Article Text

Abstract
Objective: To determine the diagnostic potential of a hand carried cardiac ultrasound (HCU) device (OptiGo, Philips Medical Systems) in a cardiology outpatient clinic and to compare the HCU diagnosis with the clinical diagnosis and diagnosis with a full featured standard echocardiography (SE) system.
Methods: 300 consecutive patients took part in the study. The HCU examination was performed by an experienced echocardiographer before patients visited the cardiologist. The echocardiographer noted whether the HCU device was able to confirm or reject the referral diagnosis, which abnormality was detected, and whether SE investigation was necessary. Physical examination by a cardiologist followed and thereafter, whenever required, a complete study with an SE was carried out. The HCU data were compared with the clinical diagnosis of the cardiologist and the SE diagnosis in a blinded manner.
Results: The cardiologist referred 203 of 300 patients for an SE study and 13 patients for transoesophageal echocardiography. In 84 patients no further examination was considered necessary. HCU echocardiography was able to confirm or reject the suspected clinical diagnosis in 159 of 203 (78%) patients. In 44 of 203 (22%) patients SE Doppler was needed. Agreement between the HCU device and the SE system for the detection of major abnormalities was excellent (98%). The HCU device missed 4% of the major findings. Among the 84 patients not referred for an SE, the HCU device detected unsuspected major abnormalities missed with the physical examination in 14 (17%).
Conclusion: Integration of an HCU device with the physical examination augments the yield of information.
- HCU, hand carried cardiac ultrasound
- LV, left ventricular
- SE, standard echocardiography
- diagnosis
- echocardiography
- portable ultrasound device
- hand carried cardiac ultrasound
- heart diseases
- outpatients
Statistics from Altmetric.com
- diagnosis
- echocardiography
- portable ultrasound device
- hand carried cardiac ultrasound
- heart diseases
- outpatients
The physical examination is the cornerstone of the evaluation of patients referred to the outpatient cardiology clinic, but often fails to provide a conclusive diagnosis. Since the introduction of echocardiography and Doppler, the limitations of the physical examination of specific cardiac abnormalities especially in their early stage have been shown.1 In addition, the auscultation skills and experience of cardiologists have declined due to less training in the curriculum as a result of the existing time pressure and the increasing availability and reliance on more sophisticated imaging methods.2–5 Consequently, echocardiography and Doppler are the initial diagnostic tests ordered for most of the patients. In practice, most of these tests are performed several days after the first patient–physician encounter, leading to a delay in the final diagnosis and sometimes treatment.
Recently, small hand carried cardiac ultrasound (HCU) devices have become available and initial studies have shown their validity in the immediate diagnosis of cardiac abnormalities at the point of care.6,7,8,9,10 HCU examination may differentiate normal from abnormal conditions and recognise patients with significant cardiac abnormalities that can be missed by physical examination alone.
The aim of the present study was to determine the diagnostic potential of an HCU device in patients referred for an initial visit to the outpatient cardiology clinic (new patients). The HCU diagnosis was compared with the diagnoses of the cardiologist’s physical examination and of a full featured standard echocardiography (SE) examination.
MATERIALS AND METHODS
Study population and design
During a five month period, 300 new patients referred to the outpatient clinic of the Thoraxcentre, Rotterdam, were examined with an HCU device by an experienced echocardiographer (cardiologist) before the patient’s initial visit to the cardiologist. Table 1 lists the patients’ characteristics. The echocardiographer had the referral diagnosis for which the patient was sent to the cardiologist. She took a brief history, performed the HCU examination (maximum duration 10 minutes), and noted her findings together with a qualitative assessment and quantitative results. She then noted whether further echocardiography and Doppler examination with SE was needed. Subsequently, the patient was examined by the consulting cardiologist, who was unaware of the HCU evaluation and who decided whether an echocardiographic examination with an SE system (Sonos 5500, Philips Medical Systems, Eindhoven, the Netherlands; or System Five, Vingmed, Horten, Norway) was indicated. This examination was then performed by an independent echocardiographer (sonographer) who was blinded to the HCU results. A cardiologist not involved in the study interpreted the SE examination results. All patients had an ECG recorded as a routine clinical practice. The clinical diagnosis made by the physician was based on the combination of clinical history, physical examination, and ECG findings. The institutional medical ethics committee approved the study and informed consent was obtained from all patients.
Baseline characteristics of 300 new patients referred to the outpatient cardiology clinic
The HCU device
The OptiGo (Philips Medical Systems) HCU device was used (fig 1). It is equipped with a 2.5 MHz phased array broadband transducer and operates on a rechargeable lithium ion battery or alternating current. Two dimensional imaging, colour flow Doppler imaging, and two callipers for linear measurements are also integrated with the system. Images are documented on a CompactFlash card.

The OptiGo device, the hand carried cardiac ultrasound (HCU) device used in the study.
Echocardiographic diagnosis with the HCU device
Cardiovascular abnormalities were classified as major or minor. Major abnormalities were considered to be the clinically significant abnormalities that would trigger further diagnostic evaluation, to change or initiate treatment management, or to have prognostic significance (table 2). Minor abnormalities were considered to be abnormalities that were of no clinical significance and would therefore not affect decision making for patient management.
Major cardiovascular findings
Valve or flow abnormalities detected with the HCU device were evaluated with the pulsed and continuous wave Doppler modalities of the SE. The severity of these abnormalities was graded according to standard methods.11
Unsuspected major abnormalities (see table 2 for definition of “major”) were considered to be the echocardiographically detected major abnormalities that were not reported in the history or were not suspected or previously described from the symptoms of the patient. Furthermore, the cardiologist’s physical examination missed these abnormalities.
Statistical analysis
Descriptive statistics are reported as mean (SD) for continuous variables and as percentages for categorical variables. The agreement between the two examination techniques for the detection of major abnormalities was assessed from 2 × 2 tables with weighted κ statistics. On the basis of Fleiss’s classification, κ values < 0.4, between 0.4 and 0.75, and > 0.75 were considered to indicate poor, fair to good, and excellent agreement, respectively.12
RESULTS
General results
Table 3 presents the most common referral question or suspected diagnosis for the 300 patients sent by the primary care physician to the cardiology outpatient clinic. The cardiologist requested after his physical examination an echocardiographic examination for 203 of the 300 (68%) patients. Table 3 also lists the most common referral question or suspected clinical diagnosis for which the SE was requested in these 203 patients. Thirteen of 300 (4%) patients were sent for a transoesophageal study for the evaluation of a cardiac source of embolism. No further examination was considered necessary for 84 of the 300 (28%) patients.
Reasons for referral by primary care physicians and cardiologists
Patients sent for an SE by the cardiologist
The HCU examination was able to confirm or reject the clinical diagnosis of the cardiologist in 159 of the 203 (78%) patients. For example, a suspected clinical diagnosis of left ventricular (LV) hypertrophy can be easily and reliably confirmed or rejected with an HCU examination without the need for SE.8
In 44 of 203 (22%) patients the HCU device was able to confirm or reject the clinical diagnosis, but haemodynamic Doppler assessment was regarded as necessary. Since this feature was not available on the HCU an SE examination followed for the evaluation of the following findings: severity of valve stenosis (14 patients); valvar regurgitant lesion (10 patients); diastolic LV function (four patients); LV outflow tract obstruction (seven patients); congenital abnormality (six patients); and prosthetic valve evaluation (three patients). Of note, in all of these patients the valvar or congenital lesion was detected and a gross estimation of their severity was possible with the HCU device.
Patients not sent for SE by the cardiologist
The cardiologist did not refer 84 of 300 (28%) patients for an SE study. In 17% (14 of 84) of these patients, a major unsuspected abnormality missed by the physical examination was detected with the HCU device. Furthermore, the HCU device detected no abnormalities in 17% (14 of 84) and minor abnormalities in 66% (56 of 84).
The HCU echocardiographer noted that an SE examination would be necessary for 14% (12 of 84) of this group of patients because the Doppler modality was needed (three patients were from the group with unsuspected major abnormalities).
Major and minor abnormalities detected with the HCU device and the SE system
In total 217 patients had an SE examination. The cardiologist referred 203 patients and the HCU examiner independently referred 14 patients.
The agreement between the two devices for the detection of major abnormalities was excellent (98%, κ = 0.95) (table 4). Table 5 lists the abnormalities detected by the SE system and missed by the HCU device and the physical examination. The HCU device missed six major abnormalities: a small ventricular septal defect that was located high, two aortic stenosis (one moderate with a peak gradient of 40 mm Hg and one mild with a peak gradient of 25 mm Hg), a moderate mitral and aortic regurgitation, both in the same patient with a poor echo window, and a moderate LV dysfunction.
Agreement of detection of major abnormalities in 217 patients between the OptiGo and a standard echocardiography system
Comparison between the SE system and the HCU device in the detection of minor and major cardiovascular findings in 203 patients sent for an SE examination
Figure 2 gives a simple overview of the correlation of major and minor findings between the HCU device and the SE system.

Agreement between the hand carried cardiac ultrasound (HCU) device and standard echocardiography (SE) system was 98% (κ = 0.95). HCU found unexpected major abnormalities in 14 of 84 (17%) patients. *Absolute number of patients with abnormalities; †findings from the transoesophageal echocardiography (TOE) examination; ‡of the 84 patients not referred for echocardiography by the cardiologist, 14 with major abnormalities on the HCU underwent SE examination after it was requested by the HCU echocardiographer.
Unsuspected major findings
In total, 71 unsuspected major findings were detected echocardiographically in 61 of 300 patients (20%). Importantly, of these 71 findings 15 were present in 14 of the 84 (17%) patients not referred to SE by the cardiologist. In particular, these findings were LV hypertrophy (six patients), hypertrophic obstructive cardiomyopathy (one patient), LV dysfunction or wall motion abnormalities (three patients), valvar regurgitation (two patients), dilated ascending aorta (one patient), mitral valve prolapse (one patients), and pericardial effusion (one patient). Two of these findings were detected in the same patient. Three patients needed SE Doppler examination for gradient evaluation after the HCU examination. Physical examination misdiagnosed hypertrophic obstructive cardiomyopathy as aortic stenosis in one patient.
The 71 unsuspected major findings were the following: LV hypertrophy (28 patients), valvar regurgitation (20 patients), valvar stenosis (six patients), LV dysfunction (five patients), hypertrophic cardiomyopathy (four patients), and miscellaneous (eight patients).
Figures 3, 4, and 5 present examples of major unsuspected findings detected with the HCU device and verified with the SE system.
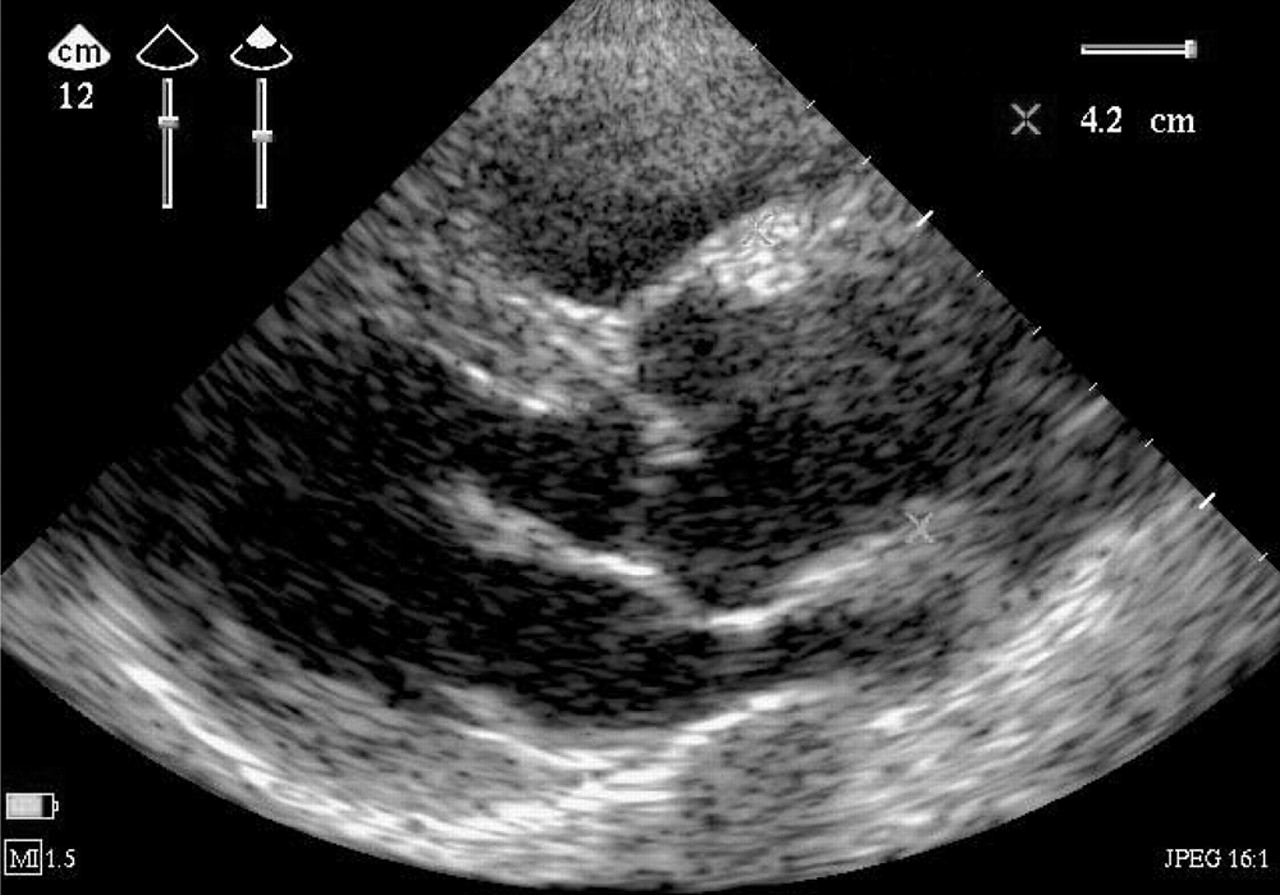
Parasternal long axis view of a 48 year old patient with a dilated ascending aorta (42 mm). The patient had a history of palpitations and was referred to the outpatient cardiology clinic for evaluation of atrioventricular nodal re-entry tachycardias.
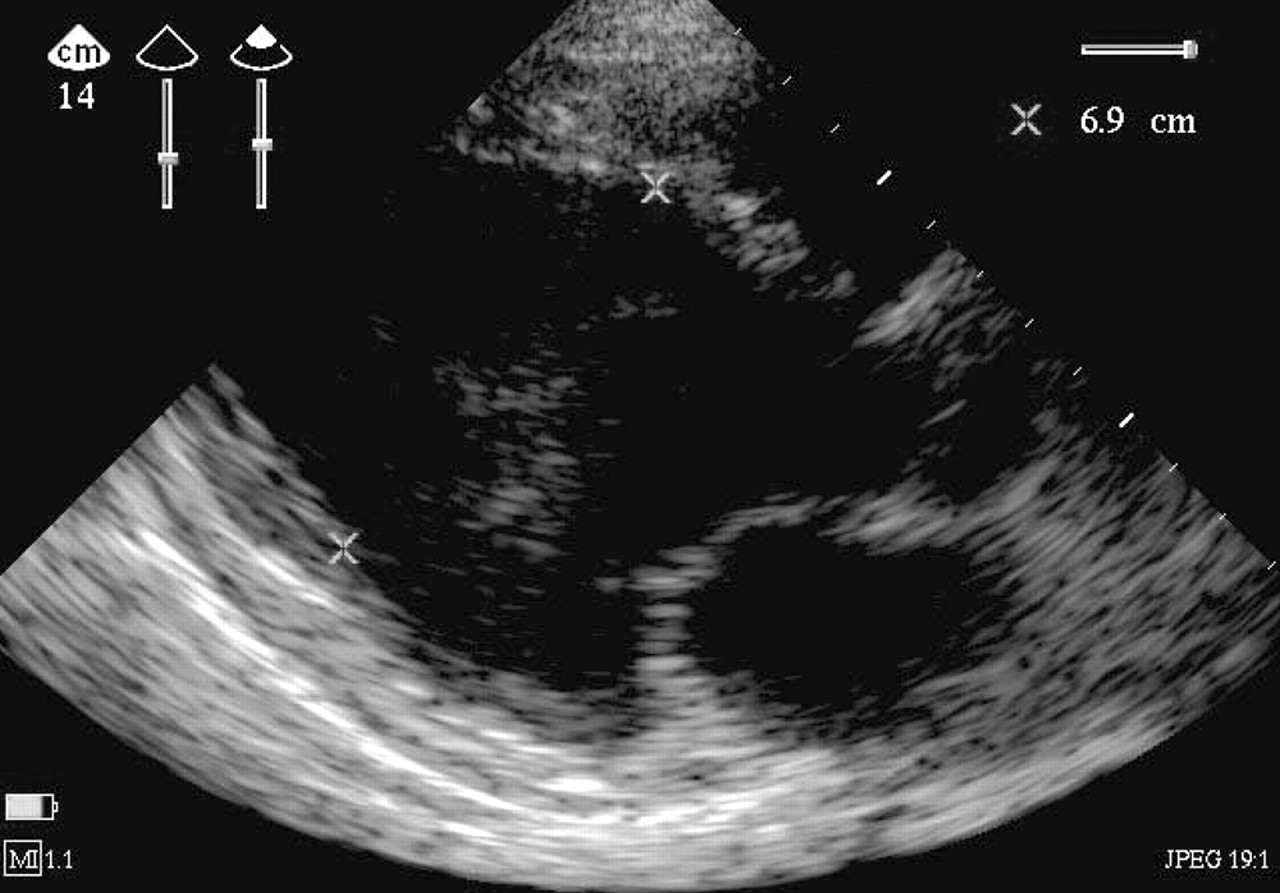
Parasternal long axis view of a 46 year old woman with a history of cancer. She was referred for preoperative evaluation. Left ventricular end diastolic dimension is 69 mm. Ejection fraction was visually estimated to be < 35%. The patient has dilated cardiomyopathy.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Apical four chamber view of a 45 year old patient with (A) prolapse of the posterior mitral leaflet and (B) an eccentric jet towards the interatrial septum. The patient was referred for evaluation of palpitations and was known to have a systolic murmur.
DISCUSSION
The first HCU device to augment the physical examination was introduced by Roelandt and colleagues in Rotterdam in 1978.13–15 However, the combination of the poor image quality, technical limitations, and reimbursement issues discontinued its development. Today, advances in microprocessor technology have led to a new generation of portable echocardiographic systems with excellent image quality and significantly lower cost than SE machines. Several studies have shown their efficacy and accuracy for the diagnosis of major abnormalities at the point of care.6,10,16
In the current study in 78% of patients sent for a full featured SE examination by the cardiologist, the HCU device provided instant information potentially sufficient to avoid an SE examination. Compared with the SE system, the HCU device had a positive predictive value in diagnosing the major abnormalities of 100% and a negative predictive value of 96%. Furthermore, an unsuspected major abnormality was found in 23% of these patients with both the HCU device and the SE system. These abnormalities were not expected based on the history and the patient’s symptoms and were on top of the clinical referral diagnosis made by the cardiologist. The HCU device missed 4% of the major findings. However, it is obvious that knowing the results of the physical examination and the detailed clinical history beforehand would have led to a more focused echocardiographic examination for major findings with high probability and would have reduced the number of missed findings by the HCU device.
Most important, in 84 of 300 (28%) patients the cardiologist considered his physical examination sufficiently accurate to decide that echocardiographic assessment was unnecessary. However, in 17% of these patients unsuspected major abnormalities were found with the HCU device and missed by the physical examination. This is in concordance with the study of Fedson and colleagues.17 It is obvious that direct visualisation leads to a more accurate diagnosis than indirect observation by palpation and auscultation even by the best experts. “Seeing” enables the pre-symptomatic detection of abnormalities and of abnormalities that are beyond physical signs. It is generally recognised that physical examination has shortcomings and that the clinical diagnosis of many common cardiac conditions such as pericardial effusion, early LV dysfunction, hypertrophic cardiomyopathy, or silent valvar disease can challenge the most experienced clinicians, whereas they are readily diagnosed by echocardiography and Doppler examination.1,18 The incorporation of HCU into the physical examination can undoubtedly provide physicians with instant valuable information assisting them in clinical diagnosis and patient management. In the current study the HCU device was tested in an outpatient cardiology clinic. The HCU device has been studied in various clinical settings.6,10,19,20
Patients referred to our outpatient clinic, which is a tertiary referral centre, have a high prevalence of cardiac disease, which explains the high number of requests for an echocardiographic examination. However, since outpatient echocardiographic examinations are often performed several days after the patient’s first visit, the patient must return to the hospital for the examination. With the incorporation of HCU into the physical examination, this extra visit to the hospital could have been avoided by 78% of our study cohort for whom the cardiologist requested an SE examination. But even for the institutions where an SE examination is standard procedure after the physical examination, the integration of HCU with the physical examination can lead to significant cost and time savings, since the majority of referred patients have no abnormalities.
Our study is in concordance with the study of Spencer and colleagues,21 who compared HCU echocardiography at the point of care with the physical examination in a smaller patient cohort (36 patients). They reported that the use of this device by cardiologists reduced the number of major cardiovascular findings missed by the clinical examination. Minor abnormalities were more easily missed. This is in agreement with our findings that the HCU device detected mild valvar regurgitations in only 112 of 150 patients. Furthermore, Galasko and colleagues19 studied 562 patients in a community setting with the same HCU device and correctly identified major abnormalities (LV dysfunction, LV hypertrophy, and left sided valvar regurgitation). They also concluded that minor disease is more likely to be missed.
Spectral flow Doppler is available on some of the HCU devices. Such devices have been shown to overcome limitations in evaluating haemodynamic variables22 and may limit referral for the full featured SE system even further. But still this needs to be evaluated in further studies.
Training requirements
There is no doubt that training is required to use an imaging device. The current study was performed by a cardiologist with expertise in both echocardiography and HCU devices (ECV). Training of clinicians and non-echocardiographers should focus on the criteria of identifying a normal heart and diagnosing major and acute cardiac disorders. The American Society of Cardiology23 has recently published guidelines regarding the use of such devices, recommending level I training as an absolute minimum.24 However, recent studies have suggested that it is possible to train physicians and students to detect significant structural or flow abnormalities in a short period of time with high efficacy.25–29
Physical examination remains the cornerstone of cardiovascular assessment and its use should be encouraged. However, visualising the heart at the point of care helps us to differentiate normal from abnormal conditions and thus to reduce the number of normal referrals, leading to targeted referrals for further diagnostic assessment whenever regarded as necessary. The HCU device should be used as phonocardiography was used in the past: whenever documentation was needed after auscultation. Thus, in case of doubt or whenever haemodynamic and quantitative information is crucial for further management, an examination with a full featured SE system should follow the HCU examination. The appropriate training of clinicians to use such devices is the basic element needed for the future use of the HCU device in daily clinical practice and efforts should be made in this respect.
It should be remembered that the real value of any imaging technology is intimately dependent on our intellectual contribution and individual responsibility.
Limitations
The HCU device that was used for this study had no spectral Doppler modality to obtain haemodynamic data. The valvar abnormalities were evaluated qualitatively with the two dimensional and colour flow Doppler features. However, continuous wave and pulsed wave Doppler echocardiography is necessary for an accurate assessment of valvar regurgitation or stenosis. Furthermore, examination of transmitral flow gives information about the diastolic function and filling pressures. Since this was a blind study, the cardiologist was not aware of which patients had undergone an HCU examination. This was done to avoid any bias that would lead the cardiologist to change his potential request for an SE. Therefore, not all patients had an SE examination, but only when the cardiologist requested it. However, many studies have already proved the accuracy and reliability of the HCU device compared with the SE system in detecting cardiovascular abnormalities. Furthermore, the main interest is to compare the yield of the physical examination with versus without an HCU device.
Conclusion
In patients who attend the outpatient cardiology clinic, integration of an HCU device with the physical examination allows the immediate detection of structural cardiac disease. Often a definitive diagnosis is made or the patient is referred for specific diagnostic tests. A major advantage is that patients with no cardiac abnormality can avoid further echocardiographic tests (negative predictive value is 96%). It appears that the yield of the physical examination is augmented, which alone may miss significant abnormalities.