Article Text

Abstract
Objective: To evaluate the reasons for repeat intervention in patients treated with balloon expandable stents for pulmonary artery stenoses, with particular analysis of the time intervals between interventions.
Design: A retrospective observational study.
Setting: A single paediatric cardiology centre.
Patients: 38 patients, mean age 6.9 years, range 6 days to 34 years (one adult patient); mean weight 19.7 kg, range 2.5–75 kg.
Intervention: Implantation of balloon expandable stents in 46 cases of main pulmonary artery stenosis, right pulmonary artery stenosis, left pulmonary artery stenosis, or right ventricle to pulmonary artery conduits.
Main outcome measures: Adaptation of stent diameter to patient growth; development of pulmonary arteries; pressure gradient in the right ventricle.
Results: 56 stents were implanted in 46 lesions. During a mean follow up time of 2.2 years, 40 repeat dilatations were performed on 28 of 42 reinvestigated stents. A second repeat dilatation was performed on eight stents, and a third on four stents. The mean time period between implantation and repeat dilatations was 15.5 months.
Conclusions: Repeat dilatation of stented pulmonary arteries was done mainly to adapt the stent diameter to the patient’s growth. However, repeat dilatations were also performed to relieve stent obstruction caused by intimal proliferation (17.5%), or to overcome progressive external compression (25%). While most repeat interventions in adult patients are for intimal hyperplasia, in paediatric patients they are needed for a variety of reasons.
- stent
- redilatation
- children
- pulmonary artery
Statistics from Altmetric.com
Stent implantation has become the non-surgical treatment of choice1–4 to overcome the immediate and late results of balloon dilatation of pulmonary artery lesions in paediatric patients.5–7 Stent implantation is carried out on postoperative or native lesions, and most stents are implanted for life. The limited lifespan of bioprosthetic right ventricle to pulmonary artery conduits caused by progressive lumen obstruction can also be treated by transcatheter stent implantation to postpone the need for reoperation.1,2,8
Palliative stenting is possible in neonates and infants with complex cardiac malformations who are at high risk from surgical intervention. For example, stenting of the central pulmonary artery in small patients with pulmonary atresia after interventional radiofrequency assisted valvuloplasty of the atretic valve is an alternative to a palliative aorto-pulmonary shunt operation. In paediatric patients, implanted stents require observation and repeat dilatation as the child grows9 or when there is intimal proliferation or external compression from related structures.8
Our aim in this study was to evaluate the different reasons for repeat dilatation of balloon expandable stents in pulmonary artery stenoses, with particular reference to the time interval between the procedures.
METHODS
Patient population
Thirty eight paediatric patients with 46 pulmonary artery stenoses or obstructions underwent cardiac catheterisation and insertion of a total of 56 balloon expandable stents between February 1994 and November 2000. The procedures were performed at the department of paediatric cardiology, Charité Hospital, Berlin. Informed consent from the parents or patients was obtained in all cases.
After previous ineffective balloon dilatation, patients were considered for stent implantation if they had main pulmonary artery stenosis, significant narrowing of branch pulmonary arteries or distal pulmonary arteries, or right ventricle to pulmonary artery conduits. The diagnoses and lesions are listed in table 1. Fourteen native lesions and 32 postoperative stenoses were treated. Three stents were implanted in a conduit, seven in the main pulmonary artery, 18 in the right pulmonary artery, and 28 in the left pulmonary artery.
Stents and diagnoses
An antiplatelet dose of aspirin was used to prevent thrombosis. During a follow up period of between three months and six years (mean 2.2 years), 42 of 56 stents were reinvestigated by cardiac catheterisation. Forty repeat dilatations were undertaken on 28 of 42 stents in 18 patients. In these 28 stents, repeat dilatation was performed twice on eight stents, and three times on four stents. Two of the 18 patients had a total of three additional stents implanted at the time of repeat dilatation.
Eleven of the 18 patients in whom reintervention was undertaken were female and seven male. Diagnoses included the following: branch pulmonary artery stenoses after repair of tetralogy of Fallot in 10 patients; central pulmonary artery stenoses after interventional radiofrequency perforation of pulmonary artery atresia and stenting of the right ventricular outflow tract in three; left or right pulmonary artery stenoses after a Glenn or Fontan procedure in two; congenital bilateral branch pulmonary artery hypoplasia after repair of truncus arteriosus in one; right ventricle to pulmonary artery conduit obstruction in one; and native peripheral right pulmonary artery stenoses in one.
The mean time between implantation, repeat dilatation, and further dilatation was 15.5 months; the mean gain in weight during these periods was 3 kg.
Special implant techniques
Before the interventional procedure, a balloon angioplasty catheter was gently inflated inside the stenotic area to show the exact shape and size of the lesion by the indentations made in the balloon. To minimise the overlap of stiff stent material and to reduce the amount of foreign material present, the stents chosen for implantation were no longer than was necessary to overcome the stenosis (table 2). Short stents—such as the 12 mm long iliac stent (Palmaz P128)—can be dilated to a diameter of 20 mm,4 which might prevent the need for further surgery. In addition short stents are easier to manoeuvre through the curved course of the right ventricle in small infants (fig 1).
Number of implantations of different stent types (lengths)
Curved course of the catheter used for stenting a left pulmonary artery stenosis in an infant. A 12 mm Palmaz iliac stent is implanted to overcome a circumscribed stenosis.
Between 1994 and 1998, 34 stents were implanted using a long sheath. This technique has been described previously.5,10 Since 1998, we have implanted 22 stents without using a long sheath, thus reducing the sheath size to 7–8 French. Eighteen of these 22 stents were mounted firmly on the balloon in order to minimise stent movement on the balloon when the stent was advanced and positioned in the lesion. In the remaining four cases, Jupiter and Corinthian “IQ” stents were used, which are premounted. The preshaped stiff end of a regular Teflon coated guide wire (“TSF”, Cook Europe, Bjaeverskov, Denmark) was positioned in the peripheral pulmonary artery distal to the lesion, as a secure guide for the balloon/stent assembly when it was being manipulated across the right ventricular outflow tract to the point of narrowing. This stiff guide wire also facilitates manipulation of the stent through the right ventricle while it is advanced to the lesion—especially important in the case of left pulmonary artery placement because of the tortuous access route. This technique potentially reduces damage to the vessel, an important consideration in small infants with the likely need for several redilatations during their lifetime.
Techniques of repeat dilatation
During repeat dilatation for growth the stents were dilated to a diameter larger than that of the native unstenosed vessel, to allow growth of the vessel by improving the blood flow across the stent. Repeat dilatations were undertaken according to the patient’s somatic growth, whether or not there was intimal hyperplasia.
In patients with stent obstruction because of external compression, repeat dilatations were done with the same size of balloon as was used for the initial implantation. In some patients we implanted an additional stent inside the pre-existing stent in order to reinforce it and make it less susceptible to external compression.
RESULTS
Implantation of 56 stents was performed on 38 patients (20 male, 18 female) with 46 lesions. Age ranged from six days to 34 years (the single adult patient), with a mean of 6.9 years; weight ranged from 2.5–75 kg, mean 19.7 kg. We implanted 52 Palmaz stents (Johnson and Johnson Interventional Systems, Sommerville, New Jersey, USA), three Corinthian “IQ” (Palmaz, Corinthian Peripheral PC 125 PPS, Roden, Netherlands), and one Jupiter “IQ” stent (Palmaz, Netherlands). The length of the stents ranged from 7–40 mm (table 2).
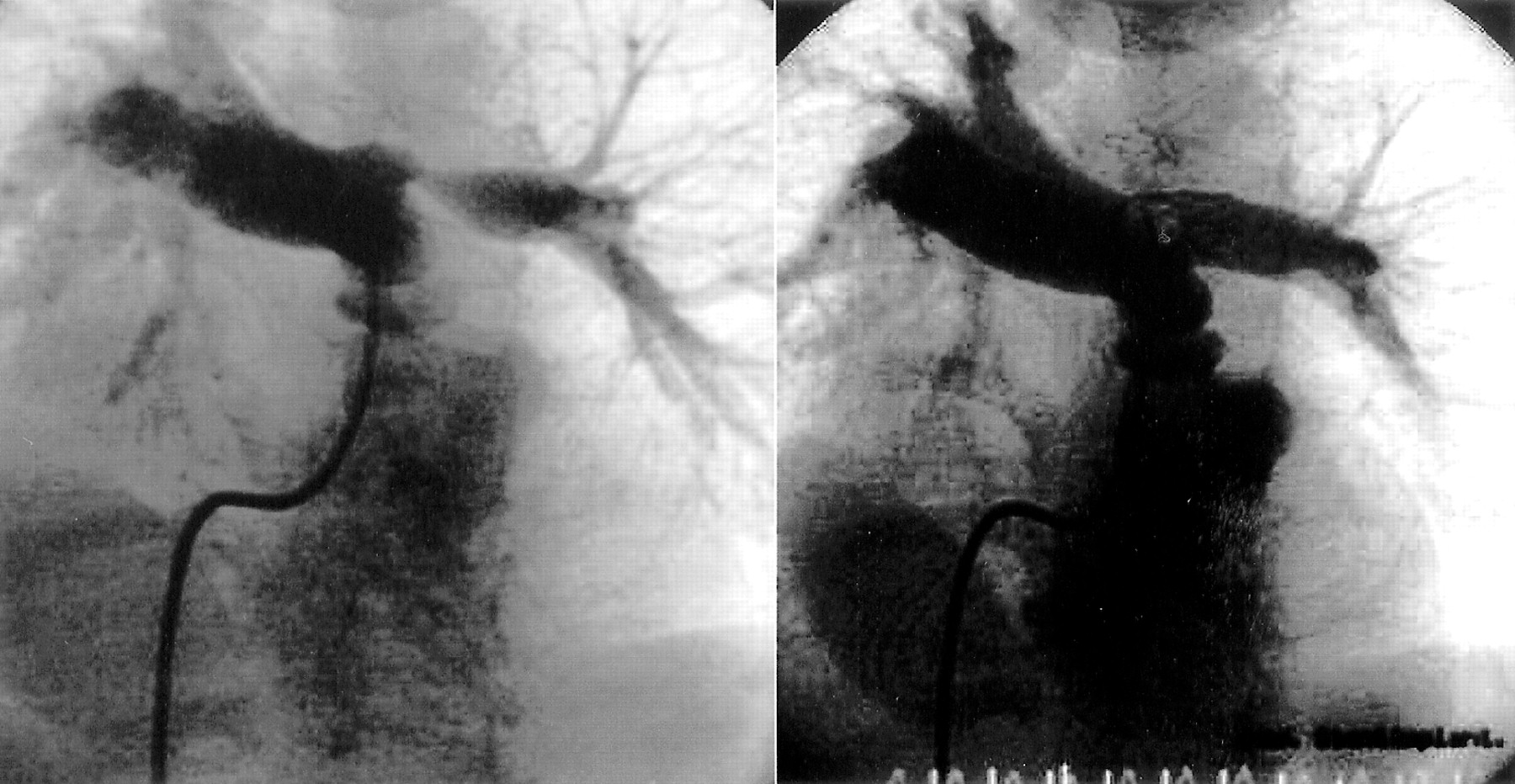
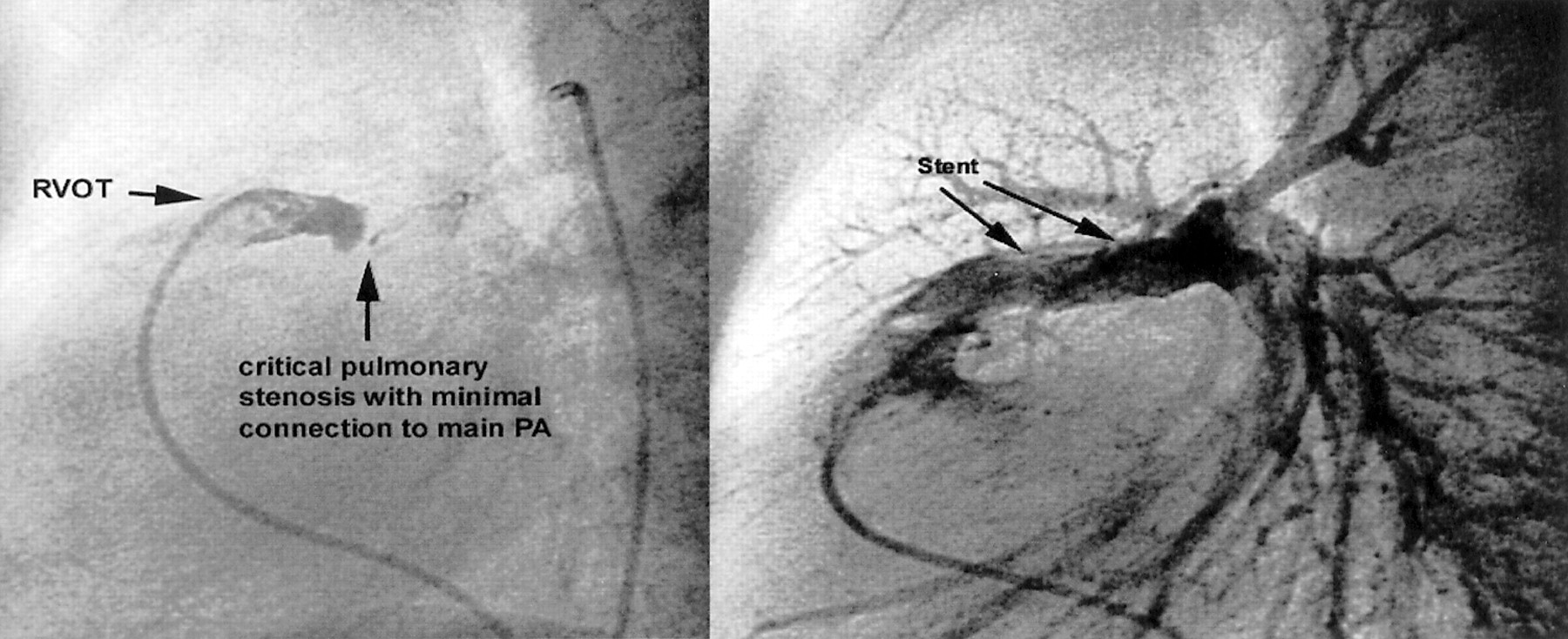
Ten stents were implanted in the main pulmonary artery in six patients; six of these 10 stents were in “native lesions” (fig 2), five of these six stents after interventional radiofrequency treatment of pulmonary atresia.

Stenting of native main pulmonary artery stenosis in a child with tetralogy of Fallot, hypoplastic pulmonary arteries, and major aortopulmonary collateral arteries, before stent implantation (left panel) and after implantation (right panel).
Twenty eight stents were used to treat 22 left pulmonary artery stenoses. Five of these were in native stenoses and 23 were for treating postoperative lesions.
We used 18 stents in 17 patients with 18 right pulmonary artery stenoses. Six of these were for treating native right pulmonary artery stenosis.
The ratio between the diameter of the implanted stent and the diameter of the stenosed vessel varied between 1.3 and 12 (mean 3.1); the ratio between the diameter of stent and that of the surrounding normal vessel varies between 0.8 and 2.4 (mean 1.1).
Acute complications
One stent did not open in its central part, causing rupture of the balloon in a right pulmonary artery stenotic lesion. The stent was withdrawn into the right ventricle but could not be removed across the tricuspid valve. It was finally placed in the apex of the ventricle without causing any rhythm disturbance. The stent is still in place after a follow up period of six years (fig 3); there have been no sequelae so far.
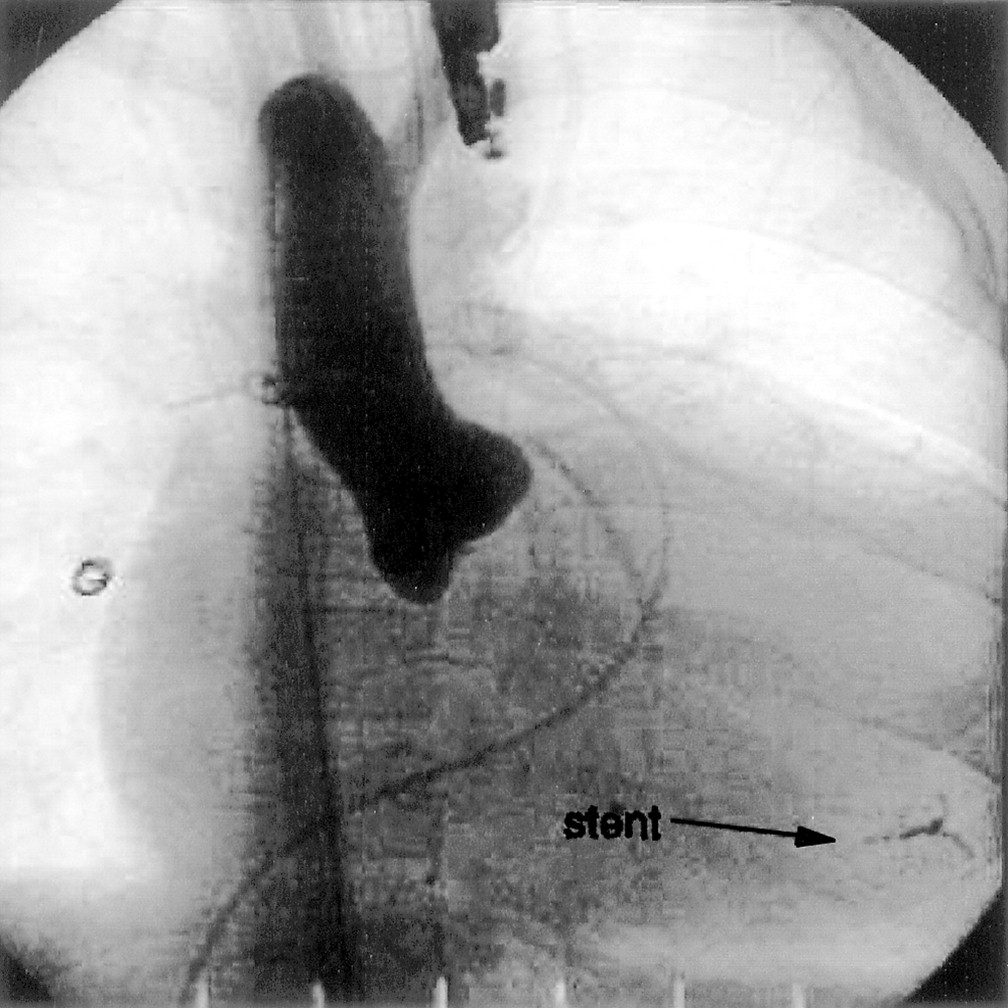
Embolised stent in the right ventricle. The stent has remained in the same position for six years.
Non-acute complications
One stent caused a small false aneurysm (fig 4) two months after main pulmonary artery stenting in a child with transposition of the great arteries and a ventricular septal defect. The patient subsequently underwent a two stage arterial switch operation with a right ventricle to pulmonary artery conduit. The stent was surgically removed and replaced by a new conduit.

Aneurysm formation four months after stenting of a right ventricle to pulmonary artery conduit.
A patient with a right ventricle to pulmonary artery conduit had severe stenosis because of external compression of the conduit against the posterior aspect of the sternum. This was treated by three concentrically overlapping stents. At the time of last repeat dilatation the struts of the outer stent were noted to be fractured8 but were completely covered by the inner stents.
Two patients died during the follow up period. One died of septicaemia six weeks after a Glenn procedure and three weeks after implantation of two stents in a left pulmonary artery stenosis. The other patient, with complex cardiac lesions, died at home six months after stent implantation in the main pulmonary artery. The precise cause of death was not established. It is felt that neither of these deaths was directly related to the stent procedures.
During a follow up period of between three months and six years (mean 2.2 years), nine of the 56 stents were removed surgically. Three were removed after perforation of pulmonary atresia and palliative stenting of the main pulmonary artery. One was removed during heart transplantation. Five were explanted during repeat right ventricle to pulmonary artery conduit implantation. In one of these patients an aneurysm developed after stenting of an obstructed conduit (fig 4). Forty two stents were reinvestigated by cardiac catheterisation; 40 repeat dilatations were performed on 28 of these 42 stents. The mean time period between implantation and repeat dilatation was 15.5 months, and the mean weight gain during that period was 3.0 kg. In eight of the 28 stents subjected to repeat dilatation the procedure was done twice, and in four three times. The details of the repeat dilatations are given in table 3.
Details of repeat interventions: time interval, gain in weight, and stent to balloon ratio
Reasons for repeat dilatation
Twenty three of the 40 repeat dilatations (57.5%) were performed for somatic growth. Stents in the right pulmonary artery were dilated six times, in the left pulmonary artery 14 times, and in the main pulmonary artery three times. Dilatation was done using a balloon size that was 0–50% (mean 24%) larger than the diameter of the neighbouring normal vessel.
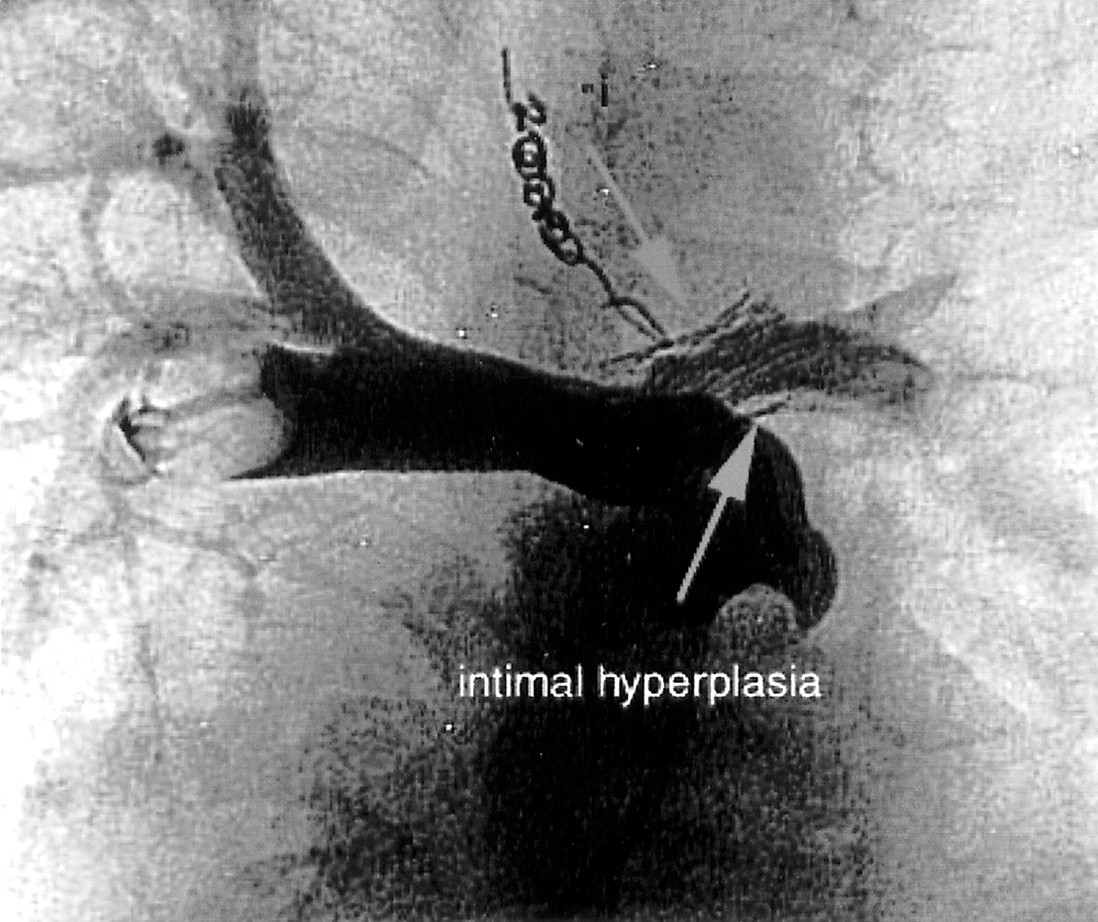
Seven of the 40 repeat dilatations (17.5%) were done because of intimal hyperplasia (fig 5) in four stents. One stent was redilated twice, another three times. All these overdilated stents were in the left pulmonary artery. The balloon diameter was chosen to be 20–30% (mean 26%) larger than the diameter of the adjacent normal vessel.
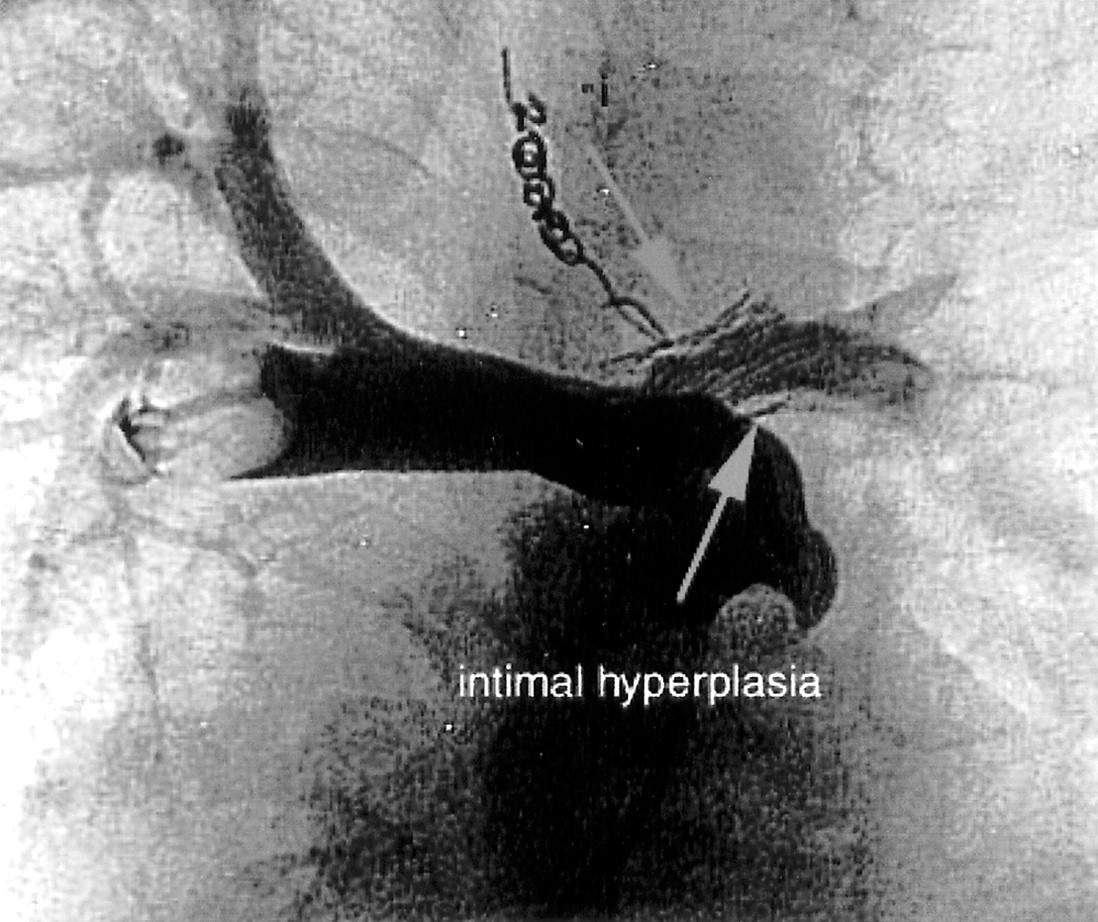
Intimal hyperplasia in a left pulmonary artery stent seven months after implantation in an 8 month old infant.
Ten of the 40 repeat interventions (25%) were done for external compression on five stents in the main pulmonary artery. Two stents were redilated twice after interventional radiofrequency perforation of right ventricular outflow tract occlusion. In a right ventricle to pulmonary artery conduit obstruction, two additional stents were implanted subsequently, and each of these three stents was redilated during three repeat interventions to overcome the external compression. The balloon diameter for repeat dilatation of those restenoses did not exceed that of the conduit.
The mean period between implantation and repeat dilatation or repeat stent implantation to compensate for growth was 20.5 months; to treat intimal hyperplasia, 14.2 months; and to treat external compression, 4.6 months.
Repeat dilatation to compensate for growth was undertaken the most aggressively, with a mean balloon to vessel ratio of 1.24 (fig 6); in patients with intimal hyperplasia the mean ratio was 1.26. External compression was treated by redilatation with or without additional stent implantation with a balloon to vessel ratio of 1.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Hypoplastic left and right pulmonary artery in a 3 month old infant after surgical correction of truncus arteriosus (left panel). Middle panel: the same patient at the age of 7 months, four months after stent implantations in the left and right pulmonary artery and after the first redilatation; the stent to vessel ratio on the right side was chosen to be 1.5:1 to allow for expected growth. The right panel shows the result one year after the first redilatation.
DISCUSSION
Compared with balloon dilatation alone, stent implantation in pulmonary artery stenosis yields better early and mid term results.6,7,11 In the paediatric population most implanted stents are intended to function lifelong. Follow up investigations and invasive assessments during the growing years are thus prudent. Intimal hyperplasia is the usual reason for repeat dilatations of implanted stents in adult patients,12 but there are various reasons for repeat dilatation in children.
In our group of patients, with a follow up time of three months to six years, all the implanted stents remained open. Though the number of patients in our study was relatively small, we found three different reasons for repeat interventions on stents implanted in pulmonary artery stenoses in the paediatric population.
The principal reason (in 57.5% of the procedures) was to adapt the stent diameter to the patient’s growth. This was done at a mean of 20.5 months after implantation. We performed repeat dilatations in these patients with a considerably larger balloon than was used during implantation. Our hope was that more aggressive dilatation would encourage the growth of the vessel distal to the stent. At the time of stent implantation the ratio of stent to vessel diameter was 1.0. On repeat dilatation, the mean ratio was increased to 1.24. Figure 6 shows a case of bilateral branch pulmonary artery hypoplasia in an infant after surgical repair of truncus arteriosus. At the age of three months, stents were implanted in both pulmonary branches. The first redilatation was done four months after implantation. At this time the balloon to vessel ratio was chosen to be 1.5 in anticipation of subsequent growth. One year after the first redilatation, the diameter of the right pulmonary artery had increased to that of the redilated stent.
The second reason for redilatation was restenosis because of intimal hyperplasia.13 This occurred in 17.5% of the procedures after a mean time of 14.2 months. Intimal proliferation,9,13 defined as an intimal lining of more than 20% of the inner lumen, was only noted after stenting of left pulmonary artery stenoses. Four of 14 repeat stent dilatations in this position were done because of intimal hyperplasia. The balloon to vessel ratio in these redilatations was 1.26—nearly the same as that used to compensate for growth. In two cases a single stent was implanted in the left pulmonary artery stenosis; a third patient received two stents, overlapping by 5 mm. However, in eight other patients in whom two or three stents were placed in main, left, or right pulmonary artery stenoses, intimal hyperplasia did not occur. An explanation for the presence intimal hyperplasia in some cases but not others could be the presence of residual duct tissue,14 which provokes intimal proliferation. Severe intimal hyperplasia after stenting of a right pulmonary artery stenosis was described by Ing and colleagues in a previous report.9 These workers used two stents and noted a pronounced intimal waist at the site of a 2.5 mm overlap. They cited an animal model of Tominaga and colleagues,15 who theorised that gaps between the wires of the stents might prevent a neointimal reaction by allowing more rapid endothelialisation of the stents, with a potential reduction in subacute thrombus deposition.
The third reason for redilatation (two patients; 25% of the procedures) was to overcome progressive external obstruction. In one case the patient was an adult with right ventricle to pulmonary artery homograft; in the other, the patient was a neonate who had suffered interventional perforation of a long segment pulmonary atresia. In these two cases stent implantation was performed as a palliative procedure to decrease the number of operations required.
The time to reintervention for external compression was considerably shorter (at 4.6 months) than the time to reintervention for other reasons, as restenoses because of external compression occurred relatively quickly. The balloon used for repeat intervention was the same size as that used for the initial implantation. In the adult patient, deployment of two additional stents was necessary to overcome rigid obstructive tissue, as described previously by Powell and colleagues.8 The lifetime of multiple stented conduits is unpredictable and further stent implantation may become necessary. In future new stent technology with increased radial strength might lessen the problem of restenosis caused by external compression.
Conclusions
Invasive follow up investigations on implanted stents in paediatric patients with pulmonary artery stenoses should be performed on a regular basis. Restenoses caused by intimal hyperplasia, growth of the patient, or external compression can be treated by repeat dilatation or repeat stent implantation.
Repeat dilatation or repeat stent implantation is feasible, safe, and effective with balloon expandable stents. More aggressive repeat dilatation to adapt the stent to expected future somatic growth—irrespective of possible intimal hyperplasia—may also promote growth in the vessel distal to the stent by increasing the blood flow in the vessel. In patients with stent obstruction caused by external compression, multiple stent implantations can be undertaken to overcome the external compressive forces. Further clinical experience and follow up will be required to determine the long term or lifetime benefits of stent implantation in the paediatric population.
Acknowledgments
We thank Dr Neil Wilson for his kind help in preparing this paper.