Article Text

Abstract
Objective: To verify whether optical coherence tomography (OCT) can accurately monitor the occurrence of arterial healing after stenting.
Setting: Delayed stent endothelialisation may predispose to stent thrombosis. OCT is a high-resolution intravascular imaging technique that accurately identifies stent struts and arterial tissues.
Design and interventions: Eight New Zealand white rabbits underwent the implantation of single bare metal stents (diameter 2–2.5 mm, length 8–13 mm) in the right common carotid artery through the external carotid artery. After a median of 11 days (range 2–28), the stented arteries were visualised by OCT, with images acquired at a pull-back speed of 0.5 mm/sec. The rabbits were then euthanised, vessels were formalin-fixed and finally processed for histopathology.
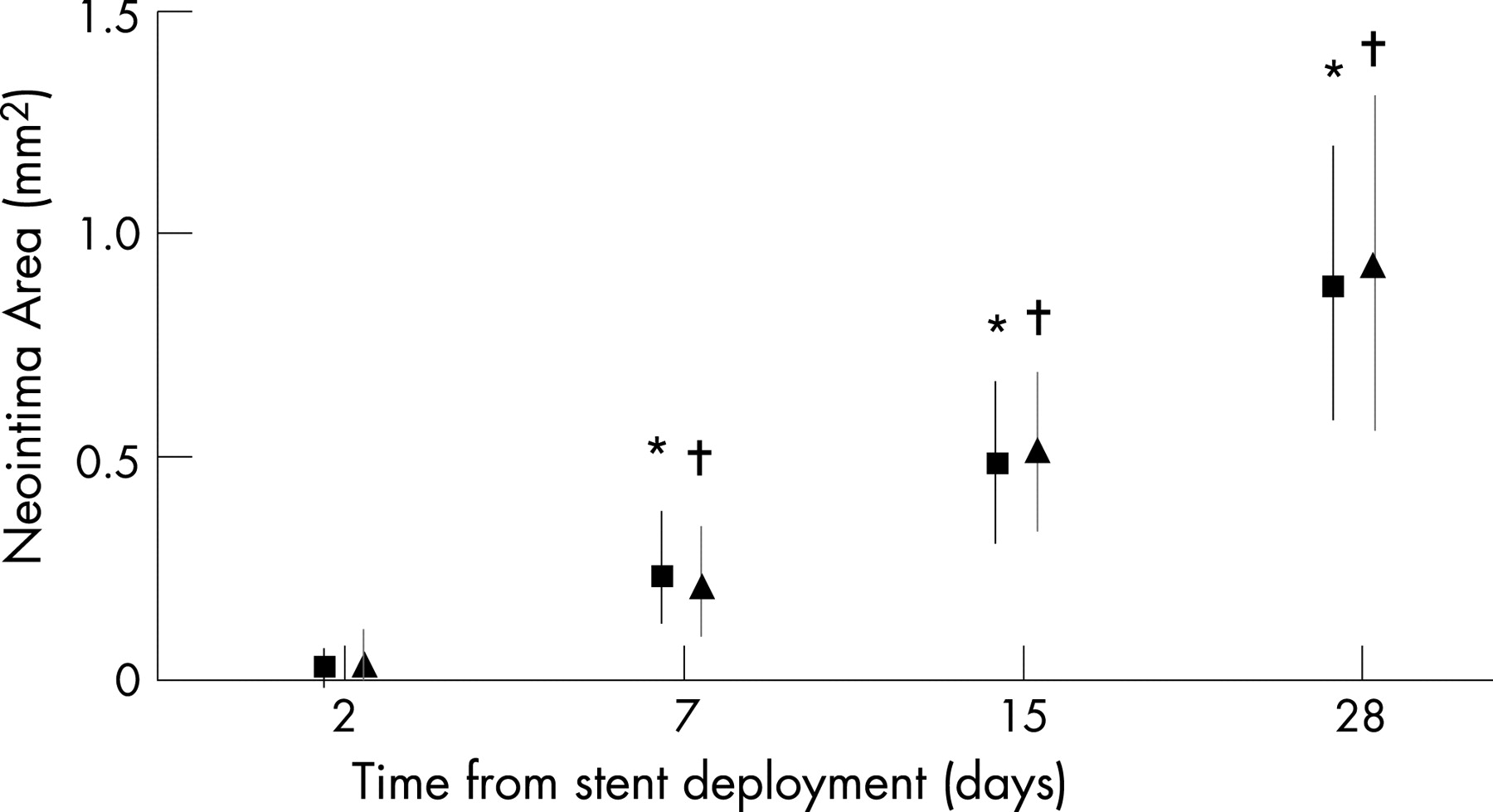
Results: We analysed 32 cross-sections from eight stented carotid arteries, for a total of 384 stent struts. OCT detected all of the stent struts in 30 of 32 cross-sections (93.7%), and correctly identified the presence/absence of tissue for every strut. Histological and OCT measurements of mean neointima thickness (0.135 (SD 0.079) mm and 0.145 (SD 0.085) mm, respectively, p = NS) were similar and closely related (r = 0.85, p<0.001). Neointima area progressively increased with longer time intervals from stent deployment to sacrifice; histological and OCT measurements were similar for each time interval.
The intra-observer and interobserver reproducibility of OCT neointima measurements were excellent (R2 = 0.90 and 0.88, respectively).
Conclusions: OCT is a promising means for monitoring stent strut coverage and vessel wall healing in vivo, the relevance of which will become even more significant with the increasing use of drug-eluting stents.
- stent
- angioplasty
- neointima hyperplasia
- optical coherence tomography
- histology
Statistics from Altmetric.com
Although infrequent, late stent thrombosis is a catastrophic event that leads to sudden death or major myocardial infarction in the majority of cases.1 After percutaneous coronary intervention (PCI) with stent implantation, an endothelialised smooth muscle cell-rich neointima seals the thrombogenic components in the underlying artery (metallic stent, lipid core, fibrin) from the lumen, providing protection against stent thrombosis. The lack of complete stent coverage is the most common pathological finding in case of stent thrombosis,2 the risk of which is heightened when the patient concomitantly discontinues double antiplatelet therapy.3 Currently, no in vivo imaging technique is able to provide reliable information on adequate strut coverage.
Optical Coherence Tomography (OCT) is an intravascular imaging technique that provides high image resolution (ca 10 μm),4 5 and, when used to assess stented arterial segments, may accurately differentiate stent struts and the vascular tissue surrounding them. OCT might thus be a valuable tool to assess appropriate healing of stented coronary segments and therefore guide pharmacological therapy to prevent late stent thrombosis. The aim of this histopathological study was to verify whether OCT can accurately monitor the occurrence of vessel wall healing.
METHODS
Study design
Ten New Zealand white male rabbits (Charles River, Calco, Italy), weighing 3.5–4.0 kg, singly housed, were used for the present study. The protocol was approved by the University of Chieti ethics committee. The investigation conforms to the Guide for the Care and Use of Laboratory Animals published by the US National Institutes of Health (NIH Publication NO. 85–23, revised 1996).
Animals were anaesthetised with ketamine (35 mg/kg), xylazine (5 mg/kg) and acepromazine (0.75 mg/kg), all administered intramuscularly. After surgical exposure of the right carotid artery, rabbits underwent the implantation of single bare metal Tsunami stents (Terumo, Japan) at 12 atm. in the common carotid artery through the external carotid artery. Stents had a nominal diameter of 2–2.5 mm, a length of 8–13 mm, an intended stent/artery ratio of 1.2:1 and a strut thickness of 0.18 mm.
Rabbits received aspirin 40 mg per os in combination with clopidogrel 75 mg daily per os starting 48 h before surgery. Therapy was continued until the animal was sacrificed. Before the intervention, rabbits were also given 100 IU of heparin per kilogram of body weight intravenously. One rabbit died during the deployment of the stent. One other rabbit died the day after, and here a carotid stent thrombosis was documented at autopsy. The remaining eight animals were the study population.
Rabbits were imaged in pairs by means of OCT after 2, 7, 15 and 28 days in order to study the different stages of vascular healing. They were then euthanised and their vessels processed for histopathology.
OCT
The carotid arteries were visualised using the M2 LightLab OCT system (LightLab Imaging, USA), which provides images at a longitudinal resolution of 15 μm and at variable frame rates up to 20 frames/s. Here, a setting of 4.1 frames/s was used to give better lateral resolution by increasing the number of radial A-lines per frame. The external carotid artery was first cannulated with a short modified 4-F multipurpose guiding catheter, which was gently placed in the distal segment of the common carotid artery, as previously described.6 After a 200 μg bolus of nitroglycerin, the 0.019-inch fibre optic imaging probe was advanced beyond the stent, in the proximal portion of the common carotid artery. OCT acquisition was then obtained with a wire pull-back at 0.5 mm/s and saline infusion was given through the guiding catheter, at a speed of 0.5–2 ml/sec, in order to transiently displace blood. Since the stent lengths were between 8 and 13 mm, the duration of the OCT pull-back ranged from 20 to 30 s. Finally, video sequences were stored on a CD in non-compressed AVI format.
Histology
Histological assessments were carried out with a previously validated methodology.7 After the follow-up stent imaging, rabbits were killed with an overdose of sodium pentobarbital, and the carotid specimens were fixed by immersion in formalin and embedded in methyl methacrylate. Four 2 mm sections were obtained from each stent (two from the middle, one from the proximal and one from the distal edge) with a tungsten carbide knife. Five-micrometre sections were cut on an automated microtome and subsequently stained with haematoxylin and eosin. Specimens were examined with a DMRAX2 photomicroscope (Leica-microsystems, Milan, Italy) and analysed with the Leica IM 500 image analysis software.
Correlation between OCT images and histopathology
All OCT analyses were performed at the Euro Imaging Laboratory, Rome, Italy. The OCT runs were qualitatively and quantitatively analysed by two experienced reviewers blinded to the histology results. Correlations of exactly corresponding OCT and histological images were performed using the stent edges as anatomical landmarks. All stent struts in each cross-section were numbered and evaluated for the presence of covering tissue. In cases where tissue was found, OCT was used to measure the thickness of neointimal hyperplasia. Intra-observer and interobserver variability were calculated for OCT assessments.
Statistical analysis
Data were analysed using the SPSS package (release 11.5, SPSS Inc., Chicago, Illinois). Continuous data were expressed as mean values (SD in brackets) and compared by means of Student t test or ANOVA for repeated measures; discrete variables were expressed as counts and percentages. Pearson’s correlation coefficient was computed to compare OCT and histopathological measurements of neointimal thickness, and Bland–Altman analysis was used to compare their agreement.8
Intra-observer and interobserver variability were assessed by means of a correlation analysis for continuous variables. A p value of <0.05 was considered statistically significant.
RESULTS
Stent architecture
Thirty-two cross-sections from eight stented carotid arteries were analysed using histopathology as the reference. OCT visualised 374 out of the 384 struts revealed at histology (97.4%), and correctly identified all stent struts in 30 of the 32 cross-sections (93.7%).
Estimates of tissue coverage
Tissue coverage was found in 12 out of the 32 cross-sections analysed by histology (37.5%) and 144 out of the 384 stent struts (37.5%). OCT correctly identified the presence/absence of tissue coverage in all cross-sections. Tissue coverage was similarly documented by histology and OCT in 0/94 (0%) struts 2 days after stent deployment, in 12/98 (12%) struts at 7 days, in 40/97 (41%) struts at 15 days, in 92/95 (97%) struts at 28 days (p for trend <0.001).
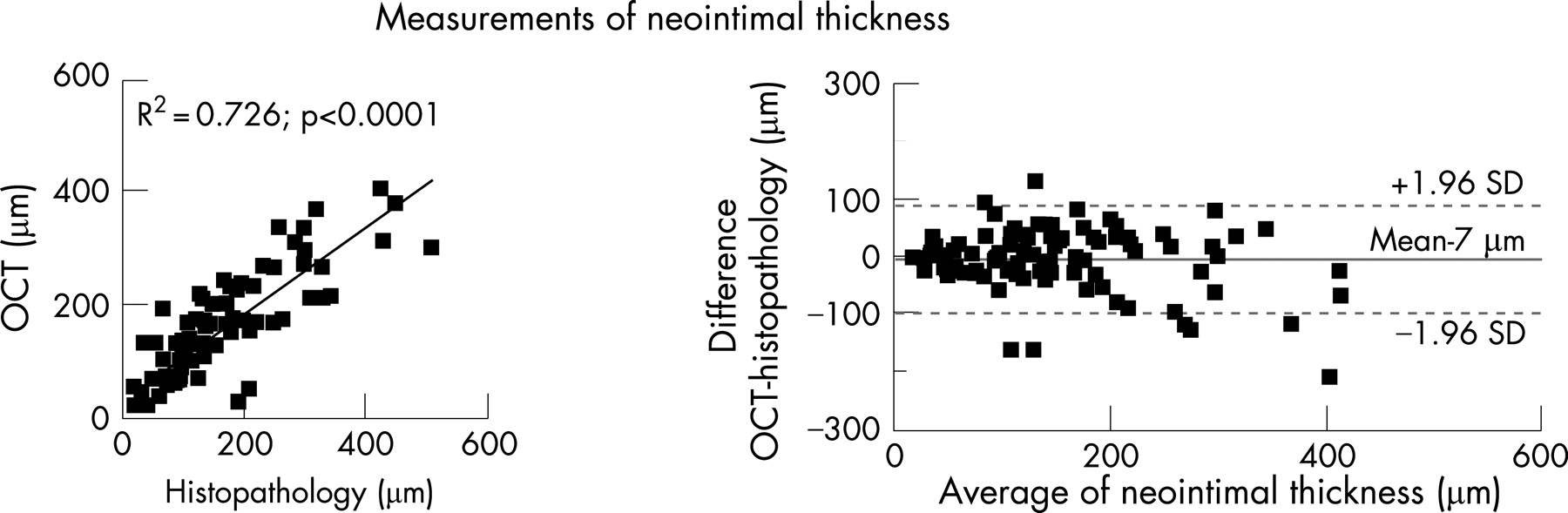
The mean neointima thickness measurements obtained by means of histology and OCT were very similar (0.13 (SD 0.079) mm and 0.145 (SD 0.085) mm, respectively, p = NS) and closely related (R2 = 0.726, p<0.001) at any range value (fig 1).

Stent area values were similar as measured by histology (3.56 (SD 0.31) mm2) and OCT (3.48 (SD 0.37) mm2, p = NS).
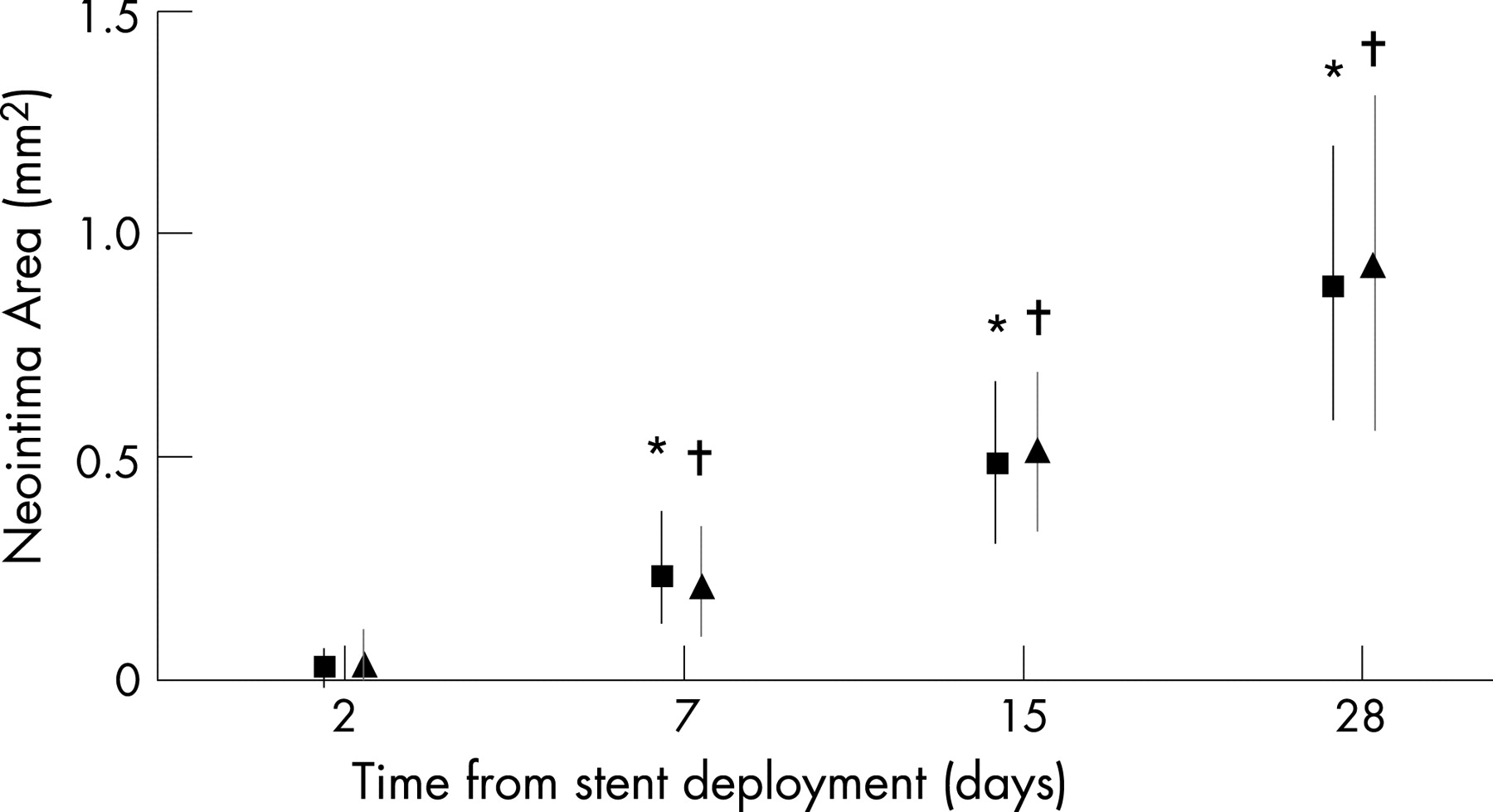
Neointima area progressively increased with longer time intervals from stent deployment to sacrifice; histological and OCT measurements were similar for each time interval (fig 2).
OCT measurements of neointima thickness were highly reproducible: the intra-observer and interobserver reproducibilities (R2) were 0.90 and 0.88, respectively. The minimum neointima thickness identified at histology was 0.025 mm. The relevant OCT measurement was 0.024 mm.
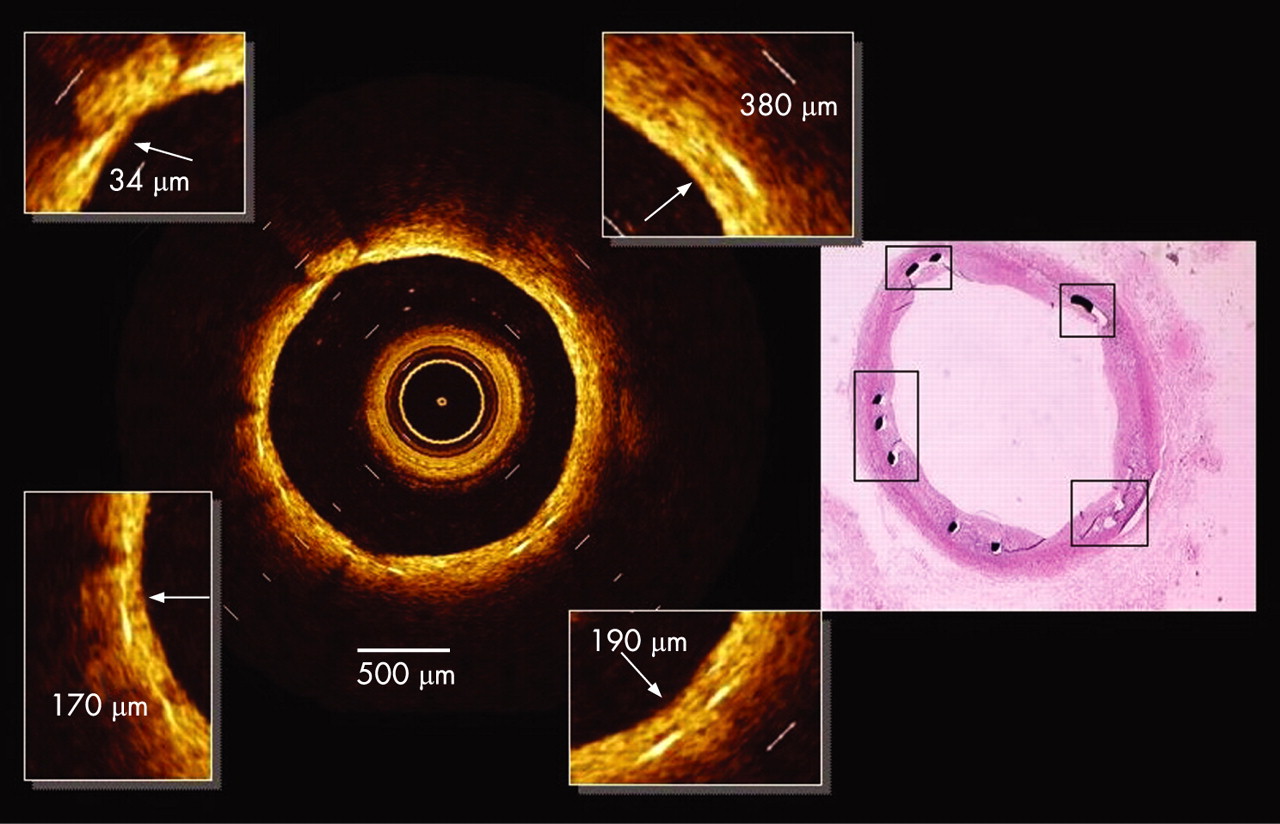
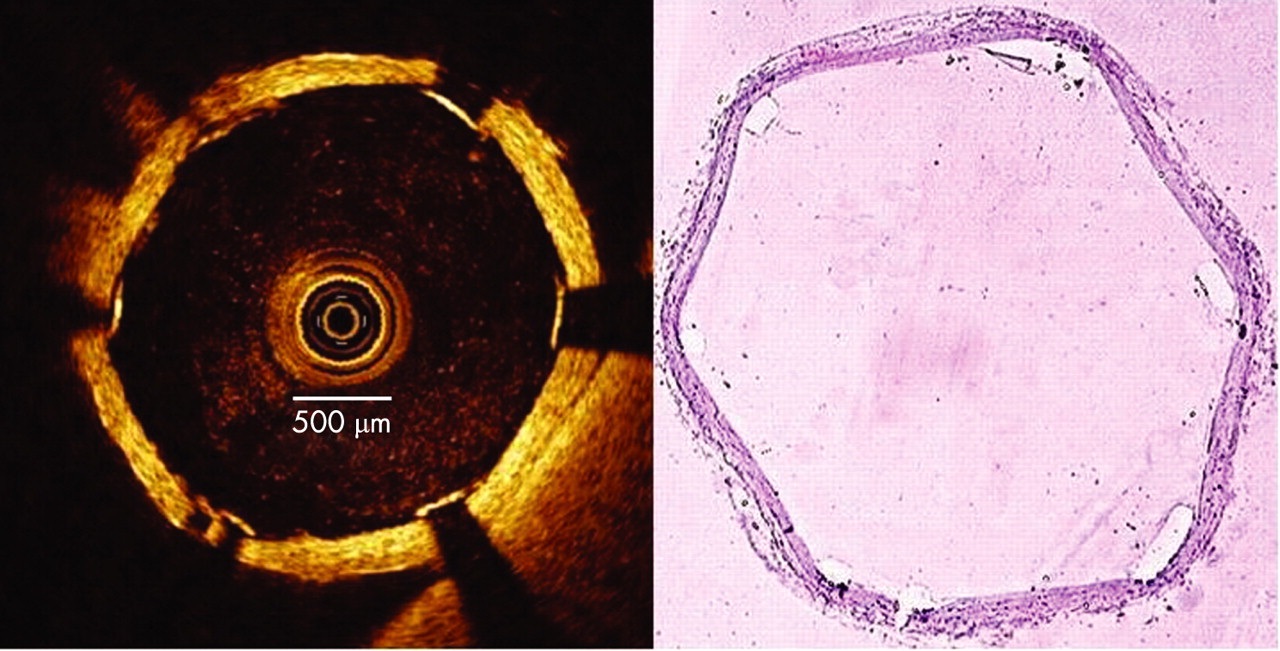
Examples of neointimal assessment by OCT and histology are shown in fig 3 and fig 4.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
DISCUSSION
The main finding of this study is that OCT provides an accurate assessment of vessel healing after stent deployment.
The typical OCT image in this study has an axial resolution of 15 μm and a lateral resolution of 25 μm, which is about 10 times higher than that of intravascular ultrasound (IVUS), the current standard of intravascular imaging. Intracoronary OCT finely visualises the microstructural features of advanced atherosclerotic lesions, as it allows an accurate quantification of lipid pools, and the measurement of fibrous cap thickness,4 5 which may be difficult to assess by IVUS.9 This unique resolution of OCT suggests that it may be well-suited for identifying vulnerable plaques in patients at risk.
More recently, OCT has been tested to monitor intracoronary stent deployment for both human and animal in vivo studies. In a consecutive series of 42 coronary stents imaged in 39 patients, tissue prolapse and incomplete stent apposition were identified more frequently with OCT than with IVUS.10 In a porcine coronary stent model lumen volumes calculated with both techniques were similar; however, stent volumes were significantly smaller with OCT than with IVUS, as OCT underestimated the stent strut thickness.11 More recently, OCT in one patient was shown to provide detailed visualisation of stent struts, neointimal proliferation, and even neovascularisation, which were missed by IVUS.12
Our findings with the present animal study extend previous knowledge, as we documented that OCT is accurate in the identification and quantification of tissue coverage of stent struts. This technique has therefore the potential to monitor vessel healing after stenting.
The current extensive use of drug-eluting stents has greatly reduced the incidence of in-stent restenosis even in the anatomical and clinical subsets of patients who are more prone to restenosis, but drug-eluting stents are also associated with late thrombosis, occurring even several months after stent implantation, and leading to adverse clinical events such as acute myocardial infarction and sudden death.1 3
Vessel healing after stenting occurs when the struts are covered by a layer of neointima and, eventually, endothelial cells.2 This tissue layer plays a pivotal role in preventing DES thrombosis, but is usually so thin that it cannot be visualised by angiography or IVUS (the resolution of the latter being in the range of 110–200 μm). In our study, OCT proved to be capable of detecting the presence/absence of neointima in all cases, including stent cross-sections with a covering neointima layer as thin as 20 μm; furthermore, the measurements were always reliable and reproducible.
OCT, therefore, has the potential to improve the clinical outcome after deployment of different types of drug-eluting stents. The technique can theoretically be used to assess the risk of stent thrombosis and guide clinical decisions on the duration of aggressive antiplatelet therapy for individual stent types and perhaps in the individual patient.
Current OCT resolution does not allow discrimination of cell types located in the superficial layers of neointima. Presumably in the near future technology developments in laser light source technology (which can bring axial resolution into the sub-5 μm range), and ongoing developments in data and image analysis, will enable the distinction between a new true intima layer and a pseudo-intima which has only fibroblast covering. This will further broaden our understanding of the vessel healing process after stent implantation.
Feasibility of OCT application
Unfortunately, at the current stage of technology, OCT is rather invasive. The manufacturer currently recommends for human use a gentle balloon inflation and vessel flushing with saline solution. The combined use of balloon inflation and vessel flushing clears the vessels of red blood cells and enables plaque visualisation. However, such a technique is cumbersome, and arterial occlusion may cause ischaemia and angina. In an animal setting, we are now using a continuous vessel flushing with saline in the external carotid arteries, but this cannot be applied in coronary arteries due to the arrhythmic effects of infusion.
Nevertheless, novel approaches that do not require balloon occlusion, currently being tested, are turning OCT into a more user-friendly technique. The adoption of intracoronary iso-osmolar solution through the guiding catheter to displace blood, which we are currently using in our cath lab, enables 30 mm-long pull-back and reduces patient discomfort. Also, introduction of new OCT platforms and optical probes, having a higher frame rate and acquisition speed, will further improve the length of analysed segments. These novel approaches will likely make OCT a technique well-suited to evaluate the risk of stent thrombosis.
OCT from bench to bedside
Our results show that OCT is capable of accurately monitoring vessel healing after stent placement. The assessment of an incomplete stent strut coverage may be extremely relevant in case of DES implantation.
OCT may therefore be used to acquire precise assessments of in-stent neointimal thickness in animal studies, and has a number of advantages over histology. It can be performed in vivo, is repeatable and allows the direct quantification of neointima at different stages after intervention; theoretically, it may even be more accurate than histology, for which cutting may cause stent distortion and tissue displacement; and it enables almost continuous visualisation of cross-sectional neointima (in this study, every 0.5 mm), whereas histology is limited by the number of cuts.
Limitations
We acknowledge that a limited number of animals were studied. Had we analysed by OCT a larger number of rabbits at each data point the current study would have enabled additional insight on the time course of vessel healing, by serially measuring in-stent neointima in the same animal. Our paper is intended to describe the ability of OCT to identify a specific anatomical aspect of the vessel wall. We did not account for animal variability because we did not perform a treatment versus control study. However, despite the limited number of animals studied, the statistical design of the current study enabled the achievement of solid conclusions on the capability of OCT to detect vessel healing after stenting.
Circumferential orientation of sections may limit the evaluation of OCT accuracy; in order to circumvent the problem, we adopted an established technique, which we had used in the past to validate IVUS cross-section images of coronary arteries13; after matching of the corresponding OCT and histology cross-sections of common carotid arteries, the geometry of the lumen and position of the struts enabled a precise circumferential orientation of cross-sections.
CONCLUSIONS
OCT is a promising technique for the accurate in vivo monitoring of stent strut tissue coverage and vessel wall healing, whose relevance will become increasingly significant in the forthcoming DES-oriented PCI era.
Acknowledgments
We thank Dr Christopher Petersen of LightLab Imaging for his assistance in the technical aspects of OCT.
REFERENCES
Footnotes
Competing interests: None.