Article Text

Abstract
Objective: To evaluate left ventricular morphology and function in a large population of patients with β thalassaemia.
Design: Echo Doppler assessment of left ventricular function and correlation of cardiovascular data with haematological data.
Setting: Thalassaemia unit in a tertiary referral centre.
Patients: 197 young adults with β thalassaemia, following an adequate transfusional and chelation treatment regimen, without clinical signs of cardiopulmonary involvement. The control group consisted of 213 healthy subjects.
Results: Left ventricular volumes, mass index, and mass/volume ratio were increased. Diastolic and systolic shapes were different, the left ventricle maintaining an ellipsoidal shape. The ejection fraction was reduced, and was < 50% in 33 patients. Stroke volume and cardiac index were increased, and systemic vascular resistance was decreased. Fractional shortening and mean velocity of circumferential shortening were decreased. Meridional end systolic and peak systolic stress were increased, as was circumferential end systolic stress. The contractile state was reduced while the functional preload index did not differ. Left ventricular diastolic function, evaluated from the mitral inflow, showed a slightly prolonged isovolumic relaxation time, increased flow velocity integrals, and an increased E/A ratio. Among the haematological data, only serum ferritin showed a weak negative correlation with left ventricular ejection fraction. The patients with the highest serum ferritin (> 2500 ng/ml) had the lowest ejection fraction.
Conclusions: Patients with β thalassaemia on an adequate transfusion and chelation treatment regimen show abnormal left ventricular remodelling with increased volumes, mass, and mass/volume ratio. Systolic chamber function and contractile state are reduced, with a slightly increased afterload. These findings seem mainly to be related to the increased cardiac output caused by chronic anaemia. Left ventricular performance is better preserved when chelation treatment is adjusted to maintain the serum ferritin concentration at < 1000 ng/ml.
- thalassaemia major
- left ventricular dysfunction
- Doppler echocardiography
- iron toxicity
- A, peak A wave velocity
- Ci, cardiac index
- DR, deceleration rate
- DT, deceleration time
- E, peak E wave velocity
- EDVi, end diastolic volume index
- ESSc, end systolic circumferential stress
- ESSm, end systolic meridional stress
- ESVi, end systolic volume index
- FPI, functional preload index
- FS, fractional shortening
- FVI, area under the total velocity curve
- FVId, velocity integral of diastolic forward flow
- FVIr, velocity integral of reverse flow
- FVIs, velocity integral of systolic forward flow
- IVRT, isovolumic relaxation time
- Ld/Dd, diastolic long axis/short axis ratio (diastolic shape)
- Ls/Ds, systolic long axis/short axis ratio (systolic shape)
- Mi, mass index
- mVCFc, mean velocity of circumferential shortening corrected for heart rate
- M/V, mass/volume ratio
- PSSc, peak systolic circumferential stress
- PSSm, peak systolic meridional stress
- SSI, stress shortening index
- SVI, stress velocity index
- SVi, stroke volume index
- SVR, systemic vascular resistance
- TFVI, velocity integral of total forward flow diastolic flow
Statistics from Altmetric.com
- A, peak A wave velocity
- Ci, cardiac index
- DR, deceleration rate
- DT, deceleration time
- E, peak E wave velocity
- EDVi, end diastolic volume index
- ESSc, end systolic circumferential stress
- ESSm, end systolic meridional stress
- ESVi, end systolic volume index
- FPI, functional preload index
- FS, fractional shortening
- FVI, area under the total velocity curve
- FVId, velocity integral of diastolic forward flow
- FVIr, velocity integral of reverse flow
- FVIs, velocity integral of systolic forward flow
- IVRT, isovolumic relaxation time
- Ld/Dd, diastolic long axis/short axis ratio (diastolic shape)
- Ls/Ds, systolic long axis/short axis ratio (systolic shape)
- Mi, mass index
- mVCFc, mean velocity of circumferential shortening corrected for heart rate
- M/V, mass/volume ratio
- PSSc, peak systolic circumferential stress
- PSSm, peak systolic meridional stress
- SSI, stress shortening index
- SVI, stress velocity index
- SVi, stroke volume index
- SVR, systemic vascular resistance
- TFVI, velocity integral of total forward flow diastolic flow
Cardiac complications such as heart failure and arrhythmias, caused by the so called “iron induced” cardiomyopathy, are considered to be the primary cause of death in patients with β thalassaemia major.1 Left ventricular systolic and diastolic function in patients with β thalassaemia with varying degrees of cardiac involvement including heart failure has recently been investigated by Doppler echocardiography. However, the findings—mostly concerned with left ventricular diastolic function—are somewhat conflicting.2–4
The present study was carried out in a large population of young adults with β thalassaemia major, who were following a carefully monitored transfusion and chelation therapy regimen, in order to evaluate morphological and functional changes in the left ventricle, and to correlate the echocardiographic findings with the haematological data.
METHODS
Study population
Of the 273 patients followed in the outpatients service of the thalassaemia unit at Ferrara, we enrolled 197 transfusion dependent subjects with β thalassaemia in the study (101 male, 96 female; mean (SD) age, 25.7 (5.9) years, range 9–39 years) (table 1). They were all examined in the period between 1997 and 2000.
Demographic data of patients with β thalassaemia major and normal controls
Inclusion criteria were as follows:
-
all the patients were under regular observation by the same thalassaemia unit
-
at the time of echo Doppler examination none of the patients had clinical signs of cardiac dysfunction or echo Doppler findings of pulmonary hypertension
-
none was taking any cardioactive drugs
-
none presented with major endocrine disorders, such as diabetes, hypoparathyroidism, or hypothyroidism.
Each patient was receiving a red cell transfusion every 2–3 weeks. Iron chelation treatment with desferrioxamine by subcutaneous injection was given 5–6 days a week on the basis of serum ferritin monitoring.
The following clinical and haematological data were obtained: age at diagnosis, duration of follow up, whether or not a splenectomy had been done, haemoglobin concentration (mean pretransfusional value in the previous year), serum ferritin concentration (mean value in the previous year), duration of transfusion treatment and iron chelation therapy, and compliance with treatment (table 2). All the patients had an echo Doppler examination the day before receiving a red cell transfusion.
Haematological profile of the patients with β thalassaemia major
The control group consisted of 213 healthy subjects comparable in age and sex, free from any cardiovascular disorder, not taking any cardioactive drugs, and with a normal echo Doppler examination (table 1).
Echo Doppler examination
The examination included a complete cross sectional echocardiographic imaging and an accurate Doppler examination of all the cardiac chambers to exclude left ventricular wall motion abnormalities and any significant valvar lesions. All echocardiographic measurements—which were done by the same observer (MV)—are reported as the average of at least three cardiac cycles, according to the criteria of the American Society of Echocardiography.5 In our laboratory, intraobserver and interobserver reproducibility of the measurements, based on the analysis of the same sets of cardiac cycles, was 4.2 (3)% and 5.1 (3.2)%, respectively. Peak systolic and diastolic blood pressure was monitored using a vital sign monitor (Dinamap; GE Medical Systems, Salt Lake City, Utah, USA) during the echo Doppler examination.
Analysis of left ventricular volume, shape, and mass
Left ventricular volume indices (EDVi, ESVi) and mass index (Mi) were obtained by measuring the areas from the short axis planes, the long axes from the apical endocardium to the midpoint of the plane of the mitral valve in the apical four chamber view, and using the area–length model.6–8 The ratio of left ventricular end diastolic mass/volume ratio (M/V) was used to evaluate the degree of wall thickness adaptation to chamber size changes. Left ventricular chamber shape was assessed using the long axis/minor axis ratio obtained at end diastole (Ld/Dd) and end systole (Ls/Ds).6,9 The ejection fraction, stroke volume index (SVi), and cardiac index (Ci) were obtained from the left ventricular volumes. Systemic vascular resistance (SVR) was calculated from the ratio [MBP − RAP]/CO, where MBP = mean blood pressure, RAP = right atrial pressure (assumed to be 4 mm Hg), and CO = cardiac output.
Analysis of left ventricular systolic function, afterload, contractility, and preload
From a parasternal short axis cut of the left ventricular end diastolic and end systolic diameters, posterior wall thickness at end diastole and end systole and septal thickness at end diastole were measured to calculate the following:
-
fractional shortening (FS) and mean velocity of circumferential shortening corrected by heart rate (mVCFc)10
-
end systolic meridional (ESSm) and circumferential stress (ESSc) (that is, indices of afterload)11–13
-
peak systolic meridional (PSSm) and circumferential stress (PSSc) (that is, indices of appropriate hypertrophy)14,15
-
stress shortening index (SSI) and stress velocity index (SVI) (that is, indices of the left ventricular contractile state, sensitive and insensitive, respectively, to preload)16,17
-
the functional preload index (FPI = SSI − SVI), which reflects the functional consequences of preload.15–17
Analysis of left ventricular diastolic function
Left ventricular diastolic function was evaluated by pulsed Doppler sampling of the mitral inflow. The peak E (E) and A (A) wave velocities, the E/A ratio, the deceleration time (DT), and the isovolumic relaxation time (IVRT) were obtained. From the Doppler curve, the area under the total velocity curve (FVI), E area (Ea), A area (Aa), and their ratios (Ea/FVI, Aa/FVI, and Ea/Aa) were obtained18; the ratio E/FVI (that is, the index of left ventricular diastolic function not dependent on heart rate and preload) was also obtained.19
Pulmonary venous flow was examined with the sample volume positioned at the orifice of the right upper pulmonary vein. The following Doppler velocities were obtained: peak velocity during ventricular systole (S) and diastole (D); the systole/diastole (S/D) ratio; and the peak reverse flow (R) caused by atrial contraction. In case of biphasic systolic flow, the highest wave is taken as the maximum systolic velocity. Flow velocity integrals of total forward flow (TFVI), systolic flow (FVIs), diastolic flow (FVId), and reverse flow (FVIr) were traced, and their ratios (FVIs/TFVI, FVIs/FVId, FVIr/TFVI) obtained.20
Statistical analysis
Data are presented as mean (SD). A two sample Student t test was used to assess the differences between the variables in patients with β thalassaemia and control subjects. Differences were considered significant at a probability value of p < 0.01. Linear regression analysis was tested between the haematological and echocardiographic findings. A multiple linear regression analysis between the haematological data and ejection fraction of the left ventricular was undertaken.
RESULTS
Clinical findings
Demographic data on the β thalassaemia patients and the healthy controls are summarised in table 1. Weight, height, and body surface area were significantly smaller in the β thalassaemia group. Systolic, diastolic, and mean blood pressures were lower in the β thalassaemia group, while heart rate was slightly increased.
The haematological profile of the β thalassaemia patients is shown in table 2. The mean pretransfusional haemoglobin concentration was 9 (0.5) g/dl, and the average serum ferritin level was 1280 (1271) ng/ml. The great majority of these patients showed good compliance with iron chelation treatment. All patients but one had undergone splenectomy.
Echo Doppler findings
In the β thalassaemia patients, left ventricular volumes, Mi, and the M/V ratio were increased, while diastolic and systolic shapes were different, the left ventricle maintaining an ellipsoidal shape. The ejection fraction of the left ventricle was reduced, and was < 50% in 33 of the thalassaemia patients. SVi and Ci were increased, while the systemic vascular resistance was decreased (table 3). FS% and mVCFc of the left ventricular diameters were decreased. ESSm, PSSm, and ESSc were increased, while PSSc did not differ from the controls. Contractile state was reduced, while the FPI did not differ from the controls (table 4).
Left ventricular volumes, mass, shape, and cardiac index in patients with β thalassaemia major and controls
Left ventricular systolic function, afterload, contractility, and preload in patients with β thalassaemia major and controls
Left ventricular diastolic function, assessed at mitral inflow level, showed an increase in total flow velocity integrals because of an increase in early and late filling integrals, with an increased E/A ratio. DT of the early filling wave did not differ from the controls, while the deceleration rate (DR) was increased. The IVRT was slightly prolonged (table 5). The pulmonary vein Doppler interrogation showed slightly decreased diastolic velocities and integrals, with an increase in the systolic/diastolic ratios (table 6).
Left ventricular diastolic function from mitral valve inflow in patients with β thalassaemia major and controls
Left ventricular diastolic function from pulmonary venous inflow in patients with β thalassaemia major and controls
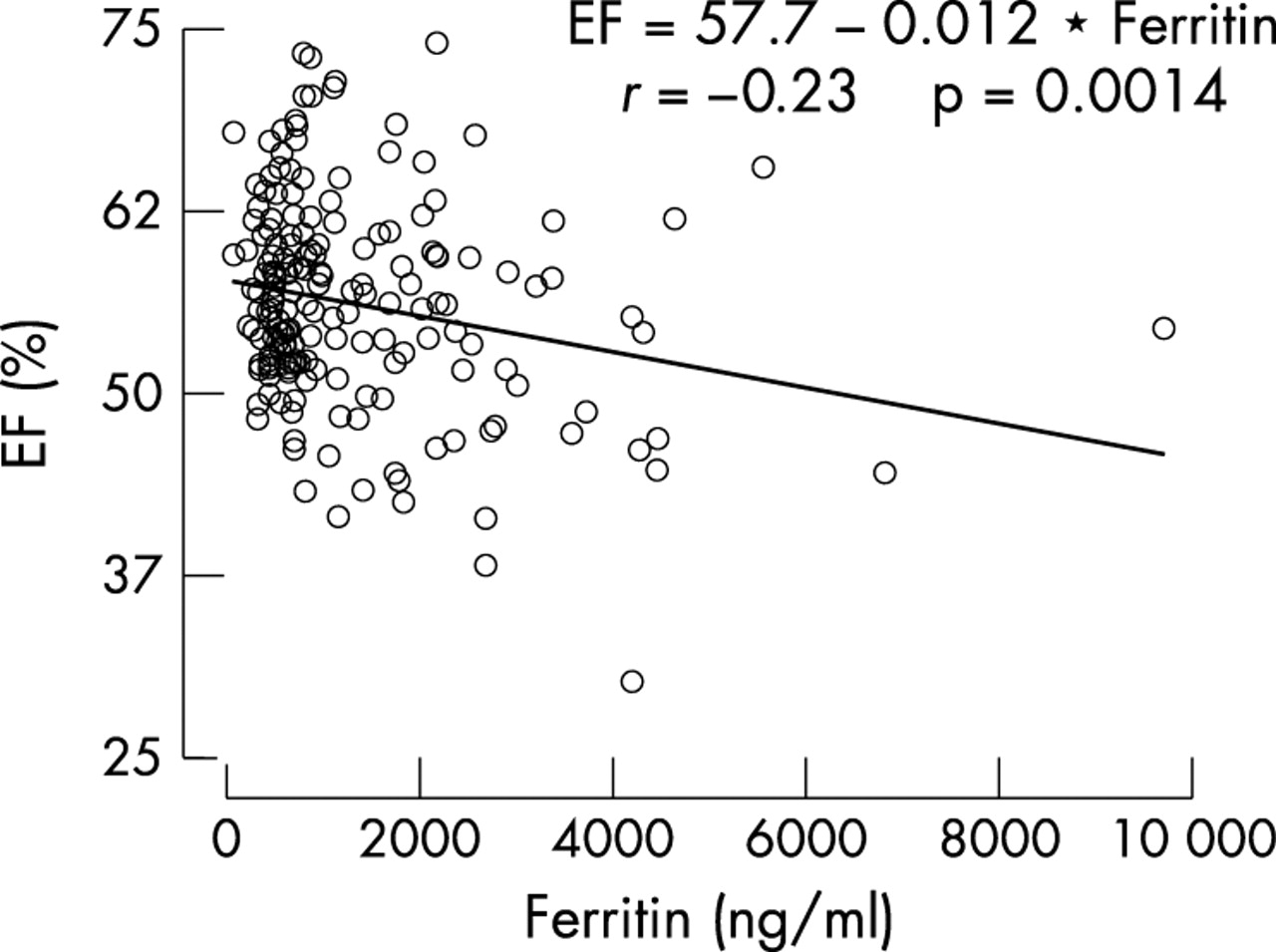
Among all the haematological data considered (table 2), only the serum ferritin concentration showed a weak negative correlation with the left ventricular ejection fraction (r = −0.23; p < 0.001) (fig 1). A weak correlation (r = 0.27; p < 0.05) between the haematological data and ejection fraction was found also on multiple linear regression analysis. The ejection fraction was significantly decreased in the group with the highest ferritin concentration (> 2500 ng/ml) in comparison with the patients with the lowest ferritin concentration (< 1000 ng/ml) (table 7).
Comparison of the left ventricular ejection fraction in patients with serum ferritin concentration < 1000 ng/ml (group 1), 1000–2500 ng/ml (group 2), and > 2500 ng/ml (group 3)

{kind=link}
Correlation between left ventricular ejection fraction (%) and the serum ferritin concentration.
DISCUSSION
This study shows that in young adults with β thalassaemia but no clinical signs of cardiopulmonary involvement, and with a mean pretransfusional haemoglobin concentration of around 9 g/dl, there are abnormalities of left ventricular morphology and systolic and diastolic function. In particular, there is an increase in left ventricular volumes, mass, stroke volume, and cardiac index, with decreased systemic vascular resistance, explaining the decreased systolic and diastolic blood pressure. The increased volume load is a reflection of the Frank–Starling mechanism and an increase in heart rate. All these findings are in agreement with those reported by others and are related to the increased cardiac output caused by the chronic anaemia.3,21 Our study also shows a decrease in left ventricular systolic performance owing to an increase in the afterload and a reduced contractile state, which is probably secondary to iron toxicity.22–24
Waldes-Cruz and colleagues demonstrated abnormalities of left ventricular systolic and diastolic function in asymptomatic children with β thalassaemia, using computer assisted echo studies.22 Borow and colleagues reported an abnormal left ventricular end systolic pressure/dimension relation in asymptomatic young adults with β thalassaemia, showing normal indices of global systolic performance.23 Others have reported early cardiac dysfunction in asymptomatic β thalassaemic patients with chronic iron overload, using stress radionuclide angiography. The stress induced alterations of left ventricular systolic performance showed a correlation with the total amount of blood transfused in these patients. Even in patients with few blood units transfused, an abnormal response of the left ventricular ejection fraction to exercise was found, while the haemoglobin concentration was not predictive of left ventricular performance.24 Moreover, in asymptomatic patients with β thalassaemia submitted to an aggressive iron chelation regimen, a decrease in serum ferritin was associated with an increase in the left ventricular ejection fraction during stress testing.25
In our study, we found a weak but significant correlation between left ventricular ejection fraction and serum ferritin concentration. Patients with a high ferritin concentration (> 2500 ng/ml) had a lower ejection fraction than patients with a low ferritin concentration (< 1000 ng/ml). No other haematological data correlated with the echocardiographic findings.
In 1994 Olivieri and colleagues, in a prospective clinical study,26 found that the cardiovascular prognosis in thalassaemic patients was excellent if serum ferritin concentrations were maintained below 2500 ng/ml. This value has been considered a “safe” concentration.26 Our study confirms this assumption, demonstrating the importance of a low ferritin concentration for the preservation of left ventricular mechanics. The higher mean age of our patients is further confirmation of a significant improvement not purely related to quality of life. This probably reflects a more aggressive treatment and the further lowering of the ferritin concentration in our study population. We suggest that a serum ferritin value of less than 1000 ng/ml should be considered the ideal goal of any therapeutic schedule. The value of starting this therapeutic approach early and maintaining good compliance has been documented before.26,27
Reports concerning left ventricular diastolic function in patients with β thalassaemia are somewhat conflicting.2–4 In 1991, Spirito and colleagues reported a restrictive pattern of transmitral flow in a group of young adults with normal systolic function.2 In contrast, no alteration in left ventricular compliance was reported in the early stage of the disease by Kremastinos and associates.3,4 The filling pattern previously reported was explained by increased volume overload caused by the hyperdynamic state.3,28 A strongly restrictive pattern of transmitral flow was reported only in the final stages of the disease, as in the final stages of dilated cardiomyopathies.2,3,29,30 In agreement with Kremastinos and colleagues,3 we have shown in our group of asymptomatic young thalassaemic adults that there is normal left ventricular compliance, and the increase in velocities and integrals of the mitral and pulmonary venous flow could be explained by the high cardiac output state.
Conclusions
Our study, which involved a large and clinically homogeneous group of patients with β thalassaemia following an aggressive transfusion and iron chelation treatment regimen, confirms the primary role of the high cardiac output state in the pathogenesis of most of the echo Doppler findings in this condition. However, there is no consensus over the optimal haemoglobin concentration required to reduce the volume overload, and consequently the optimum chelation dose for the individual patient. Our study further underlines the importance of reducing body iron stores, as a correlation between serum ferritin and left ventricular mechanics has been confirmed.
Thus several factors are involved in the pathogenesis of the so called “β thalassaemic cardiomyopathy”. The first factor is the significant volume overload imposed by the chronic anaemia,3,4 and this has also recently been demonstrated in patients affected by thalassaemia intermedia.31 More aggressive transfusion treatment could reduce the role of this factor, though it has the disadvantage of a further increase in the iron load. The second factor is iron toxicity, although the mechanisms involved in this are not universally agreed. However, cardiac iron deposits surely represent a late event, and their amount has so far not proved easy to estimate.32 A third factor is the possibility that infectious myopericarditis plays a significant role in the pathogenesis of severe left ventricular dysfunction.33,34 Further studies are required to clarify the role of this complication, as bacteriological and virological studies have revealed no causative factor in the majority of cases reported so far, though immune or genetic mechanisms have recently been proposed.34,35
Acknowledgments
We are indebted to Professor Calogero Vullo for his precise and careful advice during the undertaking of this study. The work was partially supported by a grant of the “Associazione per la Lotta alla Talassemia,” Section of Ferrara, Italy.