Article Text

Abstract
Objective: To assess the association between socioeconomic status and ischaemic heart disease (IHD) mortality in 10 western European populations during the 1990s.
Design: Longitudinal study.
Setting: 10 European populations (95 009 822 person years).
Methods: Longitudinal data on IHD mortality by educational level were obtained from registries in Finland, Norway, Denmark, England/Wales, Belgium, Switzerland, Austria, Turin (Italy), Barcelona (Spain), and Madrid (Spain). Age standardised rates and rate ratios (RRs) of IHD mortality by educational level were calculated by using Poisson regression.
Results: IHD mortality was higher in those with a lower socioeconomic status than in those with a higher socioeconomic status among men aged 30–59 (RR 1.55, 95% confidence interval (CI) 1.51 to 1.60) and 60 years and over (RR 1.22, 95% CI 1.21 to 1.24), and among women aged 30–59 (RR 2.13, 95% CI 1.98 to 2.29) and 60 years and over (RR 1.36, 95% CI 1.33 to 1.38). Socioeconomic disparities in IHD mortality were larger in the Scandinavian countries and England/Wales, of moderate size in Belgium, Switzerland, and Austria, and smaller in southern European populations among men and younger women (p < 0.0001). For elderly women the north–south gradient was smaller and there was less variation between populations. No socioeconomic disparities in IHD mortality existed among elderly men in southern Europe.
Conclusions: Socioeconomic disparities in IHD mortality were larger in northern than in southern European populations during the 1990s. This partly reflects the pattern of socioeconomic disparities in cardiovascular risk factors in Europe. Population wide strategies to reduce risk factor prevalence combined with interventions targeted at the lower socioeconomic groups can contribute to reduce IHD mortality in Europe.
- ICD, International classification of diseases
- IHD, ischaemic heart disease
- RR, rate ratio
- mortality
- heart diseases
- social class
- Europe
Statistics from Altmetric.com
Ischaemic heart disease (IHD) accounts for about 2.7 million deaths every year in the developed world.1 A lower socioeconomic status is associated with a higher risk of dying of IHD,2–6 so that around a quarter of all IHD deaths can be attributed to a lower socioeconomic status.5 IHD is the largest contributor to socioeconomic differences in life expectancy and mortality in Europe.6 Thus, examining IHD disparities is essential to understand recent cardiovascular mortality trends.
During the 1980s, large social class disparities in IHD mortality were reported in northern European populations among middle aged men. In contrast, no social class disparities in IHD mortality existed in southern and Mediterranean countries.2 This north–south gradient suggests that specific risk factors such as the Mediterranean diet may have protected the entire southern European population from higher IHD mortality.7 Furthermore, southern European countries may be lagging behind in the epidemiological transition earlier experienced by northern Europe and the USA.2,8 Consequently, no social class differences in risk factors such as smoking would have yet emerged in southern populations.8 Only through international comparisons is it possible to elucidate the impact of country specific risk factors and health care practices on socioeconomic disparities in IHD mortality.
Previous studies have compared socioeconomic disparities in IHD mortality only among middle aged men based on cross sectional data for some countries.2 Within a large European collaboration, we collated longitudinal data on mortality disparities for a more recent period. This study assessed differences in IHD mortality between socioeconomic groups during the 1990s in 10 western European populations. It is the first study of IHD disparities during this period for both men and women, which also compares middle aged and elderly populations. This is the largest study of socioeconomic differences in IHD mortality ever, comprising more than 95 million person years and around 263 000 deaths. This yielded robust estimates of the association between socioeconomic status and IHD mortality.
METHODS
Data and subjects
Longitudinal data on mortality by educational level, sex, and age were obtained for 10 European populations. Subjects were enumerated during a census in the early 1990s and followed up for different periods (appendix). For each person, information on cause of death was obtained from national statistics registries and linked to census data on educational level. Most studies covered the entire national population, except for Madrid (regional), Barcelona and Turin (urban), Switzerland (population living in German speaking areas), and England/Wales (1% representative sample of the population). Populations were selected to represent different geographical regions (for example, northern or southern) in western Europe. Longitudinal data were not available or linkage between census and mortality registry data was not possible for other western European countries. People aged 30 years and over (age specified at the start of follow up) were studied, except in Denmark, where data on education were not available for people aged 70 years or more.
Educational level was used as an indicator of socioeconomic status and assessed at baseline for each person. As opposed to occupational class, educational level can be applied equally to both men and women, it is more comparable between age groups, and it comprises both economically active and inactive populations.9 It is also more comparable across countries than other indicators such as income.9 Education was first coded according to national schemes and subsequently reclassified into three equivalent categories so that the size of the low educational level group was similar across countries. Data on the distribution of education by country have been reported elsewhere.10 These groups corresponded roughly to levels 0–2 (pre-primary, primary, and lower secondary education), 3 (upper secondary education), and 4–6 (postsecondary education) of the Unesco standard classification scheme. In most countries, about 65–80% of the population had a low educational level, 15–30% had a middle educational level, and about 10–15% had a high educational level.
Causes of death were coded according to the International classification of diseases (ICD), ninth revision (ICD-9), in most countries. IHD was defined as code numbers 410–414, stroke as code numbers 430–438, and lung cancer as code numbers 162, 163, and 165. The only exceptions were Denmark and Switzerland, where codes 410–414 (IHD), 430–438 (stroke), and 162–163 (lung cancer) from the ICD-8 and codes I20–I25 (IHD), I60–I69 (stroke), and C33, C34, and C39 (lung cancer) from the ICD-10 were used.
Methods of analyses
Age standardised mortality rates were calculated for sex and educational level strata distinguishing two age groups: 30–59; and 60 years and over. Data were analysed separately for these two age groups because IHD mortality increases sharply from age about 60 years upwards, particularly for men. Nevertheless, analyses were replicated for age groups 30–65 and 65 years and over, yielding similar results. Rates were standardised by five year age groups by the direct method and the European Union population of 1995 as the standard.11 Each population separately and a pooled dataset of all countries weighted on the size of each cohort were analysed.
Age adjusted rate ratios (RRs) were calculated by Poisson regression. RRs compared the mortality of low and middle/high combined educational level groups, with the combined middle/high group serving as the reference category. Owing to their small size, middle and high levels were combined to obtain more precise estimates. Tables and figures present results organised according to countries’ approximate geographical latitude in western Europe.
Comparable RR estimates of mortality according to educational level were calculated for stroke and lung cancer, which share some determinants with IHD such as smoking and hypertension. The international pattern for IHD and these causes of death were compared, which can shed light on shared determinants that may contribute to socioeconomic differences in IHD mortality in Europe. Data were analysed with SAS, version 8.2 (SAS Institute, Cary, North Carolina, USA).
RESULTS
In 44 673 469 person years, 146 043 men died of IHD. Table 1 shows that, among middle aged men (30–59 years), IHD mortality was higher among lower than among higher educational level groups in all populations. Among elderly men (60 years and over), IHD mortality differed by educational level in all but southern European populations (table 1). Among both middle aged and elderly men, socioeconomic differences in IHD mortality were generally larger in Scandinavian countries and England/Wales, of moderate size in Belgium, Austria, and Switzerland, and smaller in Turin, Barcelona, and Madrid (test for interaction between education and country, p < 0.0001). This north–south gradient was consistent both for relative and absolute differences in IHD mortality.
Among women, 117 802 died of IHD over 50 336 353 person years. Table 2 shows that IHD mortality was higher among lower educated women in all populations. Despite wide confidence intervals (CIs), RRs were generally larger in northern than in southern European populations for middle aged women (test for interaction between education and country, p < 0.0001). Among elderly women, however, this north–south gradient was smaller: although there were no socioeconomic disparities in IHD mortality in Madrid and Turin, disparities were large in Barcelona and RRs in other populations were generally close to the European average (RR 1.36, 95% CI 1.33 to 1.38). Absolute rate differences between educational groups were larger in northern than in southern populations among women in both age groups (tables 1 and 2). RRs were larger for women than for men in most populations, whereas absolute rate differences were generally larger for men than for women.
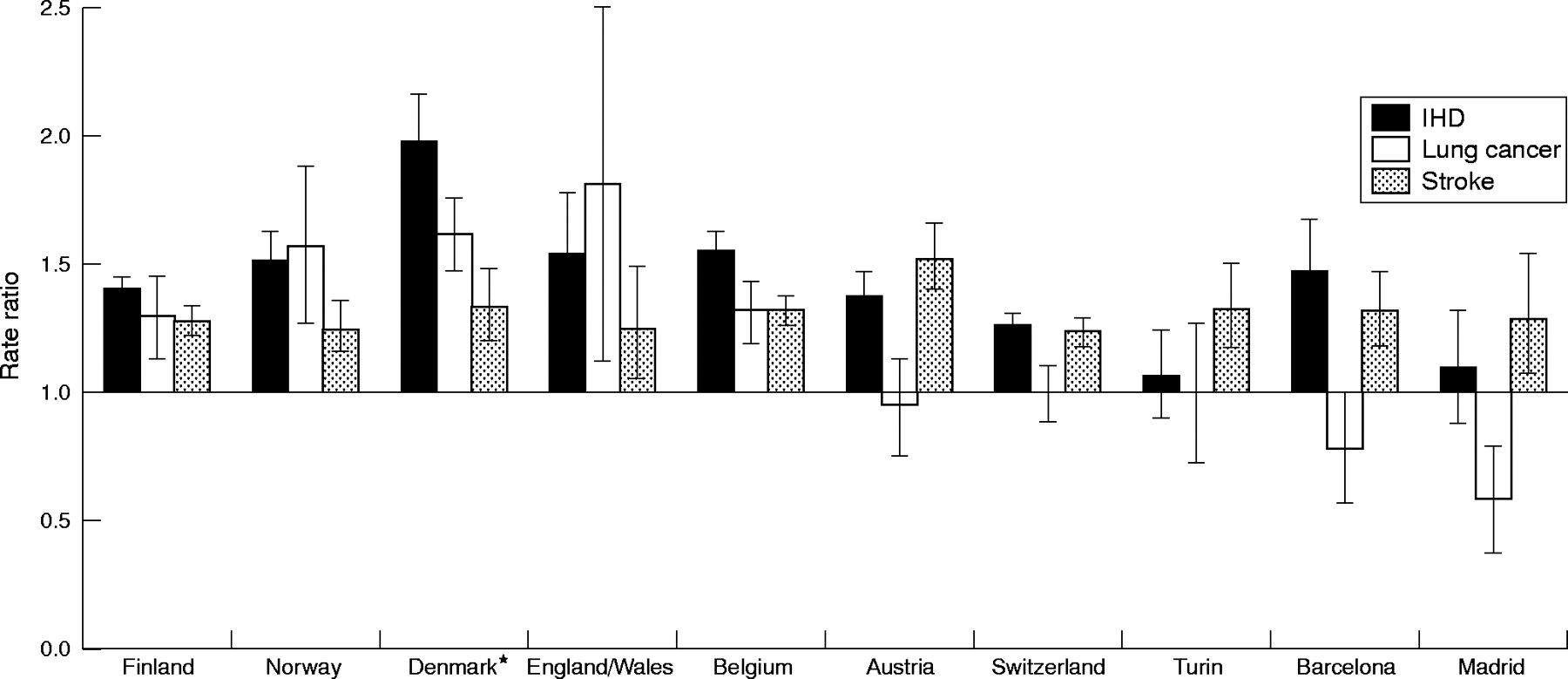
Figure 1 shows a pronounced north–south gradient in educational differences in IHD mortality among men aged 30 years and over. This north–south pattern existed also among women, with the exception of Barcelona, which had a relatively large RR for IHD (fig 2). Despite wide CIs, RRs for lung cancer mortality were larger in northern populations and smaller in southern populations in comparison to the European average for men (RR 1.62, 95% CI 1.59 to 1.66) and women (RR 1.17, 95% CI 1.12 to 1.23). In contrast, educational disparities in stroke mortality were of a similar magnitude in most populations and were all close to the European average among men (RR 1.27, 95% CI 1.24 to 1.30) and women (RR 1.29, 95% CI 1.27 to 1.32).
DISCUSSION
Previous studies have shown that IHD mortality is low in southern and Mediterranean populations and high in the north of Europe.12 We have shown that socioeconomic differences in IHD mortality during the 1990s were larger in Scandinavian countries and England/Wales, of a moderate size in Belgium, Austria, and Switzerland, and smaller in Turin, Barcelona, and Madrid. This north–south gradient was smaller among elderly women, with less variation between populations. These findings suggest that the association between socioeconomic status and IHD not only changes over time3,4 but also varies considerably between countries.
Evaluation of data and study limitations
We used the most recent data on IHD disparities in Europe. Nevertheless, some limitations in this study should be considered. Firstly, IHD deaths may be wrongly coded as other causes of death.13 This would bias our results if a greater proportion of southern populations and more lower than higher educated people were misclassified. To assess the impact of this problem, we assessed the pattern of educational disparities for a combined category of IHD and other heart diseases (ICD-9 codes 416 and 420–429). Although north–south gradients in IHD disparities were somewhat smaller for women and middle aged men, the north–south gradient for elderly men remained strong. Furthermore, our findings are consistent with studies showing a north–south gradient in cardiovascular risk factors in Europe.14–16 Thus, there is no clear evidence that our results can be explained by misclassification.
Despite our efforts at standardisation, differences remained between countries in measurements and data collection. Data for Madrid and Austria comprised a shorter follow up period. However, research indicates that mortality differentials by educational level are unrelated to follow up time.17 Thus, any bias caused by this problem is likely to be small. Furthermore, we used a different revision of the ICD code for Switzerland and Denmark, which may influence overall mortality. However, this is unlikely to affect RRs that compare mortality between educational level groups.
Although census data were collected by standard procedures, differences between populations may remain in the precision with which educational level was measured. However, if measurement precision differed systematically between northern and southern countries, a north–south gradient would have also been observed for other causes of death. Instead, we did not observe a north–south gradient for disparities in most other causes, including stroke and all cause mortality.6,10,18 Furthermore, we reclassified national levels into broad categories,10 thus minimising the impact of misclassification across country specific educational levels. Thus, misclassification of educational attainment is unlikely to explain our findings.
Except in Switzerland, where the proportion of highly educated people was larger, the distribution of educational level was comparable between countries.10 Thus, our study compared the effect of relative—as opposed to absolute—socioeconomic position on IHD mortality between populations. However, reclassified categories corresponded roughly with the Unesco standard classification.10 Furthermore, sensitivity analyses based in the relative index of inequality (an effect measure that is based on all educational levels and simultaneously adjusts for differences in the educational distribution)19 showed an identical pattern (results not shown). Thus, results are likely to be comparable when assessing the effect of absolute educational level. Nevertheless, we do not know whether findings would be similar when dividing the lower educated group into more specific levels.
Data for Switzerland can only be generalised to the German speaking population. However, this corresponds to about 72% of the entire Swiss population. The dataset for most countries comprised the national population or a representative sample of the total population, whereas only regional or urban data were available for southern Europe. However, previous studies of national data have also reported smaller IHD disparities in southern countries such as Spain and Portugal.2 Furthermore, urban areas are often in a more advanced stage of the epidemiological transition, so that socioeconomic differences in mortality are generally larger within cities than at the national level.20 Thus, by including national estimates for Italy and Spain, the north–south contrast in educational disparities in IHD mortality is likely to be greater than that observed in our study.
Comparison with previous studies
Previous research reported a north–south gradient in social class differences in IHD mortality among middle aged men during the 1980s.2 Our findings suggest that this north–south gradient also existed during the 1990s, for middle aged men and women and for elderly men. These findings are interesting in the context of previous research showing that overall IHD mortality is also lower in southern European countries and France than in northern countries such as Finland.12 Our data also show a north–south gradient in overall IHD mortality, for both the higher and the lower socioeconomic groups separately (tables 1 and 2). However, this north–south gradient was greater among the lower socioeconomic classes. This pattern resulted in both lower IHD mortality and smaller socioeconomic differences in IHD mortality in southern than in northern European populations.
Austria, Belgium, and Switzerland generally occupied an intermediate position in the size of educational differences in IHD mortality. This further highlights the persistence of the north–south gradient throughout western Europe. Previous studies reported that the pattern for Switzerland resembled that for Mediterranean populations.2 However, previous research relied on cross sectional and occupational data for this country and may have been biased by excluding economically inactive people.9,17
Previous studies suggested that socioeconomic differences in IHD mortality started to emerge in southern populations during the 1990s.3,4 Although our data are not fully comparable with data from previous studies,2,3 our results suggest that socioeconomic disparities in IHD mortality may have indeed recently emerged in younger cohorts in Italy and Spain, particularly among men. In contrast, no disparities existed among elderly men. Nevertheless, socioeconomic differences in IHD mortality were still smaller in southern than in other European populations.
Explanation of results
Our results raise questions about risk factors for IHD that may explain the north–south gradient in IHD disparities, among which smoking is an interesting candidate. Research indicates that smoking diffuses within societies as an epidemic.8 It is first adopted by the higher socioeconomic classes; subsequently, smoking declines among the higher classes and spreads rapidly among the lower socioeconomic groups.8 Whereas northern European countries and the USA have already experienced this transition, the smoking epidemic is far less advanced in Spain and Italy.8,14,21,22 These findings are in line with the pattern we observed for lung cancer mortality, which partly reflects smoking prevalence during previous decades.8,22 Our study shows that socioeconomic disparities in lung cancer mortality tended to be larger in northern than in southern European populations. Accordingly, a striking north–south gradient in socioeconomic disparities in smoking has been reported in Europe.14 This lag in the progression of the smoking epidemic in southern as compared with northern populations may partly explain why socioeconomic differences in IHD mortality are smaller in the south than in the north of Europe.
Other risk factors, however, have traditionally protected southern European populations from higher IHD rates, which may have benefited all social classes equally. Adherence to the Mediterranean diet can reduce the risk of dying of IHD as much as 40%.7 Previous research has shown that a healthy diet based on vegetables, fruits, and olive oil is generally available to all in southern Europe but only to the higher socioeconomic groups in northern populations.15,16 The Mediterranean diet may thus contribute not only to low IHD mortality but also to small socioeconomic differences in IHD mortality in southern Europe. Similarly, larger socioeconomic disparities in excessive alcohol consumption exist among men in Scandinavian countries and the UK,15,16,23 whereas alcohol disparities are small in most southern countries.15 Lastly, socioeconomic disparities in overweight and obesity among men are smaller in southern than in northern European populations.15,24 These factors may have protected the entire southern European population from higher IHD mortality.
Cross country variation was smaller in socioeconomic disparities in IHD mortality among elderly women. Owing to the low prevalence of smoking in this group,14 relatively few IHD deaths might be attributable to this risk factor in older women. Thus, other factors may have had a more prominent role. Obesity, an important predictor of cardiovascular risk among women, is a plausible candidate. The consistency of socioeconomic disparities in IHD mortality among elderly women may result from lasting socioeconomic disparities in obesity. Since the 1960s, a higher prevalence of obesity in lower than in higher socioeconomic groups has been observed among women in Europe.25 These disparities are larger and have existed for a longer period among women than among men.15,24,25 Thus, the obesity epidemic may have preceded the smoking epidemic that occurred decades later8,14,21 and influenced the pattern of IHD disparities only for younger women. Obesity may have also partly contributed to larger socioeconomic disparities in IHD mortality among women than among men in Europe.
The north–south gradient in socioeconomic disparities in IHD mortality was not observed for stroke.18 This raises questions about other risk factors that may explain the similarities in the size of stroke disparities in Europe. A possible candidate is hypertension, a major risk factor for stroke. There are socioeconomic differences in the prevalence and treatment of hypertension in Europe,26,27 which may have a role in the consistency of stroke disparities. However, a different pattern may exist for the two broadest categories of stroke: trends in IHD and cerebral infarct have had a similar pattern, whereas trends in cerebral haemorrhage mortality are very different.28 Thus, the pattern of socioeconomic disparities in cerebral infarction may resemble that for IHD mortality, whereas other determinants such as adverse childhood circumstances may contribute to similar socioeconomic disparities in cerebral haemorrhage in European populations.29 Further research should compare socioeconomic disparities in stroke subtypes and IHD mortality in Europe.
Absolute differences in IHD mortality were largest among those aged 60 years and over. However, the strength of the relative association between socioeconomic status and IHD mortality declined with age. This may be partly explained by the differential effect of selective survival. People with a lower socioeconomic status may have died earlier and only the healthiest may have survived into old age. Consequently, socioeconomic differences in IHD mortality diminished at older ages. However, previous research indicates that selective survival cannot fully explain this age pattern.30 Further research is warranted to assess the impact of this mechanism.
Lastly, inequity in health care access may have also contributed to socioeconomic disparities in IHD mortality. Inequity in access to procedures such as coronary artery bypass surgery and angiography has been reported both in northern31 and in southern populations.32 Similarly, inequity in specialist care persists in most European countries.33 Nevertheless, countries with more egalitarian policies such as the Scandinavian populations had larger socioeconomic disparities in IHD mortality than southern populations. Thus, it is uncertain to what extent health care disparities contribute to cross country variations in socioeconomic disparities in IHD mortality in Europe.
Clinical implications
We observed smaller socioeconomic disparities in IHD mortality in southern European populations, where overall IHD mortality is low.12 A strategy to reduce IHD disparities may comprise two complementary approaches. Firstly, population wide strategies to decrease the overall prevalence of risk factors such as diet and obesity may provide great benefits to reduce both overall IHD mortality and IHD disparities.5 Secondly, interventions to reduce the prevalence of risk factors such as smoking14,34 targeted at the lower socioeconomic groups can boost the impact of interventions in this high risk population. Furthermore, clinicians are confronted with a large number of low socioeconomic status patients.33 Therefore, clinicians can contribute to improved survival after the first occurrence of heart disease by assuring equal access to secondary prevention and care for patients from the lower socioeconomic groups.31,32 Cross country variations suggest that specific interventions and policies may be required for each country. In conclusion, population wide strategies to reduce the prevalence of risk factors such as diet combined with prevention of risk factors such as smoking targeted at the lower socioeconomic groups are likely to contribute to reduced IHD mortality in Europe.
APPENDIX
Follow up period, number of person years at risk, and ischaemic heart disease deaths among men and women aged ⩾30 years in 10 western European populations
Age standardised ischaemic heart disease (IHD) mortality (per 100000 person years) by educational level and rate ratio of low versus middle/high education groups among men aged ⩾30 years
Age standardised IHD mortality (per 100000 person years) by educational level and rate ratio of low versus middle/high education groups among women aged ⩾30 years

Rate ratios of ischaemic heart disease (IHD), lung cancer, and stroke mortality according to educational level for men aged 30 years and over in western Europe. *Ages 30–69 years.
{kind=link}
{kind=link}
Rate ratio of IHD, lung cancer, and stroke mortality according to educational level for women aged 30 years and over in western Europe. *Ages 30–69 years.
Acknowledgments
This study is based on a grant of the Fifth Framework Programme on Quality of Life and Management of Living Resources of the European Union (contract QLK6-CT-1999-02161). The Swiss National Science Foundation supported the construction of the Swiss National Cohort (grants no 32-5884.98 and no 32-63625.00). Frank van Lenthe is supported by a grant from the Netherlands Organisation for Scientific Research (NWO grant no 904-66-104). The authors thank Professor G A M Van den Bos and Dr Hendriek Boshuizen for their valuable comments. We thank Dr Otto Andersen for his help with the Danish data.
REFERENCES
Footnotes
-
↵* Also the National Institute of Public Health and the Environment, Bilthoven, the Netherlands
-
Published Online First 10 October 2005
-
Funding sources had no role in the design, data collection, analysis, interpretation, or reporting of data, nor in the decision to submit the paper for publication. The authors of the paper are pleased to declare no competing interests. This study was based on existing data from census and mortality registries in Europe. Therefore, ethics approval was not necessary for the conduction of the study.