Article Text

Abstract
Objective: To confirm the overall benefit of drug eluting stents (DES), to evaluate the effect of different DES, and to assess the global safety of DES compared with bare stents through a meta-analysis of randomised controlled trials.
Methods: Randomised controlled trials comparing sirolimus and derivates or paclitaxel and derivates eluting stents versus bare stents. Binary restenosis and major adverse cardiac events (MACE) were chosen as primary end points. Death, Q wave myocardial infarction (MI), and stent thrombosis up to 12 months’ follow up were also analysed.
Results: MACE overall occurrence was highly reduced with DES from 19.9% to 10.1% (odds ratio (OR) 0.46, 95% confidence interval (CI) 0.41 to 0.52, p < 0.001). A significant heterogeneity (p < 0.001) was found between subgroups according to the drug: MACE OR was 0.28 (95% CI 0.22 to 0.35) in the sirolimus subgroup and 0.62 (95% CI 0.53 to 0.73) in the paclitaxel subgroup. Restenosis was also highly reduced from 31.7% with bare stents to 10.5% with DES (OR 0.25, 95% CI 0.22 to 0.29, p < 0.001) with a similar heterogeneity between subgroups. Mortality, Q wave MI, and stent thrombosis were not significantly different between DES and control group, whereas Q wave MI and stent thrombosis tended to be more frequent with paclitaxel.
Conclusion: This meta-analysis confirms the overall benefit of DES on restenosis and MACE with significant heterogeneity between drugs, suggesting higher efficacy of sirolimus eluting stents. Additional data with longer follow up and in high risk populations are needed to clarify issues on stent thrombosis.
- CI, confidence interval
- DES, drug eluting stents
- ENDEAVOR, randomised, controlled trial of the Medtronic Endeavor drug (ABT-578) eluting coronary stent system versus the Taxus paclitaxel eluting coronary stent system in de novo native coronary artery lesions
- FDA, Food and Drug Administration
- MACE, major adverse cardiac events
- MI, myocardial infarction
- OR, odds ratio
- SCORE, study to compare restenosis rate between quest and quads-QP2
- SIRIUS, sirolimus eluting balloon expandable stent in the treatment of patients with de novo native coronary artery lesions
- drug eluting stents
- meta-analysis
- coronary stenting
- sirolimus
- paclitaxel
Statistics from Altmetric.com
- CI, confidence interval
- DES, drug eluting stents
- ENDEAVOR, randomised, controlled trial of the Medtronic Endeavor drug (ABT-578) eluting coronary stent system versus the Taxus paclitaxel eluting coronary stent system in de novo native coronary artery lesions
- FDA, Food and Drug Administration
- MACE, major adverse cardiac events
- MI, myocardial infarction
- OR, odds ratio
- SCORE, study to compare restenosis rate between quest and quads-QP2
- SIRIUS, sirolimus eluting balloon expandable stent in the treatment of patients with de novo native coronary artery lesions
Since the advent of coronary balloon angioplasty, prevention of restenosis has been the unfulfilled objective of many studies. Despite the impact of stent implantation on angiographic and clinical outcomes, in-stent restenosis has remained the major limitation of catheter based intervention.1–4
Recently, drug eluting stents (DES) have been hailed as the new and only effective means to prevent restenosis. Two DES have proved effective in large randomised trials: the sirolimus eluting stent Cypher (Cordis/Johnson & Johnson, Miami Lakes, Florida, USA) and the polymer based paclitaxel eluting stent Taxus (NIRx; Boston Scientific Corp, Natick, Massachusetts, USA). However, concerns have also been raised about the safety of these DES, leading to a US Food and Drug Administration (FDA) advisory notice and strong debates in the interventional cardiology community.5,6 By aggregating all controlled trials we sought to evaluate the global effect of DES on major adverse cardiac events (MACE) and restenosis and the specific effect of paclitaxel (and analogues) and sirolimus (and analogues) eluting stents. This meta-analysis was intended also to determine whether DES increased stent thrombosis and hard clinical events, knowing the limitations of such a meta-analysis.
METHODS
Trials searching
We reviewed randomised trials comparing paclitaxel or sirolimus eluting stents (and analogues of both drugs) with bare metal stents. We searched Medline from January 1996 up to September 2005 and the Cochrane controlled trials register. The key words used were “drug eluting stents”, “sirolimus”, “everolimus”, “rapamycin”, “paclitaxel”, “taxane”, “taxol”, and “clinical trial”. In addition, we identified relevant abstracts and presentations at the annual meetings of the American Heart Association, the American College of Cardiology, the European Society of Cardiology, and Transcatheter Cardiovascular Therapeutics from January 2000 to September 2005. Expert slide presentations were consulted on line from tctmd.com to complete data from abstracts. Internet based sources of information on the results for clinical trials in cardiology (http://www.theheart.org and http://www.tctmd.com) were also searched. Lastly we manually searched the reference sections of each retrieved article.
Inclusion criteria and outcome measurement
Paclitaxel is an antimicrotubular agent and was first developed as an antineoplastic agent. We pooled in the same subgroup polymer or non-polymer based paclitaxel as well as taxane eluting stents.7,8 Sirolimus is an immunosuppressant macrolide antibiotic first used to prevent allograft rejection. We pooled in this second subgroup sirolimus, everolimus, and biolimus (ABT 578) eluting stents.9,10
For this meta-analysis, studies were selected if sirolimus or paclitaxel derivatives coated stents were randomly assigned versus bare stent, with at least six months’ follow up duration. To avoid bias of non-publication in this analysis we decided to include at first analogues of both sirolimus and paclitaxel in each related group.
In studies in which doses or kinetics of drug delivery from the stent differed, the subgroups were pooled together in a first step analysis. In a second step analysis we excluded analogues to compare only sirolimus eluting stent (Cypher) with polymer based paclitaxel eluting stent (Taxus).
Two reviewers (CR and PSP) independently extracted the data. Disagreements were resolved by consensus.
The two primary end points of this meta-analysis were angiographic binary restenosis (restenosis > 50% of the luminal diameter) at 6–9 months of follow up and MACE, which was a composite of death, myocardial infarction (MI), and revascularisation. Table 1 reports definitions and characteristics of the trials, and table 2 presents the clinical and angiographic characteristics. We also collected the numbers of deaths, Q wave and non-Q wave MIs, and stent thrombosis in all studies. When information was not available for Q wave MI or stent thrombosis or when Q wave MI was not differentiated from non-Q wave MI, the studies were not used for these end points. These clinical end points were recorded at between 6–12 months according to each clinical trial follow up. Data were extracted in duplicate. We recalculated absolute numbers when percentages were reported.
Trials included in the meta-analysis
Clinical and angiographic characteristics
Statistical analysis
We used different calculation methods for estimation of the overall treatment effect (coated stents versus bare stents) based on odds ratio (OR). Results are presented as the OR calculated by the Mantel-Haenszel method.11 ORs are reported with 95% confidence intervals (CIs). A χ2 test for association on the pooled estimate of OR was performed and significance was set at p = 0.05. For each trial we calculated the OR for MACE, binary restenosis, death, Q wave MI, and stent thrombosis.
In the first step of the meta-analysis a fixed effect model was used. Heterogeneity between trials was tested by a χ2 procedure. When heterogeneity was present a random effect model was then used and sources of heterogeneity were studied.
To test publication bias, we constructed funnel plots and analysed robustness. The number of neutral trials (OR = 1) needed to be added to the meta-analysis to induce a non-significant overall effect was calculated. Lastly, to investigate the relation between baseline risk in the population and treatment effect we studied the so called effect model, which is a the linear regression between event rates in bare stent and DES groups in the different trials, by means of the Walter weighted regression method.12 Meta-analysis calculation (association test), heterogeneity, funnel plot, robustness analysis, and effect model were performed with EasyMA software (www.spc.univ-lyon1.fr/easyma.net/).13
RESULTS
Search results
Fifty four studies were identified as potentially relevant. We excluded seven registries and two clinical trials concerning DES in peripheral arteries. Twenty six other studies were excluded: 12 were single armed,9,14–23 five were historically controlled,24–28 five were not randomised,29–33 two concerned bifurcation lesions with one or two DES,34,35 and two had not enough details for treatment groups or end points (fig 1).36,37

Meta-analysis profile. DES, drug eluting stents; DIABETES, diabetes and sirolimus eluting stent trial; FUTURE, first use to underscore reduction in restenosis with everolimus.
For comparisons between DES and bare metal stents, 19 randomised controlled trials were selected concerning 8987 patients (4574 with DES and 4413 with bare stents). Seven randomised controlled trials tested sirolimus,38–44 one tested biolimus,10 one tested everolimus,45 one tested the taxane analogue QP 2,46 five tested polymer based paclitaxel,47–51 and four tested non-polymer delivered paclitaxel.46,52–56
DES versus bare metal stents
MACE and restenosis
The overall occurrence of MACE was significantly reduced by DES from 19.9% to 10.1% (p < 0.001). Common OR by Mantel-Haenszel method was 0.46 (95% CI 0.41 to 0.52) (fig 2). We observed a significant heterogeneity (p < 0.001) between subgroups with a larger reduction of MACE in the sirolimus subgroup (7.4% v 21.9%, OR 0.28, 95% CI 0.22 to 0.35) than in the paclitaxel subgroup (12% v 18.3%, OR 0.62, 95% CI 0.53 to 0.73). This heterogeneity remained significant when we kept only sirolimus and polymer based paclitaxel stent trials. In this second step analysis, the MACE rate with the commercialised sirolimus eluting stent was 7.5% versus 25.8% with bare stents (OR 0.23, 95% CI 0.18 to 0.30) and the MACE rate with the commercialised polymer based paclitaxel eluting stent was 11.2% versus 17.9% with bare stents (OR 0.59, 95% CI 0.50 to 0.69). An additional analysis in a random effect model found the sirolimus subgroup OR of 0.26 (95% CI 0.18 to 0.36) and the paclitaxel subgroup OR of 0.64 (95% CI 0.50 to 0.81) with confirmed heterogeneity between the two subgroups (p < 0.001).

Odds ratio and p value for major adverse cardiac events (MACE) with DES versus bare metal stents (BMS) and subgroup analysis. The occurrence of MACE was significantly reduced by DES with a larger reduction in the sirolimus subgroup.
The proportion of patients with complete angiographic follow up was > 85% in all studies except in SCORE (study to compare restenosis rate between quest and quads-QP2) (74% follow up), SIRIUS (sirolimus eluting balloon expandable stent in the treatment of patients with de novo native coronary artery lesions) (66% follow up), ENDEAVOR II (randomised, controlled trial of the Medtronic Endeavor drug (ABT-578) eluting coronary stent system versus the Taxus paclitaxel eluting coronary stent system in de novo native coronary artery lesions) (50% of follow up), and DELIVER (43% follow up). Figure 3 shows the restenosis pooled analysis. The overall adjusted rate for angiographic restenosis was 10.5% in the DES group versus 31.7% in the control group (OR 0.25, 95% CI 0.22 to 0.29, p < 0.001). A significant heterogeneity between subgroups was found (p < 0.001). In the sirolimus subgroup, the restenosis adjusted rate was 7.6% with DES versus 36.8% with bare stent (OR 0.14, 95% CI 0.11 to 0.17, p < 0.01). In the paclitaxel subgroup, the restenosis adjusted rate was 12.4% with DES versus 28.4% with bare stent (OR 0.35, 95% CI 0.30 to 0.41, p < 0.001). This heterogeneity between subgroups was found to be significant even when trials with analogues were excluded: restenosis was 6.0% versus 37.9% (OR 0.10, 95% CI 0.08 to 0.13) in the sirolimus group and 12.6% versus 28.0% (OR 0.37, 95% CI 0.31 to 0.43) in polymer based paclitaxel eluting stent group, respectively. Results were also confirmed with a random effect model.

The rate of binary angiographic restenosis was significantly reduced by DES with a larger reduction in the sirolimus subgroup.
The overall adjusted rate for angiographic target lesion revascularisation was 6.2% in the DES group versus 16.6% in the control group (OR 0.36, 95% CI 0.31 to 0.41, p < 0.001). In the sirolimus subgroup, the angiographic target lesion revascularisation adjusted rate was 6.7% with DES versus 16.7% with bare stent (OR 0.20, 95% CI 0.16 to 0.25, p < 0.001). In the paclitaxel subgroup, the angiographic target lesion revascularisation adjusted rate was 8.2% with DES versus 14.7% with bare stent (OR 0.53, 95% CI 0.44 to 0.63, p < 0.001).
Safety
Overall mortality was not significantly different between treatment groups and there was no significant heterogeneity between trials. The overall adjusted percentage was 0.9% with DES versus 1.2% with bare stent (p = 0.92, OR 1.02, 95% CI 0.64 to 1.64) and mortality was not significantly lower with paclitaxel compared with bare stents (fig 4).

Overall mortality at 6–12 months’ follow up was not significantly different between treatment groups.
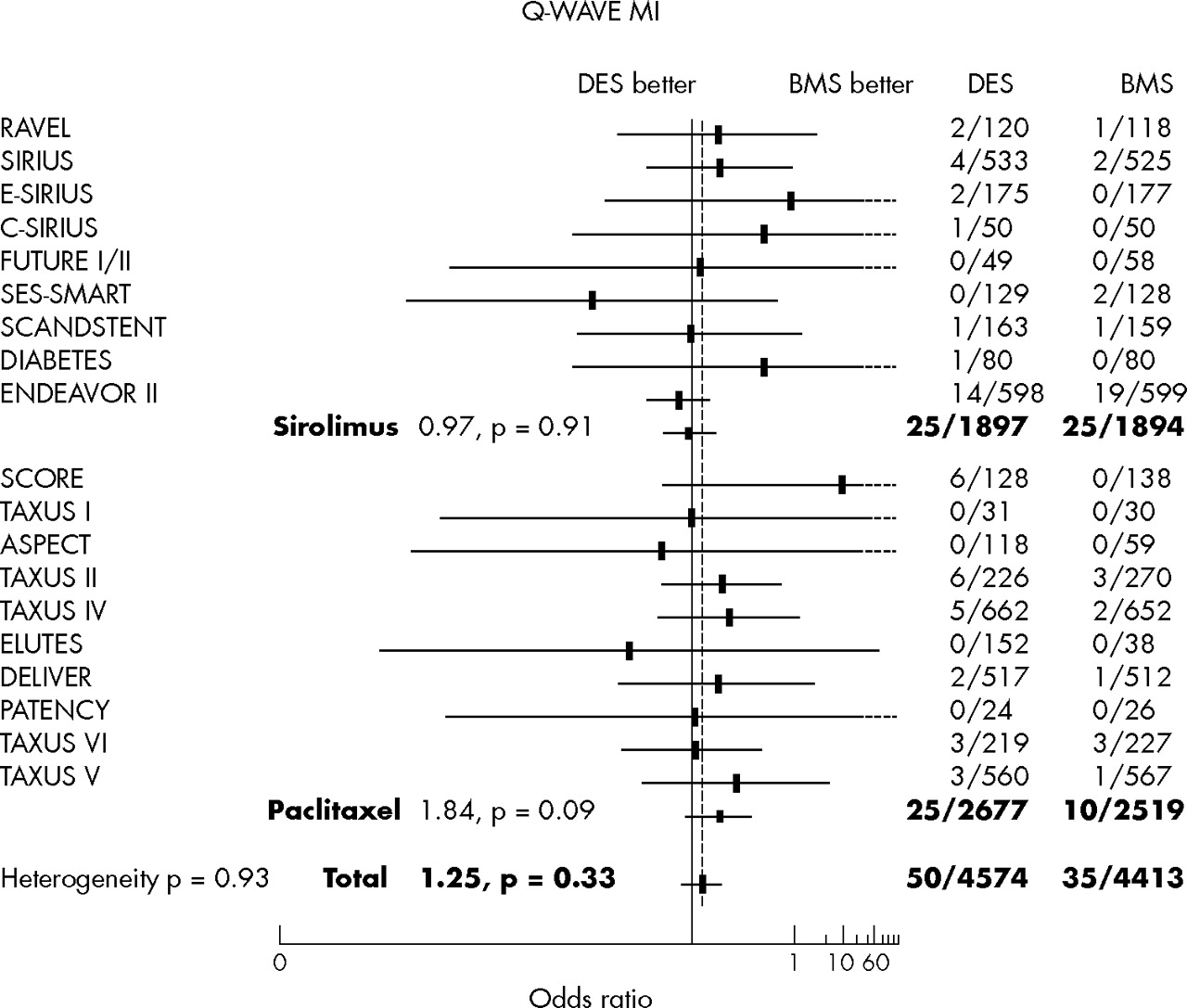
The Q wave MI adjusted percentage was 1.1% with DES versus 0.8% with bare stent (OR 1.25, 95% CI 0.79 to 1.94, p = 0.33) (fig 5) with no significant heterogeneity between trials and more Q wave MI with paclitaxel (p = 0.09).

The overall occurrence of Q wave myocardial infarction (MI) at 6–12 months’ follow up was not different between treatment groups.
The non-Q wave MI adjusted percentage was 2.3% with DES versus 3.28% with bare stent (OR 0.82, 95% CI 0.63 to 1.07, p = 0.14) (fig 6).

The overall occurrence of non-Q wave MI at 6–12 months’ follow up was not different between treatment groups.
The occurrence of stent thrombosis was 0.7% with DES versus 0.8% with bare stent (OR 0.71, 95% CI 0.41 to 1.25, p = 0.24) without heterogeneity between trials but with a trend to more stent thrombosis in the paclitaxel subgroup (fig 7).

The overall occurrence of stent thrombosis was not different between treatment groups.
The different calculation methods provided similar results on outcomes.
Robustness and sensitivity analysis
The robustness test found that more than 10 negative studies (size determined as the mean of included trials) would be necessary to affect the meta-analysis results for MACE and binary restenosis.
The sensitivity analysis for MACE and binary restenosis excluding the three main trials did not change the global results.
Effect model
To investigate whether the effect of DES on MACE was related to the risk of the studied population we performed an effect model analysis. We excluded analogues as well as the trials testing different doses and kept only studies performed with the two marketed DES. Because of the detected heterogeneity between sirolimus and paclitaxel stents, the effect model was analysed separately for these two types of stents. Figure 8 shows results for MACE. The risk ratio (slope) between bare stents and coated stents is different with paclitaxel and sirolimus. The effectiveness of sirolimus eluting stent (relative risk reduction) improved with increasing event rates in the control groups. This is not the case in the paclitaxel eluting stent group, where the relative risk reduction appeared constant whatever the risk in the bare stent group.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Effect model on MACE for polymer based paclitaxel and sirolimus. CI, confidence interval.
DISCUSSION
DES are the most recent breakthrough in the field of interventional cardiology. Their tremendous impact on restenosis in every single trial lifts one of the last barriers to the use of coronary intervention in patients at high risk of restenosis. However, issues have also been raised about the cost effectiveness, the impact on hard clinical events, and the safety of DES.6 Moreover, among the many drugs developed (actinomycin, oestrogens, batimastat, dexamethasone, angiopeptin, etc) the most convincing evidence has emerged with sirolimus and paclitaxel coated stents, but it is uncertain whether these two DES have the same risk to benefit ratio. Babapulle et al57 conducted a meta-analysis on the same subject but our updated results are slightly different. Regarding safety concerns we analysed Q wave MI, instead of all MIs, which are mainly enzymatic rises following percutaneous coronary intervention. We believe that Q wave MI is a harder clinical event probably containing underdiagnosed late stent thrombosis. We also included sirolimus or paclitaxel derivatives to enhance the power to detect infrequent event differences. For the efficacy analysis we choose a two step analysis with comparison of commercially available DES as the second step; we found differences between drugs that were graphically displayed by the effect model analysis.
Our meta-analysis confirms, with good robustness, the very significant reduction of MACE and restenosis by DES compared with bare stents. The heterogeneity between the two subgroups, with larger reductions of these two end points with sirolimus, suggests a more potent effect of sirolimus than of paclitaxel eluting stents. This was confirmed when studies of analogues were excluded from the meta-analysis, evaluating then only commercially available DES. The type of model (random or fixed) did not affect the results either. Acknowledging that MACE are mainly driven by revascularisation for restenosis, these results for the two end points are consistent.
The effect model analysis displays a different efficacy pattern for the two types of DES. The benefit of paclitaxel eluting stent (relative risk) appears constant whatever the level of risk in the bare stent group, whereas the benefit of sirolimus eluting stent increases with increasing risk in the bare stent group. Such a different effect may rely on a more appropriate pharmacological action of sirolimus against intrastent cell proliferation. Obviously, this potential superiority of sirolimus eluting stents has been confirmed in recent head to head trials and a meta-analysis of these trials.58
The present meta-analysis also allows an increase of power to detect small differences that cannot be seen in every trial for rare events. Indeed, in October 2003 the FDA released an advisory notice6 informing physicians about adverse events associated with sirolimus eluting stents. It reported more than 290 cases of thrombosis occurring within the first 30 days of stent implantation and more than 50 reports of apparent hypersensitivity reactions. One month later, the FDA updated this information. We found, compared with bare stents, unfavourable trends for Q wave MI and stent thrombosis with DES driven by paclitaxel studies. However, mortality analysis was reassuring for paclitaxel stents.
For stent thrombosis, the influence of SCORE, which was terminated early due to safety concerns, is important and affects the global result. The SCORE data can have a disproportionate effect, since a major part of the problem was the delivery method, and this is a limitation of the present analysis. No definite conclusion can be drawn but this trend, put into perspective with the FDA report, draws attention to a possible prothrombotic effect. Whether the drug, the dose, the polymer, the coronary anatomy, patients’ characteristics, or the play of chance is involved is still unknown. Future studies, registries, and pharmacovigilance surveys on the use of DES in high risk patients will also help to monitor the safety of DES in real life coronary intervention.
As far as mortality is concerned we did not find a significant difference between bare stents and DES. The recent three year follow up report of the RAVEL (randomised study with sirolimus coated BX velocity balloon expandable stent in the treatment of patients with de novo native coronary lesions) study showed a non-significant increase in death mainly of non-cardiac origin.38 Prolonged follow up of patients enrolled in DES studies is also required after the standard period of observation for restenosis.
Conclusion
A very significant reduction of MACE and restenosis was observed with DES in this meta-analysis. Heterogeneity of benefit according to the type of stent was found for these two end points. The effect model on MACE suggests that patients at high risk of restenosis benefit even more from sirolimus eluting stents. More information needs to be collected to evaluate fairly the safety of DES with regard to thrombotic events.
REFERENCES
Footnotes
-
Published Online First 10 October 2005
Linked Articles
- Miscellanea
- Miscellanea