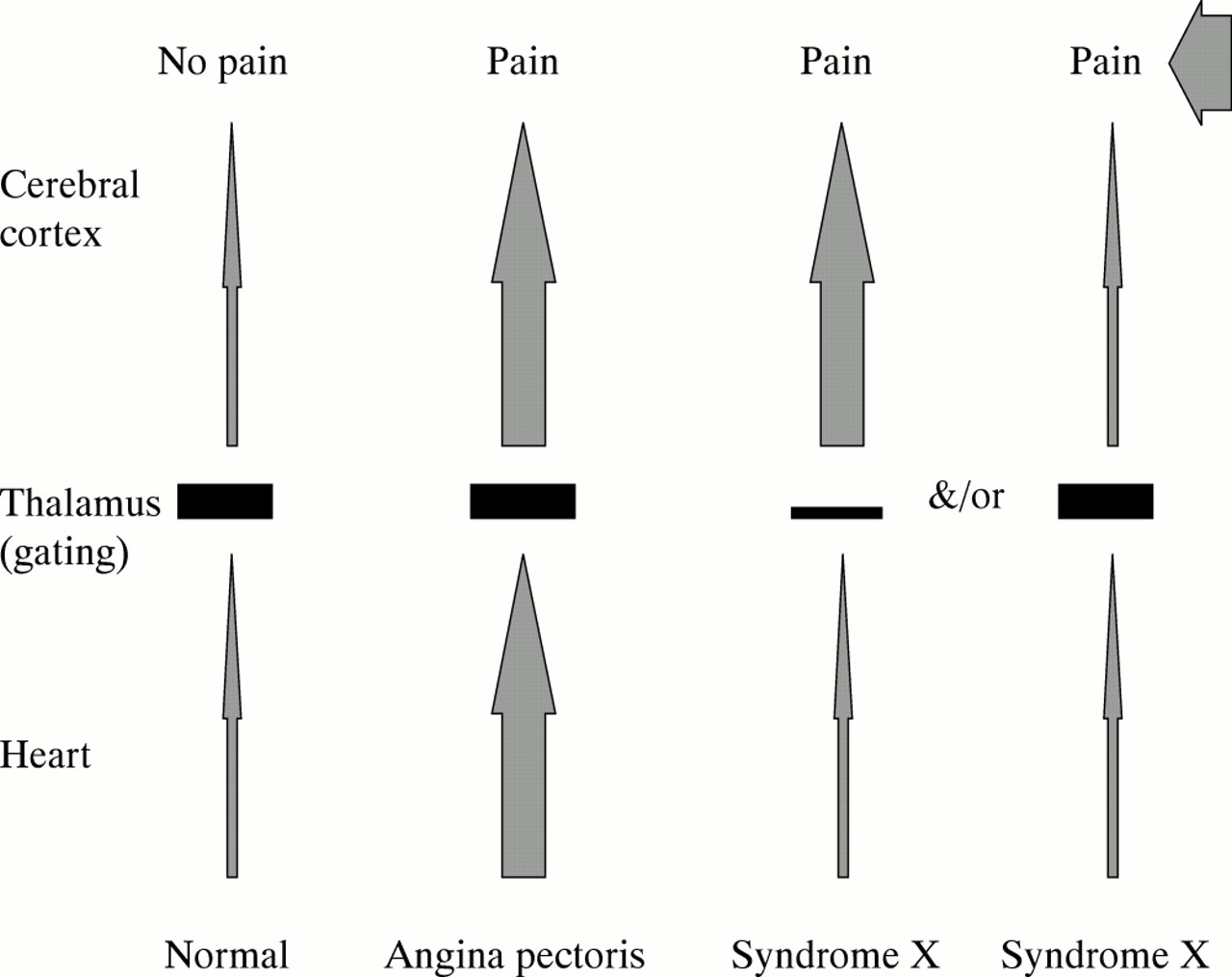
Considering the data from the present study in the light of our earlier studies,3,4 we hypothesise that abnormal central processing of cardiac signals causes or facilitates pain perception during dobutamine stress in syndrome X patients by a central misinterpretation of the increase in firing in afferent nerves. Extending a concept that dates back nearly a century to Colbeck,25 we suggest that changes in myocardial stretch during the increased cardiac work generate the increase in afferent nerve firing. In a normal healthy individual, a continuous stream of afferent stimuli from the heart reaches the brain, but the signals do not reach consciousness—there is no percept. In conditions of true myocardial dysfunction, for example during ischaemia in coronary artery disease, there is a greater intensity of afferent signalling from the heart and a correspondingly greater extent of cortical activation. A percept of pain is thereby generated. The thalamus probably has a key role in the perception of pain from the heart, acting as a gate to afferent pain signals, with cortical activation being necessary for the sensation of pain. From our previous study of patients with coronary artery disease and silent ischaemia,4 we concluded that altered central nervous handling of afferent signals from the heart (an “overactive gate”) might contribute to lack of perception of chest pain in those patients. (This notion has also been advanced by Lenz et al.26)
On the basis of the data in the present study and other work in the field, it is not yet possible to specify the site of any neurophysiological abnormality in syndrome X (whether at the level of the peripheral nerves, subcortical processing, cortical activity, or any combination of these). However, we do know that in our syndrome X patients, the perception of pain is accompanied by greater and more extensive cortical activation than in angina due to coronary artery disease, despite there being no discernible myocardial pathology. One might therefore think of syndrome X as being a type of cortical pain syndrome, a “top down” process, in contrast with the “bottom up” generation of pain caused by myocardial ischaemia in coronary artery disease. The component parts of this mechanism remain to be elucidated—for example, how far an ineffective thalamic “filter” is responsible or to what extent cortical misinterpretation of signals is involved (fig 3). Although the comparison between syndrome X and our historical coronary artery disease patients (table 4) suggests that the cortical element is the main one, the finding that both the syndrome X patients and the normal controls had substantial and equivalent increases in regional cerebral blood flow in the thalamus suggests that the issue is less straightforward.
{kind=link}
{kind=link}
{kind=link}
Schematic description of our hypothesis on the perception of cardiac pain. A full description is in the text.
Further implications of the present study—abnormal autonomic neural regulation
Several groups have reported increased sympathetic activity in syndrome X on the basis of haemodynamic and metabolic evidence12 and heart rate variability data.13,14. This topic has recently been reviewed in detail.23 The central neural abnormalities demonstrated in the present study (especially the left insular activity found in normal subjects but absent in syndrome X patients) may contribute to abnormal autonomic regulation.
Limitations of the study
Potential sex differences
Sex differences in the regional cerebral blood flow response to stress in general, and to dobutamine in particular, could be an important limitation, as our syndrome X population mainly consisted of women, as did our normal control population, while our coronary artery disease patients were mainly men. Although the numbers are very small, we found no difference between the sexes within our normal controls for regional cerebral blood flow changes in the main region of interest (the right insula); there was a small fall in both sexes, compared with a rise among the syndrome X patients. Similarly, with respect to the blood flow changes in the left prefrontal cortex (Brodman area 47, the region with the largest Z score), there was no significant difference between the nine male and three female patients with coronary artery disease.
There have been several studies suggesting sex differences in cerebral activation, but the methodology of some of these has recently been called into question, and a recent study found no differences between the sexes in lateralisation in response to some stressful stimuli.27 In contrast, Paulson et al found greater prefrontal activation in 10 women subjected to a thermal stimulus to the left hand compared with 10 men given the same stimulus,28 although it should be noted that the processing of somatic pain is mediated by distinct pathways.29 Only a new study involving a direct, sex matched comparison between syndrome X patients and coronary artery disease patients would resolve this matter.
Temporal resolution of the scanning method
The scanning mode adopted for this study is such that increases in regional cerebral blood flow were summed over a two minute single frame; the method therefore cannot differentiate afferent from efferent activations.
Differences between the syndrome X patients, coronary artery disease patients, and controls other than the experience of chest pain
The differences between patients and controls extend beyond pain registration and processing and include cognitive and emotional aspects. For example, abnormal laterality of cerebral activation has been demonstrated in coronary artery disease patients during mental arithmetic stress.30
Conclusions
The present hypothesis generating study does not provide all the answers about how pain perception—a complex process involving many structures and activities—is abnormal in patients with syndrome X. However, it is the first study to provide data pointing directly to an involvement of the central nervous system in this disorder and invites further work on the topic.
Acknowledgments
We are very grateful to the British Heart Foundation for their support of this work through BHF project grant No PG/94/039. We should also like to thank Mr Andrew Blythe MSc DCR and Ms Andreana Williams DCR for their help in the acquisition of the PET data.