Article Text

Abstract
Background: The failing Fontan circulation is associated with hepatic impairment. The nature of this liver injury is poorly defined.
Objective: To establish the gross and histological liver changes of patients with Fontan circulation relative to clinical, biochemical and haemodynamic findings.
Methods: Patients were retrospectively assessed for extracardiac Fontan conversion between September 2003 and June 2005, according to an established clinical protocol. Twelve patients, mean age 24.6 (range 15.8–43.4) years were identified. The mean duration since the initial Fontan procedure was 14.1 (range 6.9–26.4) years.
Results: Zonal enhancement of the liver (4/12) on CT was more common in patients with lower hepatic vein pressures (p = 0.007), and in those with absent cardiac cirrhosis on histological examination (p = 0.033). Gastro-oesophageal varices (4/12) were more common in patients with higher hepatic vein pressure (21 (6.3) vs 12.2 (2.2) mm Hg, p = 0.013) and associated with more advanced cirrhosis (p = 0.037). The extent of cirrhosis (7/12) was positively correlated with the hepatic vein pressure (r = 0.83, p = 0.003). A significant positive correlation was found between the Fontan duration and the degree of hepatic fibrosis (r = 0.75, p = 0.013), as well as presence of broad scars (r = 0.71, p = 0.021). Protein-losing enteropathy (5/12) occurred more frequently in patients with longer Fontan duration (11.7 (3.2) vs 17.9 (6.1) years, p = 0.038).
Conclusions: Liver injury, which can be extensive in this patient group, is related to Fontan duration and hepatic vein pressures. CT scan assists non-invasive assessment. Cardiac cirrhosis with the risk of developing gastro-oesophageal varices and regenerative liver nodules, a precursor to hepatocellular carcinoma, is common in this patient group.
- INR, international normalised ratio
- PLE, protein-losing enteropathy
Statistics from Altmetric.com
The Fontan circulation, first introduced in 1968, has undergone many modifications. It results in obligatory central venous hypertension, depressed dynamic cardiac output and impaired ventricular arterial coupling and late ventricular dysfunction.1 These haemodynamic characteristics, combined with longstanding hypoxia preceding the Fontan procedure, are all recognised risk factors for hepatic injury. Liver dysfunction late after the Fontan operation has been suggested in several studies on the basis of liver function tests.2–5 The nature, frequency, severity and reversibility of chronic hepatic dysfunction in this setting are, however, largely unknown.
We hypothesised that raised central venous pressures intrinsic to the Fontan circulation results in hepatic congestion, portal hypertension, arterialisation of liver blood supply and resultant chronic hepatic injury. In this study, we aimed to characterise the nature of chronic liver injury and its determinants, late after the Fontan operation.
METHODS
Setting
Tertiary referral adult congenital heart disease unit.
Patients
All patients referred to the Wessex Adult Congenital Heart Unit, Southampton, UK, between 1 September 2003 and 1 June 2005 for extracardiac cavopulmonary conversion of an older-style Fontan procedure.6 Patients were identified from the Wessex Congenital Heart Disease Database. Our unit had established a clinical protocol of evaluation in September 2003 to assess the suitability and potential risk associated with Fontan conversion. All patients gave informed consent for the individual procedures. This protocol was adopted after our group had experienced recurrent perioperative hepatic and hepatorenal complications, as well as reduced catecholamine sensitivity similar to patients with chronic liver disease.
Clinical protocol
Clinical assessment included detailed history with functional class assessment, clinical examination, exercise tolerance testing (using a modified Bruce protocol), pulmonary function testing, 12-lead electrocardiography, 24 h Holter ECG recording, two-dimensional echocardiogram, cardiac catheterisation and liver biopsy. All patients had detailed laboratory assessment, including measurement of haemoglobin, white cell count, platelet count, electrolytes, international normalised ratio (INR), factor V, renal and liver function tests, glucose, hepatitis A, B and C serology, α1-antitrypsin clearance, iron studies and thyroid function testing.
Haemodynamic assessment
At cardiac catheterisation, conventional angiography and pressure measurements and saturations were performed, including hepatic vein and wedge pressures and saturations. Wedge positions in both the lung and liver were confirmed by contrast injection, through an end-hole balloon-tipped catheter. When unsatisfactory wedge positions were encountered, pressure data were discarded.
Radiological assessment
Multidetector CT images of the abdomen were obtained using an IGE Hispeed Advantage system (General Electric, Milwaukee, Wisconsin, USA) and 150 ml of Visipaque at 5 ml/s. Arterial and portal phase images of the liver were obtained using bolus tracking. All CT scans were independently assessed by a blinded gastrointestinal radiologist (BS). The CT findings were supplemented by abdominal ultrasound results. Abdominal ultrasound was performed by a consultant radiologist in all cases using a Philips/ATL HDI 5000 (Philips Medical Systems, Reigate, Surrey, UK) with a 5–2 MHz convex array probe (C5-2). Intra-abdominal organs were evaluated for size, consistency and any abnormalities of parenchymal texture.
Table 1 displays the baseline clinical characteristics of patients.
Baseline characteristics of patients
Liver biopsy
A transjugular or transfemoral liver biopsy was performed by conventional means at the time of cardiac catheterisation. Biopsy specimens were processed routinely and stained using H&E, Gordon and Sweet’s reticulin, orcein, periodic acid Schiff after diastase digestion and Perl’s Prussian blue stain. Histological analysis was performed by a single experienced observer (HM-S), who was blinded to all clinical data. The histological specimens were graded semiquantitatively (0–4) for extent of fibrosis on reticulin and orcein stains, frequency of broad scars, degree of sinusoidal dilation, hepatocyte atrophy and hepatocyte plate twinning. Fibrosis was scored according to the Laennec Scoring System,7 a minor modification of the METAVIR System.8 Consistent with the METAVIR Fibrosis Score, fibrosis was scored in five grades: 0, no definite fibrosis; 1, minimal fibrosis (no septa or rare thin septum); 2, mild fibrosis (occasional thin septa); 3, moderate fibrosis (moderate thin septa; up to incomplete cirrhosis); 4, cirrhosis definite or probable. According to the Laennec Cirrhosis Scoring System, cirrhosis was scored additionally in three grades: 1, mild cirrhosis, definite or probable; 2, moderate cirrhosis (at least two broad septa); 3, severe cirrhosis (at least one very broad septum or many minute nodules).
Data analysis
Data were analysed with SPSS V.12.0 software. Continuous variables are expressed as mean (SD). Non-parametric data are indicated as median and ranges. Correlations between variables were assessed using a Spearman’s r correlation coefficient. To assess the difference between parameters, Wilcoxon’s rank sum test, Fishers exact test or a t test were performed where appropriate. p Values <0.05 were considered significant.
RESULTS
Baseline clinical characteristics
A total of 12 patients, 9 men, mean (SD) age 24.6 (8) (range 15.8–43.4) years were identified. The mean (SD) age at the initial Fontan procedure was 10.2 (9.9) (range 2.4–36.4) years. Eleven patients had undergone an atriopulmonary Fontan—that is, anastamoses of the right atrial appendage to the main pulmonary artery—whereas one patient had a Kawashima procedure and had previous inclusion of the hepatic veins in the cavopulmonary circuit. The mean (SD) duration since the initial Fontan procedure was 14.1 (5.0) (range 6.9–26.4) years.
The reason for assessment at the Wessex Adult Congenital Heart Unit was subjective deterioration in exercise tolerance in all patients, persistent atrial arrhythmia in eight and worsening peripheral oedema in four patients. Five patients had active protein-losing enteropathy (PLE) at the time of assessment. Paroxysmal atrial arrhythmias were documented as flutter in four, fibrillation in two, and flutter and fibrillation in two patients.
Haematological and biochemical profiles
Table 1 indicates the laboratory characteristics. Seven patients had deranged liver function tests, among whom two had raised alanine aminotransferase levels (48 and 454 IU/l), five had raised alkaline phosphatase level (374 (110.4) IU/l) and seven had raised total bilirubin level (37.5 (21.1) μmol/l). The INR was slightly raised in three patients (1.4–1.5), and the factor V level was decreased in one of eight patients (45 U/dl). Hepatitis serology was negative in all patients, and none of the patients had evidence of iron overload syndrome.
Haemodynamic characteristics
Two patients had moderate or severely depressed systemic ventricular function and one had moderate or severe atrioventricular regurgitation, but preserved ventricular systolic function. The mean (SD) aortic saturation was 94% (4%) (range 87–100%). Hepatic venous haemodynamics were available for all patients, and table 1 indicates their data.
Radiological characteristics
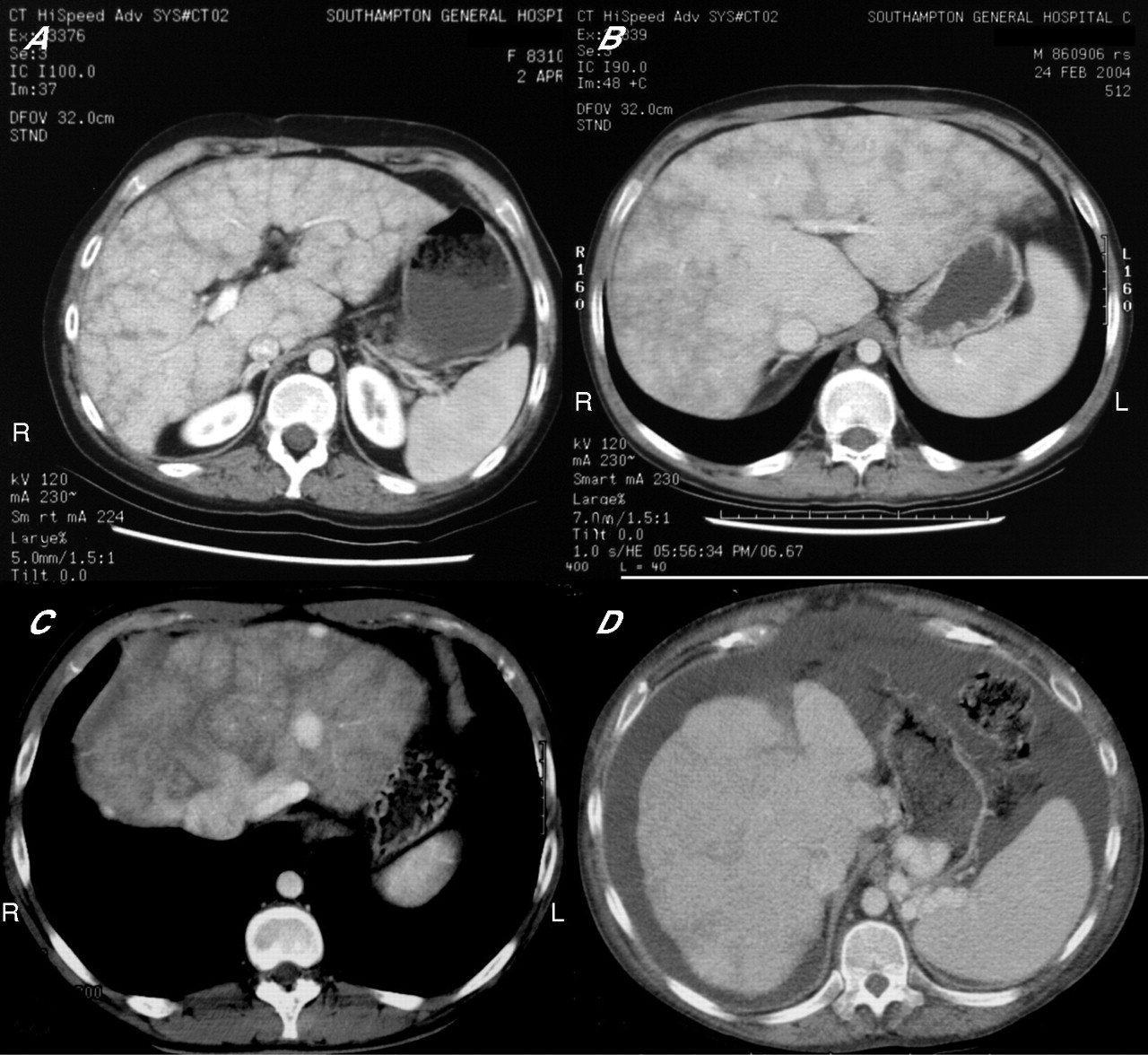
All but one patient had abnormal contrast enhancement on CT. These changes consisted of zonal enhancement—that is, altered enhancement of the liver periphery as compared with the central hilar zone9—in four patients (fig 1B), inhomogeneous parenchymal enhancement or so-called reticular pattern especially in the portal phase in eight patients (fig 1A), and hypervascular nodules in two patients (fig 1C). Multiple collateral vessels where diagnosed in seven patients: extrahepatic venovenous collaterals in six, large gastro-oesophageal varices in four (fig 1D), portopulmonary venous collaterals in two and large intrahepatic veno-venous collaterals in two patients. Other findings were hepatomegaly in 10/11 patients, splenomegaly in 8/11 patients, gallstones in 4/11 patients and ascites in 2/11 patients. Patients with gallstones and ascites had PLE.

(A) Portal-phase CT scan showing reticular pattern of contrast enhancement. (B) Portal-phase CT scan showing a zonal pattern of contrast enhancement (with peripheral reticular enhancement in this case). (C) Arterial-phase CT scan showing three hypervascular liver nodules and dilated hepatic veins with contrast reflux. (D) Portal-phase CT scan of the liver showing large gastro-oesophageal varices and moderate volume ascites.
Histological findings
Parenchymal atrophy and sinusoidal dilatation (fig 2A) with mature sinusoidal collagen deposition (fig 2B) was evident in all patients. Broad scars (fig 2C) were seen in eight patients. In 7/12 patients, cardiac cirrhosis with loss of hepatic architectural integrity was noticed. Evidence of liver cell twinning as a sign of localised parenchymal regeneration was present only in three patients. No biopsy specimen showed signs of active inflammation or extravasation of red cells into the space of Disse. There was no evidence of amiodarone toxicity in any of the biopsy specimens (six patients were taking amiodarone).

{kind=link}
{kind=link}
(A) Biopsy specimen showing marked sinusoidal dilatation, hepatocyte atrophy and an area of scarring with linking of two portal tracts and no visible hepatic vein (H&E stain, ×200 magnification). (B) There is a diffuse pattern of sinusoidal fibrosis, which is irregularly distributed throughout the acinus. The cell plate pattern is deranged with atrophic and twinned cell plates in close proximity (Gordon and Sweet reticulin stain, ×125 magnification). (C) Broad scars of doubly refractile collagen (red–brown) distorting the architecture and causing cirrhosis (Gordon and Sweet reticulin stain, ×125 magnification).
Univariate analyses and interparameter correlations
Patients with zonal enhancement on CT had significantly lower hepatic vein pressures (10.8 (1.5) vs 19 (5.8) mm Hg, p = 0.007), and were significantly less likely to have cirrhosis (3/4 vs 1/7, p = 0.033). Hepatic vein pressures were significantly higher in patients with gastro-oesophageal varices (21 (6.3) vs 12.2 (2.2) mm Hg, p = 0.013) and in patients with cirrhosis (17.7 (6.3) vs 11 (1.7), p = 0.049). The extent of cirrhosis on the histological specimens was positively correlated with hepatic vein pressures (r = 0.83, p = 0.003), and the patients with gastro-oesophageal varices, who all had cirrhosis, were the patients with the highest cirrhosis score (1.5 (0.5) vs 0.5 (0.5), p = 0.037).
A reticular enhancement pattern on portal phase contrast CT was positively associated with the extent of broad scars and the degree of fibrosis on histological examination (3.2 (0.3) vs 1 (1), p = 0.048 and 2.8 (0.2) vs 1.5 (0.5), p = 0.048, respectively). The two patients with hypervascular nodules had hepatic vein pressures of 19 and 30 mm Hg and Fontan pressures of 19 and 28 mm Hg, which were the highest pressures in the group studied.
A significant positive correlation was found between the Fontan duration and the degree of hepatic fibrosis (r = 0.75, p = 0.013), as well as broad scars (r = 0.71, p = 0.021). Aortic saturations were negatively correlated with the hepatic vein wedge pressure (r = −0.79, p = 0.006), and the lowest saturations were in the patients with the highest cirrhosis score (r = −0.66, p = 0.038). PLE was significantly more common in patients with longer Fontan duration (11.7 (3.2) vs 17.9 (6.1) years, p = 0.038).
The five patients with PLE had significantly lower albumin and total protein levels (22 (2) vs 40 (1.5) g/l, p = 0.004 and 48.6 (4.6) vs 79 (3) g/l, p = 0.004, respectively). Also, a significantly raised total bilirubin level was found in the patients with PLE (34.1 (8.1) vs 10.6 (1.1) IU/l, p = 0.006).
DISCUSSION
In this retrospective investigation, we have shown striking abnormalities in gross and histological liver morphology in patients with a failing Fontan circulation.
These data provide objective evidence that liver injury and fibrosis may be related to systemic venous pressures and duration of the Fontan circulation, and confirm the relationship between cardiac cirrhosis and increased right heart pressures suggested in previous postmortem studies.10
Abnormal liver histology has previously been documented in patients with right heart failure. This process usually begins with sinusoidal dilatation, parenchymal atrophy and progressive sinusoidal collagen deposition in the perivenular distribution. As the disease advances, fibrosis extends from the centrilobular zones with the development of reverse lobulation and finally bridging of different (portal–central) vascular structures with fibrotic septa. These profound changes in liver architecture are associated with diffuse sinusoidal fibrosis, which together constitute cardiac cirrhosis.11–13
The similarity of histological appearance in patients with Fontan circulation, albeit much more exaggerated in this group, suggests that similar pathophysiological mechanisms are at work. In the Fontan circulation, central venous pressures are raised by virtue of the absence of a subpulmonary pump, rendering the systemic and pulmonary venous circulations in series. The liver, wedged between the raised pressure of the central venous system and the portal venous circulation, superimposes an additional capillary bed over and above the pulmonary and intestinal arterial capillary beds. Cardiac output is also frequently depressed, thereby providing the ideal substrate for hepatocyte hypoxia, congestion and stimulation of the fibrotic response. Additionally, during atrial contraction, there is marked flow reversal with deep intrahepatic reflux with associated hepatic vein distension, causing stromal stretch and compression of the adjacent hepatocyte cell plates. Mechanotransduction associated with stretch and compression may be a potent inducer and/or modulator of hepatic fibrosis.14 Our data suggest that the degree of collagen deposition and fibrosis is significantly related to the duration of the Fontan circulation and that cirrhosis was more common in those with raised venous pressures, underscoring the important role of central venous hypertension in the progression of liver injury. None of the patients in this small series had Fontan pathway obstruction, to account for the abnormally raised venous pressures.
The relatively low hepatic vein wedge pressures, and absence of significant gradient between wedged and unwedged positions, was an unexpected finding. However, this finding is consistent with previous studies.15 Whether the unique changes in hepatic arterial and venous perfusion lead to a low transhepatic gradient or to an inability to estimate the portal pressure via hepatic vein wedge pressure needs further evaluation, and might only be appreciated from direct cannulation of the portal circulation.
Our data also suggest that the radiological appearances of the liver on a CT scan may aid in defining liver injury. Zonal enhancement, representing a diminished peripheral portal perfusion, while conserving central perihilar perfusion, was present in patients with lower hepatic venous pressures and absent in those with more advanced cirrhosis. Zonal perfusion relies on relatively preserved perihilar vascular integrity, which by definition is lost in the setting of advanced cirrhosis. A heterogeneous contrast enhancement (reticular pattern) pattern has been described in hepatic congestion due to heart failure and Budd–Chiari syndrome.16 In our series, patients with a reticular pattern were more likely to have advanced fibrosis. This connection has previously been suggested in an arterial portography study of patients with chronic liver disease.17
For the first time, we describe hypervascular liver nodules in the context of Fontan circulation. These had the characteristics of benign arterialised regenerative nodules as described in patients with hepatic venous hypertension.18 They represent localised hyperenhancement of the radiological contrast agent on arterial phase imaging.19 Worryingly, regenerative nodules may be associated with the development of hepatocellular carcinoma in the setting of chronic liver disease,20 and cases of hepatocellular carcinoma in patients with cardiac cirrhosis have been reported.10,21 We therefore believe that it is essential to follow-up these lesions carefully and to consider targeted biopsy, interventional ablation or embolisation treatment especially for enlarging lesions.
We observed greater degrees of desaturation among patients with cirrhosis, consistent with greater degrees of venous collateralisation. This can be expected when the Fontan and portal venous pressure are relatively increased.22 We also noted significant gastro-oesophageal varices (the size of the descending aorta in one patient) in one third of patients. The established primary prophylactic option of variceal ligation or β-blocker treatment warrants further investigation to assess the efficacy in this patient group. Although we have not yet encountered any documented variceal bleeds, one patient with Fontan circulation under our care, not part of this series, had massive gastrointestinal haemorrhage and succumbed to this. The efficacy of intrahepatic portosystemic shunt creation in this group is questionable without further information on portal pressures and portosystemic gradients.
Patients with PLE in this cohort did not have liver injury worse than those without PLE. This would suggest that factors additional to hepatic fibrosis and portal hypertension may be at play in the pathogenesis of PLE.23–26 The high incidence of PLE in this population with Fontan circulation may be a reflection of compromised haemodynamics as all patients had been referred for Fontan conversion surgery.
Despite marked histological changes, markers of synthetic liver function such as INR and factor V were only slightly deranged and did not correlate with morphological changes observed. Low albumin levels were significantly associated with PLE, but not with the degree of morphological abnormality in the liver, or with other markers of impaired synthetic function. The Child–Turcotte–Pugh classification of severity of liver disease seems therefore less appropriate for the population with Fontan circulation. The lack of correlation between the original model-of-end-stage-liver-disease score and morphological findings reflects the relatively preserved INR, creatinine and bilirubin values in the group studied.27
Clinical implications and conclusions
Hepatic fibrosis and cirrhosis are common findings late in patients referred for Fontan conversion surgery. Despite the selective population studied, we believe that such changes are likely to be common in all patients late after the Fontan conversion, similar to patients with chronic congestion. Cardiac fibrosis and cirrhosis have been said to be reversible when the contributing causes are relieved.28 The creation and long-term maintenance of an interatrial communication may lower systemic venous pressures and improve cardiac output, both risk factors for liver injury.29 Conversion to total cavopulmonary anastomosis has also been shown to be associated with lower systemic venous pressures,5 and removes flow reversal in the hepatic vein during atrial systole.15 Vasodilator treatment has the potential to reduce the transhepatic and transpulmonary gradient. Recently, sildenafil (phosphodiesterase inhibitor type 5) and bosentan, the non-selective endothelin receptor blocker, have been shown to favourably modulate pulmonary vascular resistance, and in the context of the Fontan circulation, may improve transhepatic perfusion pressures. Their effects on hepatic vascular resistance are unknown.
We currently use the degree of cirrhosis—that is, as assessed clinically, radiologically and on histological—to assist in risk stratification of patients undergoing Fontan conversion surgery. Indeed, we have opted for an alternative—that is, non-conversion surgery—as a definite strategy in 2/12 patients on the basis of the extent of liver disease in combination with overall risk (table 2).
Characteristics of cirrhosis
We currently evaluate all patients with a longstanding Fontan circulation for gastro-oesophageal varices, hypervascular hepatic nodules, cirrhosis and gallstones using contrast CT and abdominal ultrasound. When hypervscular nodules are present, we monitor these carefully with 6-month serum α-fetoprotein levels and ultrasound, and consider MRI or repeat CT with or without lipidiol angiography and targeted biopsy for large or enlarging lesions, on the basis of the surveillance guidelines for high-risk patients of hepatocellular carcinoma published by the American Association for Study of Liver Diseases.30
Although we believe that patients with liver disease are likely to benefit from creation of a fenestration at the time of Fontan conversion, this needs prospective evaluation before a general recommendation can be made.
Limitations
This was a small, retrospective study, with all the incumbent limitations on statistical analyses. This meant that we were unable to perform multivariable regression analyses, and did not have sufficient power to assess a large number of potential risk factors for liver disease. The patient-reported alcohol consumption was not further substantiated, but was thought to be sufficiently reliable to be included in this study. The effect of varying medical treatment (including antiarrhythmics, ACE inhibitors and diuretics) in this small patient group is statistically uncertain. As this was not a prospective study, we did not routinely include direct measurement of cardiac output or pulmonary vascular resistance. Although coagulation data were only included when the INR had stabilised after stopping warfarin, a residual influence of the anticoagulation treatment cannot be excluded. We did not include more detailed serological tests of liver synthetic or secretory function. However, we believe it is important that conventional liver dysfunction markers in this population were not able to predict the severe underlying histological and morphological abnormalities.
Larger-scale investigations and longitudinal studies are necessary to confirm our findings, particularly in the non-failing patient.
REFERENCES
Footnotes
-
Published Online First 27 September 2006
-
Competing interests: None declared.
-
Informed consent was obtained for publication of the patients’ details in this report.