Article Text

Abstract
Background: Conventional contrast cineangiography and intravascular ultrasound (IVUS) provide a limited definition of vessel microstructure and are unable to evaluate dissection, tissue prolapse, and stent apposition on a size scale less than 100 μm.
Objective: To evaluate the use of intravascular optical coherence tomography (OCT) to assess the coronary arteries in patients undergoing coronary stenting.
Methods: OCT was employed in patients having percutaneous coronary interventions. Images were obtained before initial balloon dilatation and following stent deployment, and were evaluated for vessel dissection, tissue prolapse, stent apposition, and stent asymmetry. IVUS images were obtained before OCT, using an automatic pull back device.
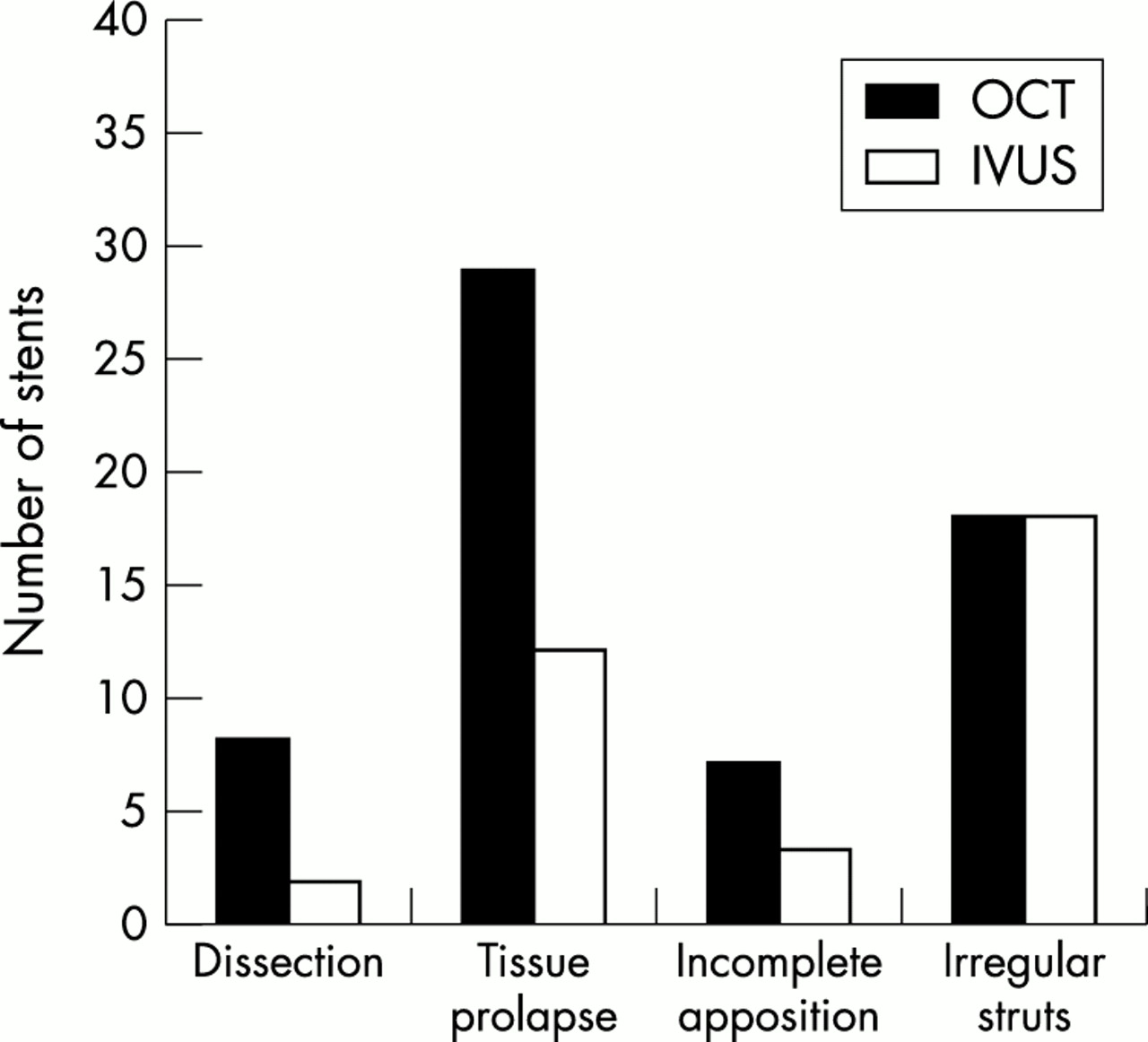
Results: 42 stents were imaged in 39 patients without complications. Dissection, prolapse, and incomplete stent apposition were observed more often with OCT than with IVUS. Vessel dissection was identified in eight stents by OCT and two by IVUS. Tissue prolapse was identified in 29 stents by OCT and 12 by IVUS; the extent of the prolapse (mean (SD)) was 242 (156) μm by OCT and 400 (100) μm by IVUS. Incomplete stent apposition was observed in seven stents by OCT and three by IVUS. Irregular strut separation was identified in 18 stents by both OCT and IVUS.
Conclusions: Intracoronary OCT for monitoring stent deployment is feasible and provides superior contrast and resolution of arterial pathology than IVUS.
- stent
- imaging
- tomography
- IVUS, intravascular ultrasound
- OCT, optical coherence tomography
Statistics from Altmetric.com
Advancements in stent design, improved antiplatelet treatment, high pressure dilatation, and intravascular ultrasound (IVUS) imaging have dramatically changed interventional cardiology. Based in part on the success of these innovations, the use of stents for percutaneous revascularisation has increased dramatically in recent years. IVUS imaging has played an important role in understanding failure and optimising outcome in stent treatment. Key insights from IVUS have included the role of negative remodelling in late lumen loss1,2 and the significance of complete expansion and apposition.3 However, owing to its relatively low resolution (100–150 μm), IVUS does not provide detailed structural information that could improve our understanding of the mechanisms of acute complications and restenosis. Additionally, the high echogenicity of stent struts makes it difficult to evaluate adjacent structures such as small dissections and tissue prolapse.
Optical coherence tomography (OCT) is an optical analogue of IVUS, with improved resolution (10 μm) and contrast. Previous studies have demonstrated the feasibility of catheter based intravascular OCT in obtaining qualitative information about arterial anatomy both in vitro and in vivo.4–9 Imaging in vitro has shown an excellent correlation between plaque characterisation by OCT and histology.5 Catheter based OCT images have detected post-angioplasty dissection in porcine coronary arteries,7 and recent results suggest that OCT may provide sufficient information to characterise plaque type in living patients.9 Our aim in this study was to determine the feasibility and applicability of using intravascular OCT to assess the acute effects of coronary stenting.
METHODS
Patient and lesion population
Forty patients were enrolled in the study, 30 men and 10 women (mean (SD) age 60 (9) years, range 42–79 years). The indication for intervention was progressive or unstable angina in 23 patients (one had previous stenting), and acute myocardial infarction in 17. In all, 42 lesion locations were imaged, including the left anterior descending coronary artery (n = 10), the circumflex coronary artery (n = 8), and the right coronary artery (n = 24).
The study was approved by the institutional review board of the Massachusetts General Hospital.
Stent deployment and imaging
Coronary interventions were undertaken in a standard manner over a 0.014 inch (0.36 mm) guide wire through a 6 or 7 French guiding catheter. The selection of the predilatation balloon and stent size was based on visual estimation, using the guide catheter for calibration. IVUS and OCT imaging were done before balloon dilatation and were repeated at the end of the procedure.
The IVUS catheters used in this study incorporated a single 30 or 40 MHz transducer within a 3.2 or 3.0 French (respectively) short monorail sheath (Ultracross or Atlantis, Boston Scientific, Natick, Massachusetts, USA). The IVUS catheter was advanced distal to the lesion and a motorised, constant velocity (0.5 mm/s) pull back was used to image the artery retrograde to the coronary ostium. The location of the catheter transducer was documented at the initiation of pull back with angiography. IVUS images were displayed in real time on a video monitor and recorded to S-VHS video tape for subsequent analysis. Quantitative analyses were performed off-line using software in the IVUS system and with image processing software (IPLab Spectrum 3.1, Signal Analytics, Vienna, Virginia, USA).
The OCT system used in this study has been described previously.10 OCT images were acquired at either eight frames a second (250 angular pixels × 250 radial pixels) or four frames a second (500 angular pixels × 250 radial pixels), displayed with a grey scale lookup table, and digitally archived. OCT catheters were constructed using modified 3.0 or 3.2 French short monorail IVUS catheters identical to those used for ultrasound imaging. Key modifications included the insertion of a single mode optical fibre through the IVUS flexible shaft, and distal termination of the optical fibre by a miniature gradient index lens and prism.
Following IVUS imaging, the OCT catheter was advanced over the guide wire and placed at the culprit lesion. Three locations were imaged per lesion: distal and proximal shoulder regions and the area of greatest stenosis or ulceration within the plaque. All imaging locations were documented using contrast angiography. At each location images were acquired while saline (8–10 ml) was introduced through the guide catheter by hand injection to temporarily displace blood. Following stent deployment, OCT imaging was done in a similar manner, placing the catheter at three locations within the stent. OCT images were displayed in real time using a video monitor and archived digitally for subsequent analysis. Quantitative analyses were undertaken using the same software as used for the IVUS images.
Image analysis
Previously described methods11 for correlating IVUS images before and after stenting and for correlating IVUS images with angiography were employed and extended to incorporate the OCT data. In this study, the OCT imaging site identified by angiography was taken as the evaluation site for IVUS. Image processing software was used to measure the angiographic longitudinal distance along the vessel from the OCT imaging locations to reproducible landmarks (side branches, aorto-ostial junction, and perivascular anatomy). These measurements were subsequently used to identify the corresponding IVUS images. In IVUS imaging, the location of the catheter at the initiation of pull back was documented with angiography. The video recording of IVUS images during the pull back contains a time stamp which, when multiplied by the translation velocity, yields the catheter location for each frame. In the case of post-stent imaging, the longitudinal edges of the stent were used as the registration landmarks.
The registered IVUS and OCT datasets were evaluated for the presence of dissection, tissue prolapse, incomplete apposition of the stent to the vessel wall, and irregular stent strut distribution. The IVUS reviewer was blinded to the results of angiography and OCT. The OCT reviewer was blinded to the results of angiography and IVUS. The IVUS data were reviewed under real time and stopped frame playback within a six second window (3.0 mm under constant velocity pull back) around the location of OCT imaging. Dissection was defined as an arterial disruption within or adjacent to the stent where a flap of tissue could be clearly differentiated from the underlying plaque.12 Prolapse was defined as protrusion of tissue between stent struts extending inside a circular arc connecting adjacent struts. The distance from the arc to the greatest extent of protrusion was taken as a quantitative measure. Incomplete apposition was identified as clear separation between at least one stent strut and the vessel wall.
Although post-deployment stent asymmetry with IVUS has not been found to be predictive of restenosis,13 recent work has suggested that IVUS criteria for asymmetry (minimum stent diameter/maximum stent diameter) may not reflect local stent induced strain.14 Schulz and colleagues found that the correlation between the variation in interstrut spacing and local neointimal thickness was as strong as that between vascular injury and neointimal thickness.14 Based on this work, we defined irregular stent strut distribution as a variation in interstrut separation greater than 200%.
RESULTS
Forty patients were enrolled in the study. The IVUS and OCT catheters were successfully passed in all patients before stenting. Following stenting, the IVUS catheter would not pass the stent in one patient; no OCT imaging was attempted in this case. In the 39 patients in whom IVUS and OCT studies were completed, 42 lesions were evaluated with no complications. The time span of clear OCT imaging during administration of saline averaged 2.8 seconds (range 1.8–6.0 seconds). The efficiency of the flush was influenced by several factors, including the distance between the lesion and the guide catheter, the degree of stenosis at the lesion, and the presence of prominent vessel side branches proximal to the lesion.
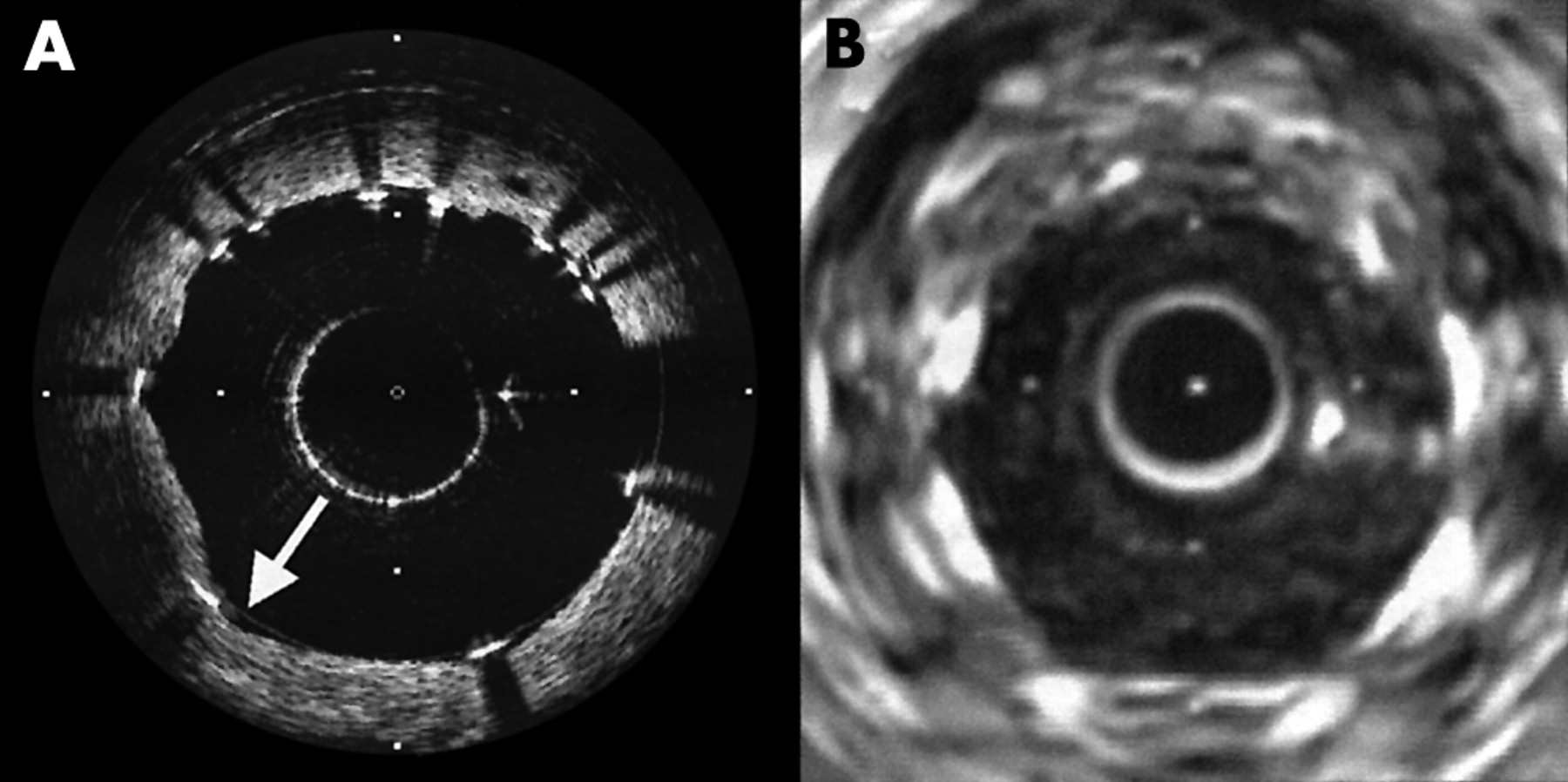
A summary of the findings by OCT and IVUS is presented in fig 1. The visualisation of dissection following stent deployment with IVUS and OCT can be complicated by the opacity of the stent struts. Imaging undertaken immediately after balloon dilatation but before stent deployment, however, often showed severe disruption of the vessel wall (fig 2). Dissections of the vessel wall were observed by OCT in eight cases following stent deployment (fig 3). In two of these cases, dissection was also observed by IVUS.
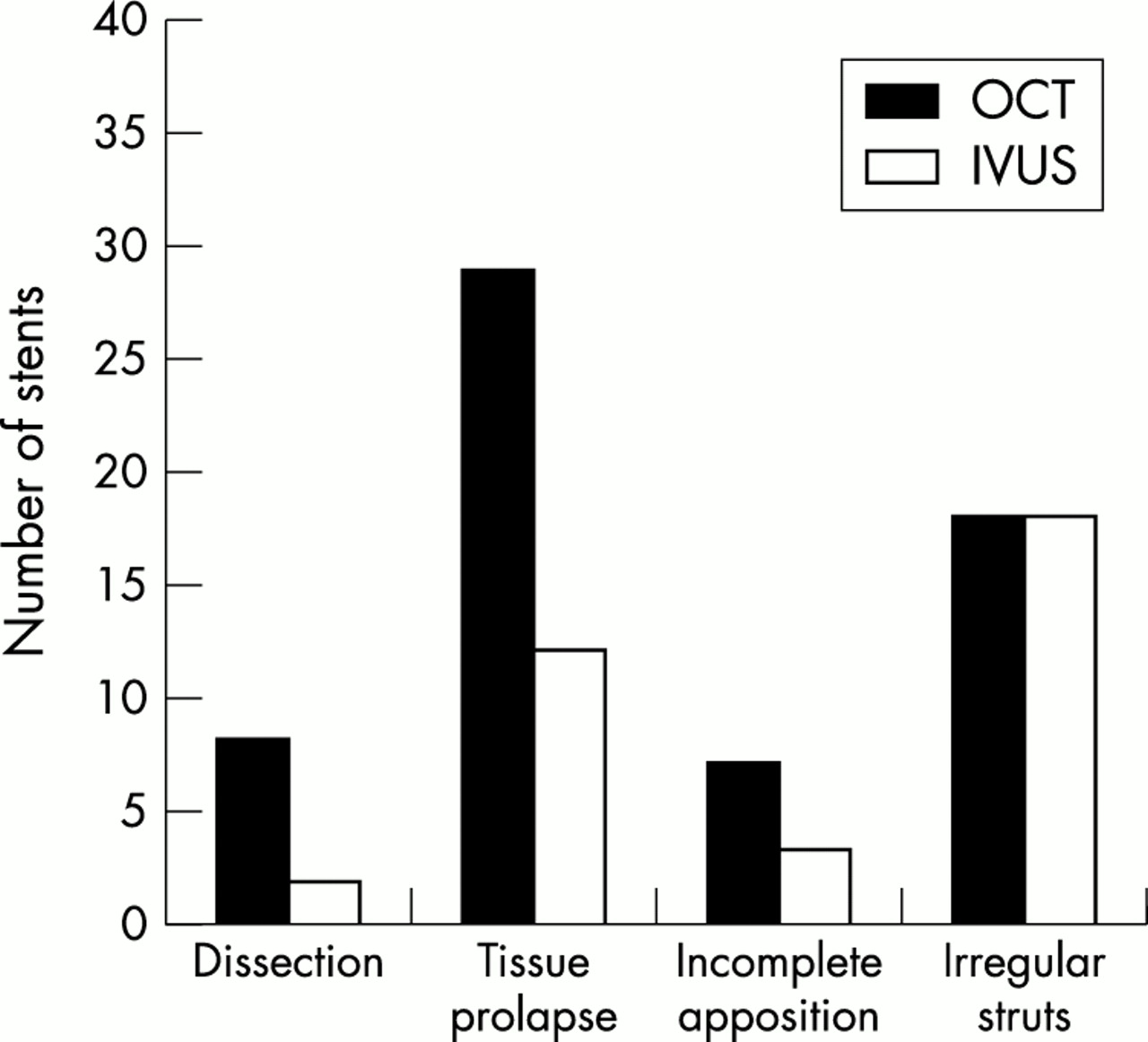
Summary of observations with optical coherence tomography (OCT) and intravascular ultrasound (IVUS): 42 stents were imaged in 39 subjects.
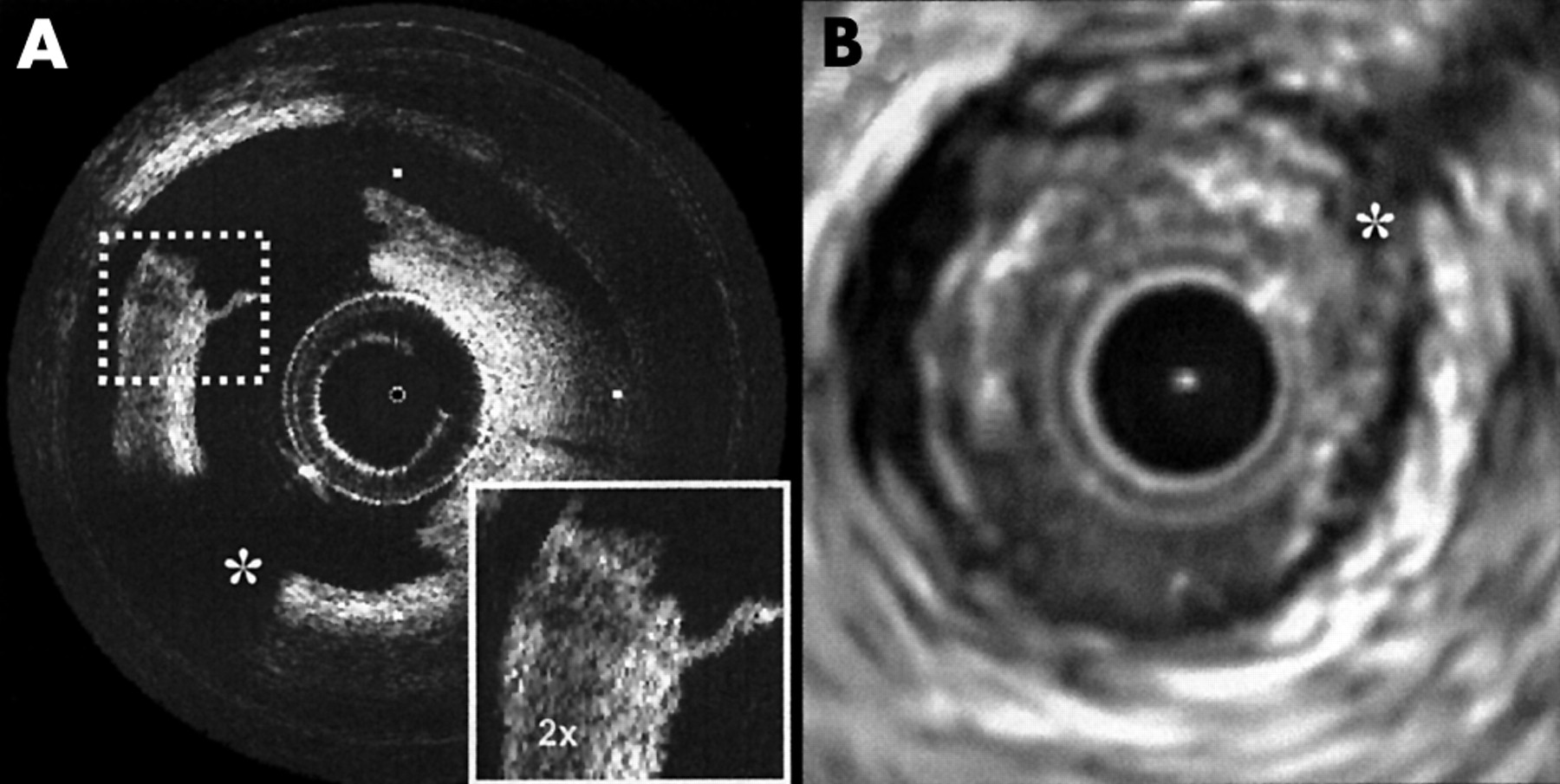
Dissection observed with optical coherence tomography (OCT) (A) and intravascular ultrasound (IVUS) (B) following balloon dilatation. Although the tissue flap can be seen in the IVUS image, it is difficult to determine the depth of dissection. In the OCT image, the bright-dark-bright banding within the flap suggests involvement of the adventitia. In each image, tick marks represent 1.0 mm, and the guide wire location is denoted by an asterisk. Following stenting, the disrupted tissue was held in place and a patent lumen was observed.

(A) Optical coherence tomographic image of a stent showing minor dissection (∼250 μm in depth) between stent struts at 6 o’clock. The individual struts appear as opaque bands at the vessel surface. The guide wire obstructs the view from 8 to 9 o’clock. The characteristic structure of a layered fibrous plaque is evident between the struts from 11 to 3 o’clock. (B) Corresponding intravascular ultrasound image. The guide wire in this image is at ∼8 o’clock. A minor dissection is evident at 6 o’clock.
Tissue prolapse between stent struts was often observed by OCT (n = 29), but less often by IVUS (n = 12, coincident with OCT) (fig 4). The magnitude of prolapse averaged 242 (156) μm (range 50–500 μm) measured by OCT, and 400 (100) μm (range 200–500 μm) by IVUS. Incomplete stent deployment was observed in seven stents with OCT and in three stents with IVUS (all coincident). The mean spacing between the struts and the vessel wall in these stents was 186 μm, with a standard deviation of 144 μm (range 100–500 μm) measured by OCT. In 18 stents, the struts were found by both OCT and IVUS to be arrayed in an non-uniform pattern, having small interstrut spacing in one sector and comparably larger spacing in opposing sectors (fig 5).

(A) Optical coherence tomographic image showing tissue prolapse (filled arrow at 7 o’clock, measuring 340 μm). At 2 o’clock (open arrows) the stent is under deployed by 100 μm. Neither of these small features is readily apparent in the corresponding intravascular ultrasound image (B).

Stent having irregular spacing between adjacent struts acquired with optical coherence tomography (A) and with intravascular ultrasound (B). At locations of greater strut separation, the pronounced angulation observed in the vessel wall (arrow in A) may correspond to increased focal stress.
To test for an association between observed dissection, prolapse, incomplete apposition, and irregular strut distributions, Fisher’s exact test was applied to all pairings of observations in the OCT data. The results suggest that tissue prolapse was associated with irregular struts (p = 0.0011), but no other significant associations were identified (p > 0.24 for all other pairs).
IVUS and OCT imaging was performed in one case of in-stent restenosis. Before the intervention, eccentric neointimal proliferation was observed with both modes (fig 6). As in the 42 de novo stents imaged in this study, the superior contrast and resolution of OCT allowed precise determination of strut location and the relation of the strut to the vessel wall. In the case depicted in fig 6, the maximum thickness of neointima within the stent was measured by OCT to be 430 (10) μm.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Optical coherence tomography (OCT) (A) and intravascular ultrasound images (B) of a patient with in-stent restenosis. In the left portion of the OCT image (3 o’clock to 12 o’clock) neointimal growth is seen inside of the stent struts. Two guide wires, denoted by asterisks, were used in this procedure.
DISCUSSION
In this study we evaluated the feasibility and applicability of OCT for monitoring stent deployment compared with IVUS. Images obtained with both methods from corresponding locations provide a basis for evaluating the ability of OCT to identify important features, including dissection, prolapse, apposition, and irregular stent struts. The high resolution and contrast of OCT appear to provide significantly more detailed morphological information than IVUS, and it may prove superior for assessing stent deployment. The relatively coarse resolution of IVUS (> 100 μm) implies that prolapse with a radial extension within the stent of less than 100 to 200 μm (one to two picture elements) may go undetected. This has two implications for our measurements. First, the incidence of prolapse may be underestimated by IVUS. Second, the average extent of the prolapse will be overestimated owing to the decreased sensitivity for prolapse of lower magnitude.
The increased frequency with which small detailed features are observed with OCT compared with IVUS is not surprising, considering the superior resolution of OCT. The clinical relevance of these observations, however, is not yet determined. Although IVUS guidance of stenting initially led to significant changes in clinical practice,3 subsequent multicentre trials have shown only modest benefits.15–18 In a recent study,19 minor tissue prolapse identified by IVUS was not found to be associated with late angiographic in-stent restenosis. The correlation between local vessel injury and in-stent restenosis identified in animal models20–22 and human cadaver studies23 suggests, however, that an improved ability to monitor stenting may be beneficial in understanding restenosis and in developing improved therapeutic strategies. Recent results also suggest that OCT may provide more information on plaque composition before treatment than IVUS.9 The non-uniform resistance to balloon expansion in eccentric plaques or plaques of complex composition may result in asymmetrical stent deployment.24,25 Considering the varied inflammatory response to stenting for different plaque types,23 combined pre-stent and post-stent monitoring with OCT warrants further investigation.
Limitations
The OCT imaging system and catheters used in this study constitute a prototype research device. In developing the catheters, emphasis was placed on safety rather than on technical capability. Future embodiments will probably take advantage of size reductions and increased flexibility of the catheters, as well as increased scanning depths. Delivery of saline through the guide catheter in order to displace blood is inefficient, especially in the case of distal vessel segments with occlusive lesions and prominent side branches. The system used in this study was not capable of imaging over extended longitudinal segments. Imaging was undertaken at three discrete locations within the lesion before treatment and within the stent following deployment. The frequency with which dissection, tissue prolapse, and incomplete stent apposition were observed may therefore underestimate the prevalence of these acute effects following stenting. Future improvements in saline delivery may increase the clear viewing time per bolus injection. Additionally, increases in image acquisition rates would permit increased pull back velocities, thereby extending the ability to image longer segments. The image acquisition rate used in this study (four or eight frames a second) is limited only by the power available from the light source of the system. Although there are no standards for maximum exposure of coronary arteries to near infrared light, the power level used in this study was significantly below that acceptable for continuous exposure of the retina.26
Conclusions
Our study shows the feasibility of using intravascular OCT to monitor stent deployment in human coronary arteries. OCT images of stents obtained in vivo provide more detailed structural information than IVUS images. Based on the results of this study, a prospective investigation of the clinical relevance for in-stent restenosis of dissection, prolapse, asymmetrical deployment, and incomplete apposition, as identified by OCT, is merited. However, the clinical value of monitoring stenting is currently a moving target, considering the prospect of reduced restenosis rates by the use of drug eluting stents. The results of this study suggest that the high resolution and contrast of OCT may make it a superior research tool for detecting and quantifying neointimal proliferation in the testing of new treatments for coronary artery disease, especially in the case of the new coated stents.
Acknowledgments
Development of the OCT imaging system was supported by CIMIT, Boston, Massachusetts; catheters for IVUS imaging were provided by Boston Scientific Corporation, Natick, Massachusetts. This research was supported by a grant from The Guidant Corporation, Santa Clara, California, USA.