Article Text

Abstract
Objective: To test the hypothesis that impaired coronary and myocardial blood flow are linked with increased myocyte apoptosis, thus establishing a link between pressure overload and left ventricular (LV) remodelling.
Methods and results: Peak diastolic coronary blood flow velocity (CBFV) was evaluated at transthoracic Doppler echocardiography, and signal intensity (SI) and the rate of SI rise (β) were measured at myocardial contrast echocardiography in 11 patients with severe aortic stenosis and LV hypertrophy. In the same patients, biopsies were obtained from the anterolateral LV free wall during surgery and analysed for cardiomyocyte apoptosis. LV mass corrected CBFV (CBFVI) was significantly lower in patients than in controls (median 0.100 cm·g/s (interquartile range 0.07–0.115) v 0.130 cm·g/s (0.130–0.160), p = 0.002). Similarly, SI*β was significantly lower in patients than in controls (11 1/s (8–66) v 83 1/s (73–95), p = 0.001). Apoptotic rate was increased in aortic stenosis more than 100-fold versus controls (1.2% (0.8–1.4) v 0.01% (0.01–0.01), p < 0.001) and inversely correlated with lower CBFVI and SI*β (r = −0.77, p = 0.001 for both).
Conclusions: Patients with severe aortic stenosis and LV hypertrophy have impaired myocardial perfusion, which is associated with enhanced cardiomyocyte apoptosis. Impaired myocardial perfusion and the ensuing oxygen demand–supply imbalance may, at least partially, be responsible for increased apoptosis and possible transition to heart failure, thus establishing a link between pressure overload, LV remodelling, and heart failure.
- CBFV, coronary blood flow velocity
- CBFVI, coronary blood flow velocity index
- LAD, left anterior descending coronary artery
- LV, left ventricular
- MCE, myocardial contrast echocardiography
- SI, signal intensity
- TUNEL, terminal deoxynucleotidyl transferase mediated dUTP nick end labelling
- aortic stenosis
- apoptosis
- coronary flow reserve
- myocardial contrast echocardiography
- myocardial flow
Statistics from Altmetric.com
- CBFV, coronary blood flow velocity
- CBFVI, coronary blood flow velocity index
- LAD, left anterior descending coronary artery
- LV, left ventricular
- MCE, myocardial contrast echocardiography
- SI, signal intensity
- TUNEL, terminal deoxynucleotidyl transferase mediated dUTP nick end labelling
The natural history of aortic stenosis entails pressure overload and left ventricular (LV) hypertrophy with initially preserved ejection fraction. Without valve replacement, these patients develop diastolic and systolic dysfunction and heart failure,1 with high mortality of untreated patients.2 When ventricular dilatation becomes detectable, pathological alterations such as reduced coronary blood flow per mass of myocardium have already occurred.3 Myocyte loss caused by apoptosis has been reported in both human and experimental heart disease including aortic valvopathy,4–6 hypertensive heart disease,7,8 and post-infarction remodelling.9,10 A major role for apoptosis in the transition from compensated hypertrophy to failure in pressure overloaded hearts has been proposed.6–8 However, the causes of increased apoptosis in aortic valve disease have not been completely characterised. Aortic valve stenosis, ensuing pressure overload, and abnormal coronary and myocardial flow may mechanistically explain increased apoptosis (caused by oxygen demand–supply imbalance) leading to unfavourable remodelling. Thus, the goal of the current study was to measure myocardial perfusion in patients undergoing isolated aortic valve replacement for pure severe stenosis and LV concentric hypertrophy and to ascertain its relation to apoptosis in the same patients by tissue sampling at the time of surgery.
METHODS
Patient selection and sample harvesting
Eleven patients (mean age 70 years; two men) scheduled for elective surgery with symptomatic severe aortic stenosis (valve area ⩽ 0.5 cm2/m2), LV hypertrophy (end diastolic wall thickness ⩾ 12 mm), and preserved LV ejection fraction (> 50%) and without coexisting aortic insufficiency, moderate to severe valvopathy at any other position, presence of coronary artery disease (at angiography), past diagnosis of any type of cardiomyopathy, atrial fibrillation or ventricular pacing, or systemic inflammatory disease and advanced cancer were selected. Two control groups were also selected. A group of five non-hypertensive non-diabetic patients (mean age 60 years; two men) selected among ambulatory patients referred to our institution for atypical chest pain and in whom heart disease was excluded by non-invasive or invasive tests comprised the control group for echocardiography. One group for pathological examination comprised five patients who died of non-cardiac causes (< 30 hours before necropsy) and without a history and pathological findings of heart disease. Selected hearts did not have any alteration of the microarchitecture or autocytolysis of the cardiomyocytes.
Echocardiography
Patients’ data were prospectively recorded. Echocardiography was performed by the same operator the day before intervention. The echocardiographic report was formulated according to the American Society of Echocardiography guidelines.11 All dimensions were indexed to body surface area.
Each patient underwent ultrasound recordings of coronary artery blood flow velocity (CBFV) in the left anterior descending coronary artery (LAD) under baseline conditions. The mid distal LAD was imaged from a modified foreshortened two chamber view with a 7 MHz probe (Sequoia; Siemens). Peak diastolic LAD flow velocity was measured by pulsed Doppler during at least three cardiac cycles (fig 1). CBFV was measured at rest and after infusion of adenosine (140 μg/kg/min intravenously for 90 seconds) and LV mass corrected CBFV (CBFVI) was obtained. Coronary flow velocity reserve was calculated as the ratio of peak velocity after adenosine challenge to baseline velocity.12

Example of (A) distal left anterior descending coronary artery (LAD) visualised by colour Doppler by transthoracic echocardiography and of (B) pulsed wave Doppler flow of the distal LAD.
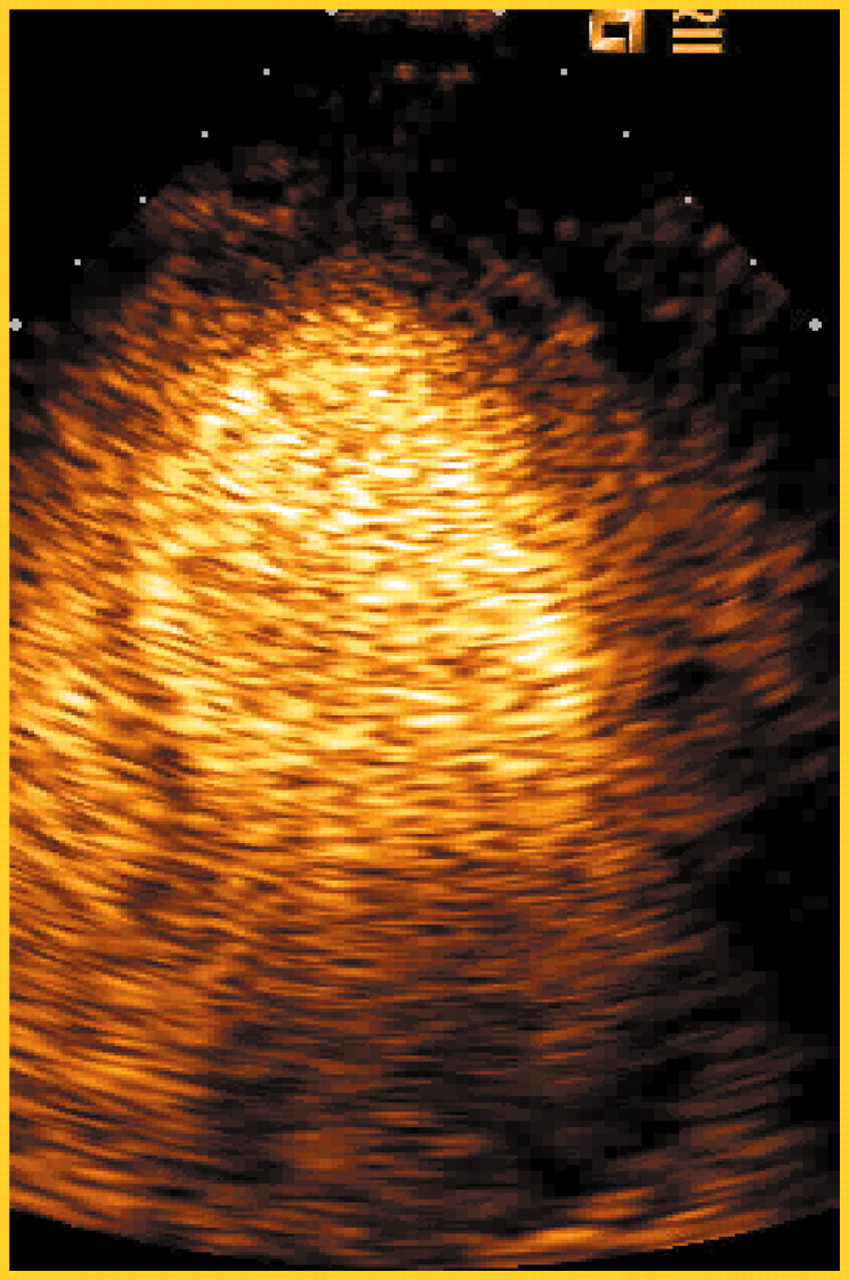
Myocardial contrast echocardiography (MCE) was performed with real time contrast pulse sequencing (Sequoia; Siemens), with intravenous infusion of the second generation ultrasound contrast agent SonoVue (Bracco, Milan, Italy) at the rate of 1 ml/min. Contrast images were acquired in the apical four chamber view optimised to effectively visualise the anterolateral wall, the same wall from where the biopsy was obtained in the operating room (fig 2). As soon as the myocardial video intensity had reached a plateau, a flash of ultrasound with a very high mechanical index was given to destroy microbubbles in the sector. Then the replenishment of bubbles was observed and digitally acquired and stored on to a magneto-optical disk. Then, with custom designed software (Qontrast; AMID, Rome, Italy), a region of interest was positioned in the lateral wall, a replenishment curve was constructed, and peak signal intensity (SI) and SI multiplied by the rate of signal rise (SI*β), which is the best approximation of myocardial flow values, were calculated.13

Example of myocardial contrast echocardiography in the four chamber view.
Surgical procedure
Informed consent was obtained from all patients. All procedures were performed by the same surgical team in a standardised fashion by a median sternotomy approach. A myocardial biopsy was harvested at the epicardial surface from the anterolateral LV free wall before institution of total cardiopulmonary bypass.
Sample processing
Myocardial samples were processed and analysed as extensively described elsewhere.9 Briefly, after the samples were fixed in 10% paraformaldehyde in 0.1M buffer, sections were processed by dehydration, embedding in paraffin, and stained for in situ end labelling of DNA fragmentation (terminal deoxynucleotidyl transferase mediated dUTP nick end labelling (TUNEL)) with an Apoptag kit (Oncor, Gaithersburg, Maryland, USA) (fig 3). Sections were subsequently stained also with antibodies to muscle actin (mouse monoclonal anti-human actin HHF35; DAKO) and activated caspase-3 (cleaved caspase-3 (Asp 175) antibody; Cell Signaling Technology, Beverly, Massachusetts, USA). Suitable negative and positive controls were set up, as defined elsewhere.9 Apoptotic rate was defined as the rate of double positive (TUNEL and caspase-3) cardiomyocytes per field.
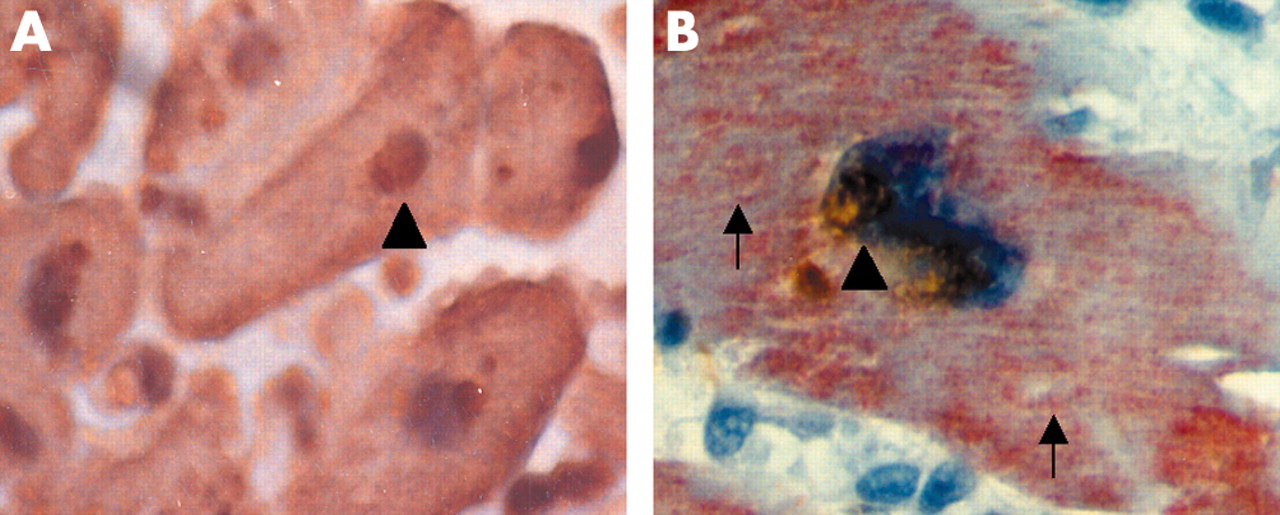
Histological analysis of surgical biopsies of the left ventricular anterolateral free wall. (A) Cardiomyocyte undergoing apoptosis (arrow head), as shown by the dark brown nuclear staining of the terminal deoxynucleotidyl transferase mediated dUTP nick end labelling (TUNEL) reaction, which highlights DNA fragmentation, non-apoptotic nuclei appear blue caused by haematoxylin counterstaining. (B) Colocalisation of TUNEL (arrow head) and red cytoplasmic staining for activated caspase-3 (arrows).
Statistical analysis
Data were statistically analysed with SPSS 10.1 for Windows (SPSS Inc, Chicago, Illinois, USA). Quantitative results are expressed as median (interquartile range) because of potential deviations from assumed normality. The χ2 and Fisher’s tests were used for categorical variables when appropriate. Continuous variables were analysed with Mann-Whitney or Pearson correlation tests. Two tailed significance was at the 0.05 level.
RESULTS
Clinical and echocardiographic characteristics
Table 1 reports characteristics of patients and echocardiographic controls. All patients were in New York Heart Association class II–III. Five patients with refractory hypertension were treated with angiotensin converting enzyme inhibitors and three also with β blockers. All of them had concentric hypertrophy (median LV mass 286 mg and LV mass index 163 mg/m2), and all had normal LV end diastolic and end systolic volumes (table 1).
Clinical and echocardiographic characteristics
Coronary and microvascular flow and flow reserve
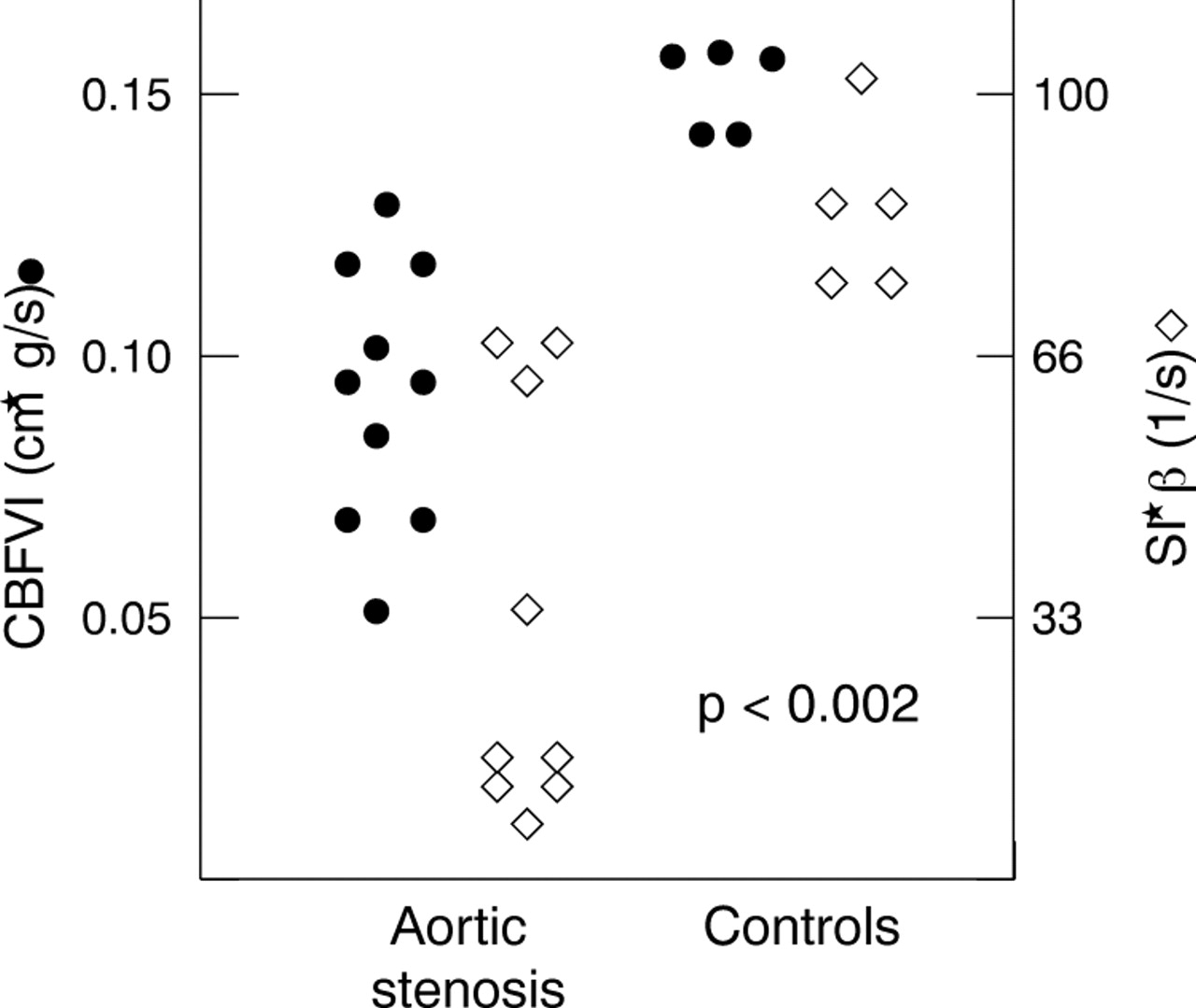
Absolute baseline CBFV was higher in patients than in controls (26 cm/s (22–35) v 20 cm/s (9–22), p = 0.044) but CBFVI was lower in patients than in controls (0.100 cm·g/s (0.07–0.115) v 0.130 cm·g/s (0.130–0.160), p = 0.002) (fig 4). Coronary blood flow reserve was lower in patients with aortic stenosis than in controls (1.6 (1.3–1.9) v 2.6 (2.5–2.7), p < 0.001). SI*β, the best approximation of microvascular flow at MCE, was significantly lower in patients than in controls (11 1/s (8–66) v 83 l/s (73–95), p = 0.001). A high correlation between CBFVI and SI*β was found (r = 0.86, p < 0.001).

Individual data points of coronary blood flow velocity index (CBFVI) (circles) and signal intensity times signal intensity rise (SI*β) at myocardial contrast echocardiography (diamonds) in patients with severe aortic stenosis and in controls.
Apoptosis
Apoptosis rate was significantly higher in patients than in controls (1.2% (0.8–1.4) v 0.01% (0.01–0.02), p < 0.001) (fig 5). Features of myocardial necrosis were not encountered.
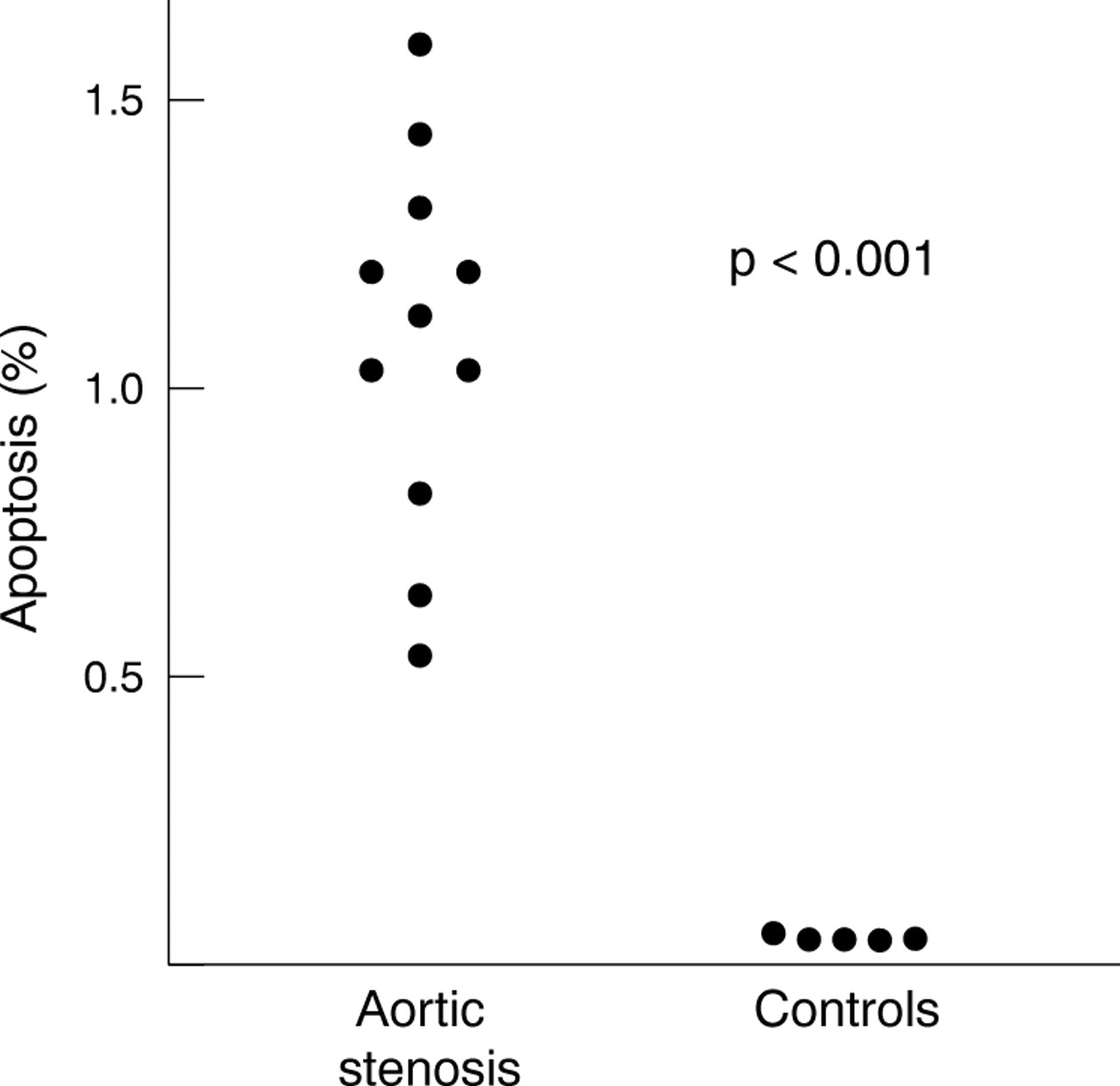
Individual data points showing increased cardiomyocyte apoptosis in patients with severe aortic stenosis versus controls.
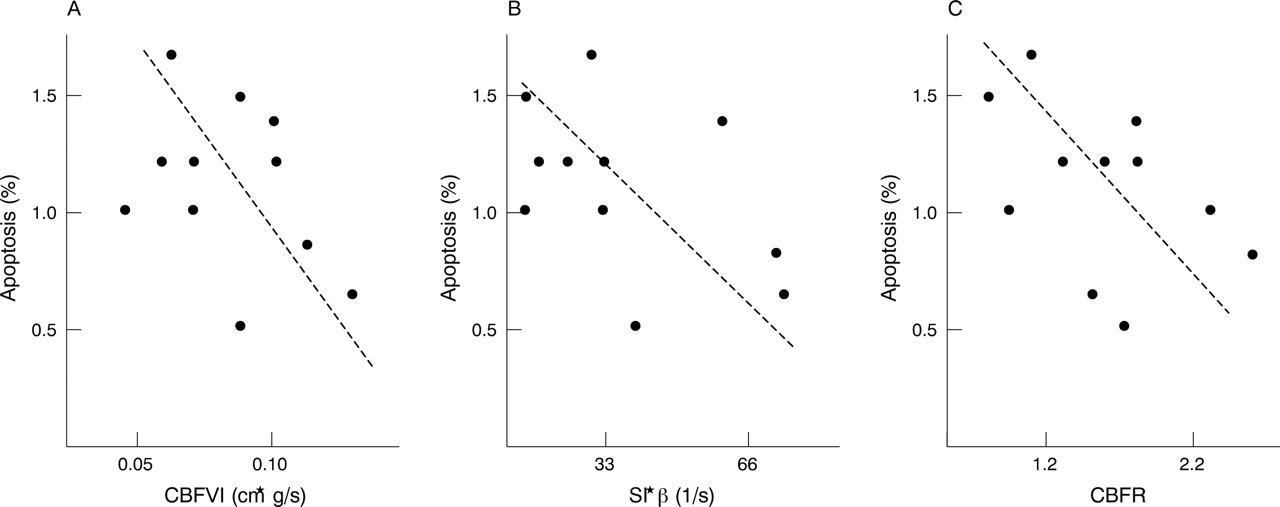
In patients with aortic stenosis, apoptotic rate correlated significantly with LV mass (r = 0.57, p = 0.029) and LV mass index (r = 0.59, p = 0.021). Apoptosis rate was also inversely correlated with CBFVI (r = −0.77, p = 0.001) and with coronary blood flow reserve (r = −0.83, p < 0.001). Moreover, apoptosis significantly correlated with myocardial flow as expressed by SI*β at MCE (r = −0.77, p = 0.001) (fig 6).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Correlation between apoptosis and indexes of myocardial perfusions. Correlation between (A) apoptotic rates and CBFVI and (B) SI*β at myocardial contrast echocardiography. (C) Correlation between apoptosis and coronary blood flow reserve (CBFR) at coronary artery Doppler analysis after adenosine challenge.
DISCUSSION
This study documents for the first time that patients with severe aortic stenosis and LV hypertrophy have reduced myocardial blood flow as quantified by transthoracic Doppler echocardiography and MCE. More important, reduction of flow is strongly associated with increased cardiomyocyte apoptosis, as shown in biopsy samples.
These novel findings from innovative methods of non-invasive quantification of coronary and myocardial blood flow and in vivo determination of apoptosis led to the hypothesis that pressure overload produced by severe aortic stenosis may lead to decompensated heart failure through oxygen demand–supply imbalance, producing progressive cardiomyocyte loss by apoptosis.
Non-invasive evaluation of coronary and myocardial blood flow
One of the novelties of this study is the non-invasive evaluation of CBFV by transthoracic Doppler echocardiography and of myocardial flow by MCE. Transthoracic assessment of Doppler flow velocity of the mid LAD has been previously validated12 and it has been shown to be a reliable indicator of the presence and severity of coronary artery disease.14 On the other hand, data on LAD flow velocity in patients with microvascular flow impairment are only preliminary.15 This is the first report of LAD flow velocity assessment in patients with severe aortic stenosis in the absence of coronary artery disease.
In our study population, rest flow velocity was higher in patients than in controls, yet LV mass corrected CBFV was reduced in patients with aortic stenosis compared with controls, thus suggesting a microvascular flow mismatch in the hypertrophied LV wall, in agreement with previous studies.16 Structural abnormalities of intramural vessels in cardiac hypertrophy have also been described,17 and reductions in CBFV and coronary flow reserve correlate with LV mass.18 The finding of normal absolute CBFV values with reduced LV mass corrected CBFV supports the concept that coronary arterioles cannot spread in parallel with the increase of myocardial mass during pressure overload hypertrophy, causing an oxygen demand–supply imbalance.
In our study, microvascular flow impairment was confirmed by quantitative analysis of MCE. This non-invasive imaging technique provides important information on microvascular flow pattern, as air or gas microbubbles are pure intravascular tracers.19 Appropriate applications of novel ultrasound detection methods to the principles of destruction and replenishment of bubbles in the imaging field have allowed reliable quantification of microvascular flow.13
In this study, for the first time, microvascular flow has been quantified by echocardiographic methods within the hypertrophic wall of patients with severe aortic stenosis and it has been found to be reduced compared with controls. This impairment of flow has been shown by both Doppler and MCE and the strong correlation between the two novel methods further confirms that they are looking at the same real phenomenon.
Cardiomyocyte apoptosis in aortic stenosis
Our biopsy findings confirm the increase in cardiomyocyte apoptosis in patients with severe aortic stenosis and LV hypertrophy. More important, our data show for the first time an inverse correlation between apoptotic rates and myocardial perfusion.
Several experimental studies have shown that apoptosis may be important in the transition from compensated hypertrophy to failure in pressure overloaded hearts.6–8
Very recently Hein et al4 for the first time reported the presence of ongoing myocyte death in hearts of patient with aortic stenosis. Their study found a prevalence of active (programmed) cell death in approximately 0.6% of cells, although, according to their findings, a novel modality of programmed cell death that may differ from apoptosis (autophagy) appeared to be more prevalent than apoptosis itself.
The finding in our study of increased apoptosis in severe aortic stenosis despite the presence of normal global LV function suggests that apoptosis may be the cause rather than a consequence of unfavourable remodelling. However, although the high rate of apoptosis suggests an active role in adverse remodelling in valvar heart disease, the effective impact of apoptosis is still to be determined, since many features of cardiomyocyte apoptosis are still unclear (for example, the exact duration of apoptosis in the human heart in vivo). Furthermore, whereas promising results of anti-apoptotic treatments in preventing LV failure in animal models further support the role of apoptosis,20–22 enhanced stem cell proliferation may offset, at least in part, the potential detrimental effect of apoptosis.23
Sampling biases need also to be considered when comparing our study with others. Our report of high rates of apoptosis in the lateral free wall may lead to overestimation of the global apoptotic burden and may explain apparent discrepancies with the results of the recent study by Hein et al,4 who describe lower rates of apoptosis in the interventricular septum in patients with aortic stenosis than in our study. Notably, in the landmark study by Li et al,24 apoptosis in the transition from compensatory hypertrophy to heart failure was found to be about 10 times higher in the LV free wall than in the septum. Nevertheless, the overall rate of myocyte death in our study (by apoptosis only) and in the study by Hein et al4 (by apoptosis, necrosis, and autophagy) are impressively similar and are similar to the rates observed in the animal model of aortic stenosis described by Ding et al5 (by apoptosis only).
Although we found a close inverse correlation between apoptotic rate and myocardial perfusion, it is important to note that other pathophysiological mechanisms may be considered to explain the excess of apoptosis in patients with aortic stenosis, such as mechanical stress produced on myocardial cells by pressure and volume loading.
Lastly, our study group was made up of consecutive patients with aortic stenosis and we included more female patients (80%). This higher prevalence of women, whereas aortic stenosis is slightly more common in men, can be justified by the inclusion only of patients without coronary artery disease, who are more likely to be women.
Acknowledgments
This study was supported in part by an ONLUS support grant to AB. The authors thank Dr Vera Di Trocchio (Virginia Commonwealth University, Richmond, VA, USA) for her editorial and technical support.
REFERENCES
Footnotes
-
Published Online First 20 May 2005
-
The authors declare no competing interests.
-
This work has been presented in part at the American Heart Association scientific session, New Orleans, 7–10 November 2004, and at the VIII Euroecho meeting, Athens, 1–4 December 2004.
-
Address for reprints: Dr A Abbate, Department of Medicine, Virginia Commonwealth University, 10025 Bellona Court, Richmond, Virginia 23233, USA; abbatea{at}yahoo.com.