Article Text

Abstract
Objective: To investigate the relation between the degree of ST segment resolution (STR) after thrombolysis and the pressure derived collateral flow index (CFIp), determined using an intracoronary pressure measurement technique in patients with recent myocardial infarction.
Methods: 33 patients were studied. TIMI grade III flow was achieved in the infarct related artery by thrombolysis. A surface ECG was obtained on admission and 90 minutes later. The sum of ST segment elevations was measured by summing all leads with ST elevation on the baseline ECG and on the 90 minute ECG (after thrombolysis) and calculating the percentage recovery. The study population was divided into two groups, with good STR (⩾ 50%; group 1) or poor STR (< 50%; group 2). After angiography, a fibreoptic pressure monitoring guidewire was advanced to the stenosis to be dilated. The CFIp was determined as the ratio [coronary wedge pressure − central venous pressure]/[mean aortic pressure − central venous pressure].
Results: The mean STR on the surface ECG was 54.6% and mean (SD) CFIp was 0.25 (0.12) (range 0.10–0.41). There was an inverse correlation between the individually calculated percentage of STR and CFIp (r = −0.64, p < 0.01). The mean CFIp was lower in patients with a good STR than in those with a poor STR (0.18 (0.07) v 0.27 (0.10), p < 0.02).
Conclusions: Although TIMI grade III flow was achieved after thrombolysis, a worse STR on the surface ECG was associated with higher CFIp measured in the infarct related artery. CFIp appears to reflect the degree of microvascular obstruction by quantifying impedance of the microvasculature.
- ST segment resolution
- pressure derived collateral flow index
- acute myocardial infarction
- thrombolysis
- CFIp, pressure derived collateral flow index
- CWP, coronary wedge pressure
- FFRmyo, myocardial fractional flow reserve
- STR, ST segment resolution
- TIMI, thrombolysis in myocardial infarction
- Pa, proximal aortic pressure
- Pd, distal aortic pressure
- Pv, central venous pressure
Statistics from Altmetric.com
- CFIp, pressure derived collateral flow index
- CWP, coronary wedge pressure
- FFRmyo, myocardial fractional flow reserve
- STR, ST segment resolution
- TIMI, thrombolysis in myocardial infarction
- Pa, proximal aortic pressure
- Pd, distal aortic pressure
- Pv, central venous pressure
Resolution of ST segment elevation has been shown to be a simple and useful predictor of final infarct size, left ventricular function, and clinical outcome after both thrombolytic and interventional approaches to the management of acute myocardial infarction.1–3 It is known that a patent epicardial artery does not necessarily result in reperfusion at a cellular level, and it has been suggested that ST segment recovery may be a better marker of myocyte reperfusion.4–6 Determination of a pressure derived collateral flow index (CFIp), assessed by intracoronary pressure measurement with a pressure monitoring guidewire, makes it possible to evaluate collateral function in the non-infarcted heart.78 However, after acute myocardial infarction, CFIp is significantly influenced by the severity of the dysfunction in the ischaemic microvasculature.9
Our objective in this study was to evaluate the correlation between the degree of ST segment resolution (STR) and CFIp in patients with acute myocardial infarction treated with thrombolysis, in whom TIMI (thrombolysis in myocardial infarction) grade III flow was achieved in the infarct related artery after thrombolysis.
METHODS
Study patients
We studied 33 patients between September 1999 and August 2001. They all presented within six hours of symptom onset (typical chest pain lasting more than 30 minutes) with ST segment elevation in at least two contiguous leads. They were treated with tissue plasminogen activator. The angiographic inclusion criteria were as follows:
-
TIMI grade III flow in the infarct related artery
-
single vessel disease
-
all destined for stent implantation.
ECG evaluation
Standard 12 lead ECGs were obtained at baseline and at 90 minutes after admission. All ECGs were evaluated by a single investigator blinded to the angiographic data. The ST segment was measured 20 ms after the J point. The summed ST segment elevation was measured by summing the ST amplitude in all leads with ST elevation at baseline (before fibrinolysis) and at 90 minutes (post-fibrinolysis), using methods described previously by Schröder and colleagues.10 The per cent resolution of STR was calculated as the initial sum of ST segment elevation minus the sum of ST segment elevation on the second ECG, divided by the initial sum of ST segment elevation. STR was also categorised on a dichotomous scheme which defined it as good (⩾ 50%) or poor (< 50%).1112
Angiographic analysis and intracoronary pressure measurements
Cardiac catheterisation was done at a mean of four days after the myocardial infarct. Left and right coronary angiography and left ventriculography were achieved in all patients. TIMI flow grades were assessed as previously described.13 Angiographic collateral grade was determined by two observers using Rentrop’s classification.14 After angiography, a fibreoptic pressure monitoring guide wire (pressure wire, 0.014 inch (0.36 mm), Radi Medical Systems, Sweden) was set at zero, calibrated, advanced through the guiding catheter, and positioned distal to the stenosis to be dilated. The same wire was used as a guidewire for the angioplasty catheter. Proximal aortic (Pa), distal aortic (Pd), and central venous (Pv) pressures were recorded simultaneously. Adenosine was used as the hyperaemic agent, given in intracoronary bolus doses of 20 μg for the left coronary system and 15 μg for the right coronary system, and repeated if necessary. Myocardial fractional flow reserve (FFRmyo) was calculated under adenosine hyperaemia as the ratio of mean Pd minus Pv to mean Pa minus Pv. During the stent implantation procedure, when total occlusion was achieved by balloon occlusion, the distal pressure obtained from the pressure wire was recorded as the coronary wedge pressure (CWP, mm Hg). CFIp (unitless) was calculated as the ratio of simultaneously measured CWP minus Pv to mean Pa minus Pv.
Statistical analysis
Statistical analysis was done using SPSS 10.0 for Windows. Data are expressed as mean (SD). A probability value of p < 0.05 was considered significant. Differences between groups were evaluated by χ2 analysis for categorical variables and by Student’s t test for continuous variables. The Pearson correlation analysis was used to investigate relations between variables.
RESULTS
The baseline clinical and angiographic characteristics of the patients are given in table 1. Most of the patients presented with anterior wall infarction, and the left anterior descending coronary artery was the culprit vessel in 66% of the patients. All the patients had TIMI grade III flow in the infarct related artery on coronary angiography, which was done at a mean of four days after the myocardial infarct.
Baseline angiographic and clinical characteristics
ST segment resolution
The mean (SD) ST segment resolution was 54 (26)%. The study population was divided into two groups according to whether they had good STR (⩾ 50%; group 1) or poor STR (< 50%; group 2). Poor STR was observed in 11 of the 33 patients. There were no differences between the two groups with respect to angiographic or clinical characteristics. Preinfarction angina tended to be more frequent in patients with good STR (27% v 45%) (table 1).
Intracoronary pressure measurement
Basal and hyperaemic mean Pa and Pd before and after stent implantation were not different between the two groups. Mean FFRmyo values before and after stent implantation were also similar (table 2). However, mean CWP (18.2 (9.5) v 28.2 (10.1) mm Hg, p<0.02) and CFIp (0.18 (0.07) v 0.27 (0.10), p < 0.02) were significantly lower in patients with good STR than in those with poor STR (figs 1 and 2).
Intracoronary pressure measurements

Mean coronary wedge pressure (CWP, mm Hg) values in patients with good (⩾ 50%) and poor (< 50%) ST segment resolution (STR).

Mean pressure derived collateral flow index (CFIp) in patients with good and poor STR.
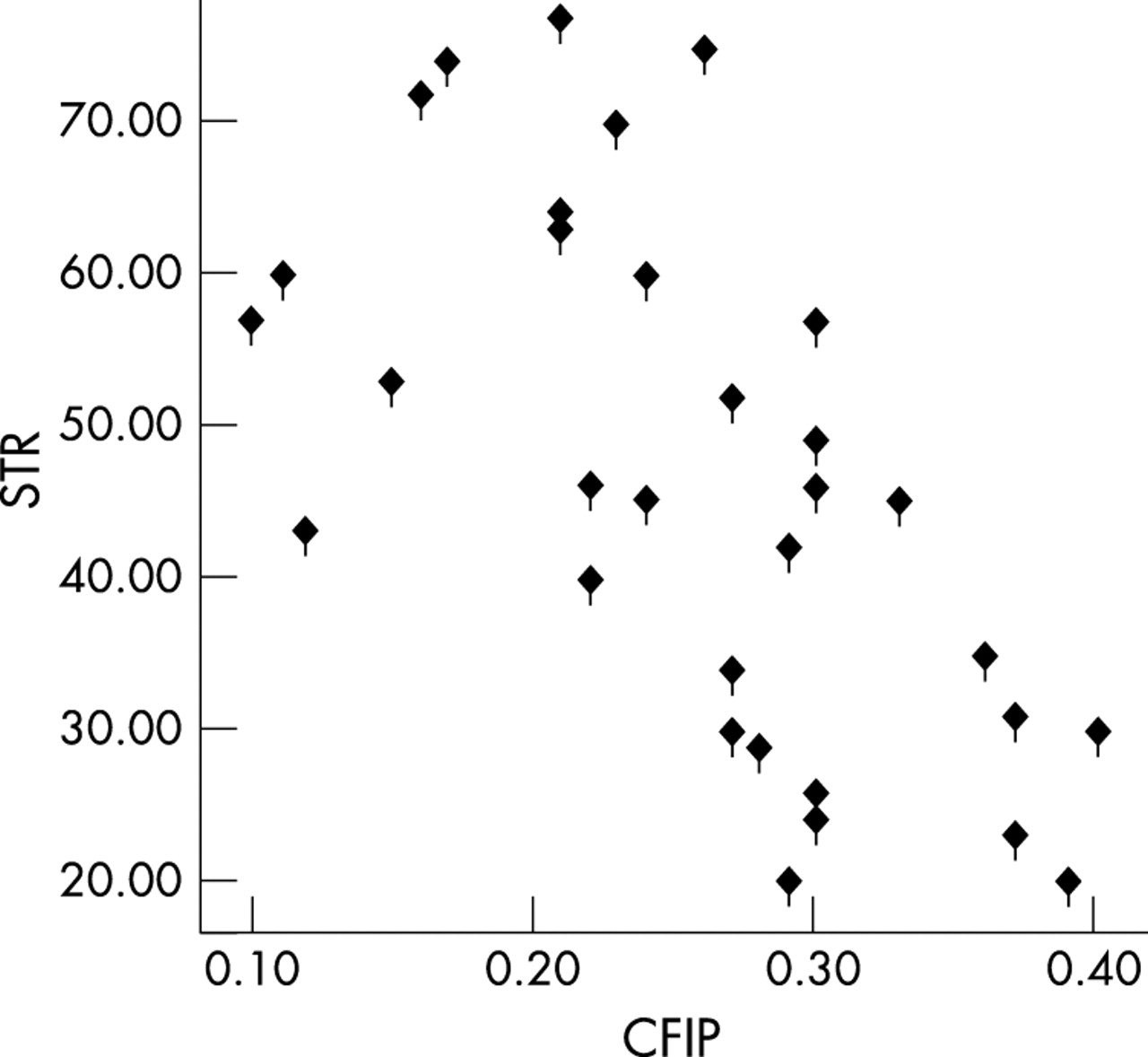
There were also significant inverse correlations between CWP and STR (r = −0.69, p < 0.01) (fig 3) and CFIp and STR (r = −0.64, p < 0.01) (fig 4), implying that higher CFIp and CWP are associated with poorer STR.

Relation between coronary wedge pressure (CWP) and ST segment resolution (STR). There was significant correlation between two variables (r = −0.69, p < 0.01).

There was significant inverse correlation between STR and the pressure derived collateral flow index (CFIp) (r = −0.64, p < 0.01).
Angiographic collateral grade and CFIp and STR
There was no difference in CFIp among the patients with collateral grades 0 to 3 (grade 0: 0.20 (0.09); grade 1: 0.25 (0.12); grade 2: 0.22 (0.11); grade 3: 0.25 (0.08); NS). There was also no relation between CFIp and collateral grade (r = 0.16) (fig 5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Comparison of pressure derived collateral flow index among angiographic collateral grades. There was no correlation between these two variables (r = 0.16).
We found no differences between the two groups with respect to angiographic collateral grades (p = 0.41).
DISCUSSION
To our knowledge, this study represents the first investigation of the correlation between the extent of ST segment resolution and the degree of microvascular destruction determined by intracoronary pressure measurement in patients with reperfused acute myocardial infarction. We found that a greater STR was associated with lower CFIp values.
ST segment resolution as a marker of myocardial tissue perfusion
The primary goal of reperfusion therapy has shifted from opening of the infarct related artery to establishment of myocardial tissue perfusion.1516 It has been reported that STR is a practical and useful measure of this latter variable.111217 Several studies have shown that persistent ST elevation is predictive of poor recovery of left ventricular function and of increased mortality, even among patients with TIMI grade 3 flow after a percutaneous coronary intervention.1819 This finding is supported by results from contrast echocardiography,20 nuclear scintigraphy,21 and Doppler flow wire studies,22 which show that no reflow in the microvasculature is associated with poor recovery of left ventricular function, even when patency has been restored in the infarct related artery. Santoro and colleagues demonstrated a relation between failure of ST resolution and reduced myocardial perfusion assessed by contrast echocardiography.23 In another study it was confirmed that early resolution of ST segment elevation correlated with myocardial salvage as assessed by Tc-99m sestamibi scintigraphy.24 It has been shown that patients with ⩾ 50% STR have improved left ventricular function and reduced mortality.2526 In the present study, 33% of the patients had poor STR (< 50%) after thrombolysis, implying that extensive tissue and microvascular injury had occurred in a substantial number of the patients, although all had TIMI grade 3 flow at the coronary angiography. The pressure derived collateral flow index was found to be raised in this group of patients. We also found that there was a significant inverse correlation between CFIp and STR, implying that a higher CFIp is associated with poorer STR. This finding suggests that CFIp is affected by microvascular dysfunction even in reperfused patients with TIMI grade 3 flow after acute myocardial infarction, and that it reflects the degree of microvascular dysfunction.
Pressure derived collateral flow index as a marker of microvascular obstruction
Several studies have reported that intracoronary pressure measurements with a pressure wire permit the assessment of collateral function in the non-infarcted heart.27–29 The CFIp is hypothesised to increase with an increase in collateral flow. However, in the infarcted heart CFIp is not associated with well developed collateral channels. Yamamuto and colleagues showed that the CFIp does not necessarily reflect collateral function in patients with acute myocardial infarction.9 They observed that the CFIp is influenced by the presence and severity of ischaemic microvascular dysfunction in acute myocardial infarction, and that a higher CFIp is associated with the no reflow phenomenon and with worse functional outcomes. The relation we found between STR and CFIp (a higher CFIp is associated with a poorer STR) is similar to that observed by Yamamuto and colleagues,9 who used myocardial contrast echocardiography as a marker of tissue perfusion. In the normal heart, coronary blood flow fills the intramyocardial blood pool and partially runs through the coronary microvasculature into the venous circulation. Extensive microvascular obstruction in the infarcted region can cause congestion of the intramyocardial blood pool. Because of this obstruction, intramyocardial blood pressure should increase with an increase in myocardial wall stress. Thus an increase in mean CWP and CFIp in patients with reperfused infarct related arteries but poor STR on the surface ECG (group 2) is probably related to a greater degree of obstruction in the microvasculature, and these variables can be taken as a marker of the impedance of the distal microvasculature. The inverse correlations found between mean CFIp and STR suggest that a higher CFIp is associated with further destruction in the microcirculation. We did not find any relation between the degree of angiographic collateralisation and CFIp. Thus these variables do not necessarily reflect collateral function in the presence of microvascular dysfunction, which may occur even in patients with acute myocardial infarction and TIMI grade 3 flow. In this study we also showed that although TIMI grade 3 flow was restored after thrombolysis, a sizeable proportion of the patients (33%) probably had abnormal perfusion at the cellular level, as evidenced by a poor STR on the surface ECG. This finding is supported by our measurements of CFIp, a marker of microvascular dysfunction.
Study limitations
Our findings were derived from a selected population of patients with acute myocardial infarction who were treated with thrombolysis and in whom TIMI grade III flow was restored in the infarct related artery. Thus our results cannot be generalised to all patients receiving reperfusion therapy. Second, our study population was relatively small and a larger number of patients may be necessary to confirm our results.
Conclusions
The results support the hypothesis that ST resolution is a surrogate marker of tissue level reperfusion. This study provides further clarification of the relation between STR after thrombolysis and microvascular function, using the CFIp as another measure of microvascular dysfunction.
Acknowledgments
Part of this study was presented as an oral contribution at the 75th AHA Scientific Congress, Chicago, USA, and was published in abstract form in
.