Article Text

Abstract
Objective: The purpose of the study was to evaluate the prevalence of CAD as well as plaque morphology in asymptomatic patients with type 2 diabetes using multi-slice computed tomography (MSCT). In addition, the relation between calcium score and MSCT findings was explored.
Design: In 70 patients, coronary calcium scoring and non-invasive coronary angiography were performed. Angiograms showing atherosclerosis were further classified as obstructive (⩾50% luminal narrowing) CAD or not. Plaque type (non-calcified, mixed and calcified) was determined. Finally, the relation between calcium score and MSCT findings was explored.
Results: A calcium score <10 was observed in 31 (44%) patients. A calcium score of 10–100 was observed in 14 (20%) patients while a score of 101–400 or >400 was identified in 12 (17%) and 13 (19%) patients respectively. Non-invasive coronary angiography showed CAD in 56 (80%) patients. 322 coronary segments with plaque were identified, of which 132 (41%) contained non-calcified plaques, 65 (20%) mixed plaques and 125 (39%) calcified plaques. The percentage of patients with obstructive CAD paralleled increasing calcium score. The presence of CAD was noted in 17 (55%) patients with no or minimal calcium (score <10).
Conclusions: MSCT angiography detected a high prevalence of CAD in asymptomatic patients with type 2 diabetes. A relatively high proportion of plaques were non-calcified (41%). Importantly, a calcium score <10 did not exclude CAD in these patients. MSCT might be a useful technique to identify CAD in asymptomatic patients with type 2 diabetes with incremental value over calcium scoring.
- coronary artery disease
- type 2 diabetes mellitus
Statistics from Altmetric.com
Diabetes mellitus has reached epidemic proportions and has become a major public health problem. Almost 200 million individuals are known to have diabetes and this number is expected to increase exponentionally. In the USA almost 1.3 million new subjects are diagnosed with diabetes each year.1
Cardiovascular complications, including coronary artery disease (CAD), are the leading causes of morbidity and mortality in individuals with type 2 diabetes mellitus.2 The overall prevalence of CAD has been reported to be as high as 60% in patients with diabetes referred for stress testing.3 The 10-year mortality in patients with known CAD and diabetes exceeds 70%.4 The poor clinical outcome in patients with diabetes underscores the need to develop practical approaches for detecting CAD at an early stage. Moreover, in patients with diabetes mellitus, CAD has frequently progressed to an advanced state before it becomes clinically manifest.5 6
The role of single photon emission computed tomography (SPECT) in asymptomatic patients with diabetes has recently been evaluated. The Detection of Silent Myocardial Ischemia in Asymptomatic Diabetics (DIAD) study is an ongoing randomised study using gated SPECT for risk stratification in asymptomatic patients with diabetes type 2. In 22% of patients (silent) myocardial ischaemia was noted, with 16% showing abnormal perfusion on SPECT.7
Recently, multi-slice computed tomography (MSCT) has been proposed as an alternative imaging modality for the evaluation of patients with known or suspected CAD.8 MSCT allows anatomical, non-invasive imaging of the coronary arteries, including detection of coronary atherosclerosis by assessing the coronary artery calcium burden (calcium scoring) and by performing non-invasive angiography. This technique has the potential to detect CAD at an early stage. With the recently introduced 64-slice MSCT, high sensitivity and specificity for the detection of significant (⩾50% luminal narrowing) stenoses have been reported and this technique has been validated against conventional coronary angiography and intravascular ultrasound.9–14
The purpose of this study was to evaluate the prevalence of CAD in a large cohort of asymptomatic type 2 diabetic patients using MSCT angiography. The plaque constitution of the coronary artery lesions was also evaluated, and the relation between calcium scoring and non-invasive angiography was explored.
DESIGN
Patients
Seventy-three asymptomatic patients with type 2 diabetes mellitus were included. All patients were referred from an outpatient diabetic clinic to our institution for assessment of cardiovascular risk. Inclusion criteria consisted of type 2 diabetes mellitus, no angina or angina-equivalent symptoms. Exclusion criteria were: known or suspected CAD; history of coronary revascularisation; treatment with anti-anginal medication; ventricular and supraventricular arrhythmias; contraindications for the use of iodinated contrast media.
Patients were excluded from analysis when an irregular heart rate during MSCT data acquisition rendered the MSCT data set uninterpretable.
Asymptomatic status was confirmed using the Rose questionnaire for angina.15
The study was part of a clinical study for patients referred to the MSCT for which clinical approval was obtained.
MSCT, data acquisition
Imaging was performed using a 64-slice MSCT scanner (Aquilion 64, Toshiba Medical Systems, Japan). If the heart rate was ⩾65 beats/min, additional oral β-blockers (metoprolol 50 mg, single dose, 1 h before scan) were provided when tolerated.
First, a prospectively triggered coronary calcium scan was performed before MSCT angiography. Accordingly, data were acquired with a collimation of 64×0.5 mm and a tube rotation time of 400 ms, and tube current of 300 mA at 120 kV for patients with normal posture (BMI<30 kg/m2). In case of patients with higher body mass indexes (>30), tube current was increased to 350 or 400 mA at 135 kV. The temporal window was set at 75% after the R-wave for electrocardiographically triggered prospective reconstruction. 80 to 110 ml non-ionic contrast material, depending on the total scan time, was administered with a flow rate of 5 ml/sec (Iomeron 400®, Bracco Atlanta Pharma, Konstanz, Germany). Automated detection of peak enhancement in the aortic root was used for timing of the scan. All images were acquired during an inspiratory breath hold of approximately 10 s, with simultaneous registration of the patient’s electrocardiogram. Subsequently, data sets were reconstructed and transferred to a remote workstation as previously described.16 Briefly, images were initially reconstructed at 75% of the cardiac cycle. In case of motion artefacts, a representative single slice was reconstructed throughout the cardiac cycle in steps of 20 ms to determine the most optimal additional reconstruction phases.
MSCT, data analysis
Coronary artery calcium score
The coronary artery calcium score was assessed with the application of dedicated software (Vitrea 2, Vital Images, USA). Coronary artery calcium was identified as a dense area in the coronary artery exceeding the threshold of 130 HU. An overall Agaston score was recorded for each patient.
Coronary plaque assessment
All angiograms were evaluated by two experienced observers (JWJ, JS) unaware of the clinical history of the patients. In case of disagreement, a joint reading was performed and a consensus decision was reached. Coronary arteries were divided into 17 segments according to the modified American Heart Association classification.17 Only segments with a diameter >1.5 mm (as measured on the MSCT coronary angiogram) were included. First, each segment was classified as interpretable or not. Then, the interpretable segments were evaluated for the presence of any atherosclerotic plaque using axial images and curved multiplanar reconstructions. Coronary plaques were defined as structures >1 mm2 within and/or adjacent to the coronary artery lumen, which could be clearly distinguished from the vessel lumen and the surrounding pericardial tissue, as described previously.18
As adequate distinction between a single lesion and the presence of diffuse atherosclerosis extending over several segments may be difficult in some cases, it was chosen to perform the analysis on a segmental basis, also in order to improve reproducibility of the results. One coronary plaque was assigned per segment. Subsequently, the type of plaque was determined using the following classification: 1) non-calcified plaques, plaques having lower density compared with the contrast-enhanced vessel lumen; 2) calcified plaques, plaques with high density; and 3) mixed plaques, plaques with non-calcified and calcified elements within a single plaque. Finally, it was determined whether the lesion was obstructive or not, using a threshold of 50% luminal narrowing. For each patient the number of diseased vessels and number of each type of plaque were determined. Patients without plaques were considered normal; an abnormal MSCT was defined in the presence of ⩾1 coronary plaque.
Statistical analysis
Continuous variables were expressed as mean and standard deviation. Proportions were expressed in percentages. Statistical analysis was performed using SPSS 12.0 software.
RESULTS
Patient characteristics
In total 73 patients were referred from the outpatient diabetic clinic and enrolled in the present study. Three patients (4%) were excluded from the analysis because of an irregular heart rate during MSCT data acquisition, which rendered the MSCT data set uninterpretable. Baseline characteristics of the 70 analysed patients are provided in table 1. The majority of the patients were male (74%). The mean duration of diabetes was 110 (SD 88) months.
MSCT
Coronary artery calcium score
As shown in fig 1, coronary calcium was absent or the calcium score was less than 10 in 31 (44%) patients. A calcium score of 10–100 was observed in 14 (20%) patients, a score of 101–400 in 12 (17%) patients, and 13 (19%) patients had a calcium score >400.

Coronary angiography
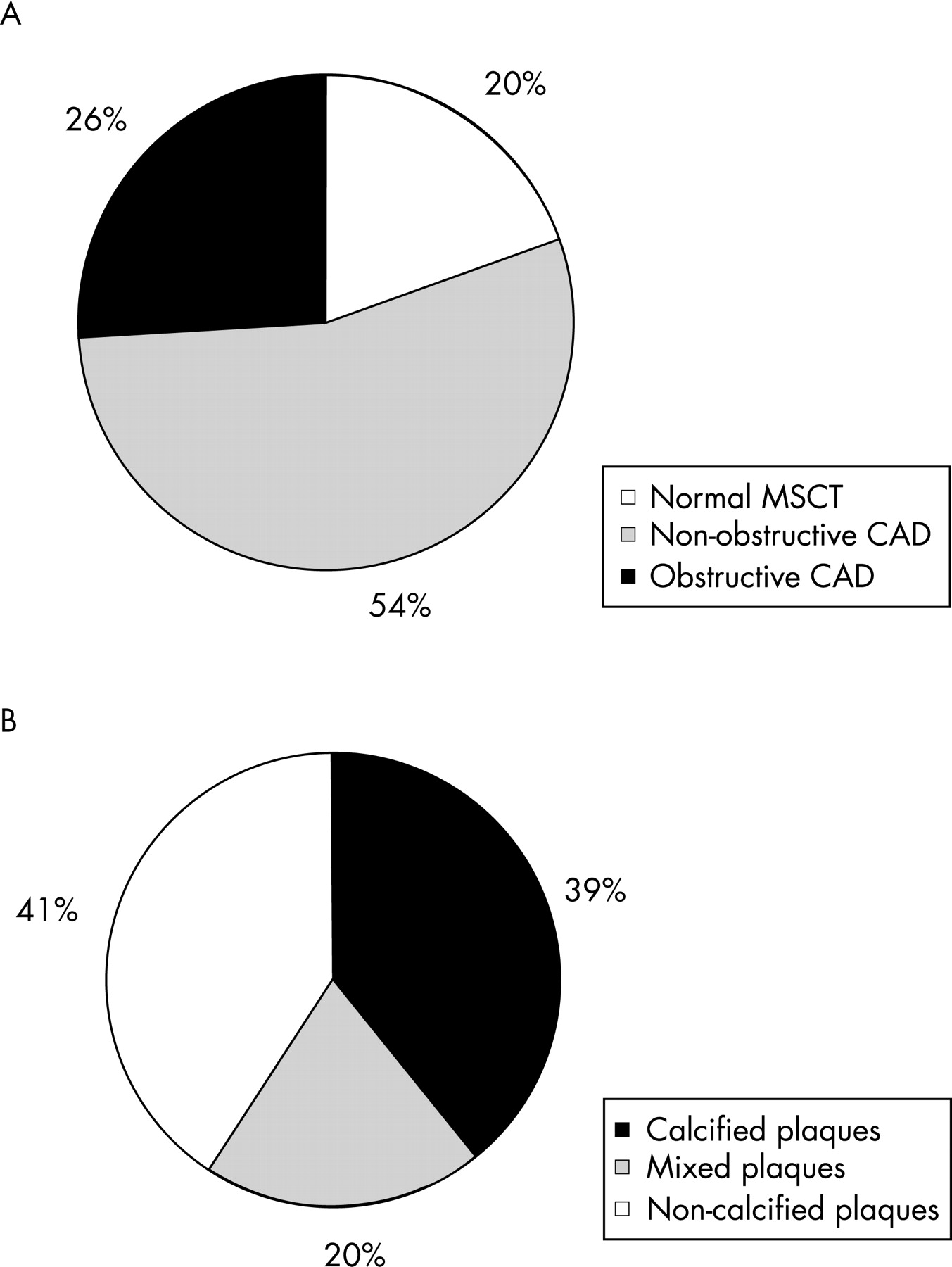
MSCT identified 14 (20%) patients without CAD and 56 (80%) patients with CAD.
A total of 38 (54%) patients had non-obstructive CAD, and 18 (26%) patients had obstructive CAD (at least one significant (⩾50%) stenosis) (see fig 2). In the 38 patients with non-obstructive CAD, 10 (26%), 8 (21%) and 20 (53%) had 1-vessel, 2-vessel and 3-vessel disease, respectively. Regarding the 18 patients with obstructive CAD, one, two and three vessels were significantly diseased in no (0%), 4 (72%) and 14 (78%) patients.

Plaque morphology
A total of 15 (1.3%) of 1190 coronary segments were not interpretable due to motion artefacts. In the 56 patients with CAD, 322 coronary segments with plaques were observed.
Fifty-nine (18%) plaques were obstructive and 263 (82%) plaques were non-obstructive. One hundred and thirty-two (41%) contained non-calcified plaques, 65 (20%) mixed plaques and 125 (39%) calcified plaques, as illustrated in figure 2B.
Coronary calcium score versus coronary angiography
Comparison of the coronary artery calcium score and MSCT angiography showed that the percentage of patients with obstructive CAD paralleled the increasing calcium score; increasing from 10% in patients with minimal calcium (score <10) to 54% in patients with calcium score >400 (fig 3). Still, in patients with minimal calcium (score <10), the presence of CAD was detected on non-invasive coronary angiography in 55% (n = 17) of the patients. In these patients, CAD was non-obstructive in 82% (n = 14) and obstructive in 18% (n = 3) patients.

DISCUSSION
The main findings of this study can be summarised as follows. First, MSCT could detect CAD in 80% of asymptomatic patients with type 2 diabetes. In addition, in 56% of patients an elevated calcium score (>10) was observed. Although most patients presented with non-obstructive CAD, in 26% of the patients at least one significant coronary artery stenosis was detected. Furthermore, in the majority of patients with non-obstructive CAD, diffuse disease was noted involving the entire coronary tree.
Second, coronary plaque composition was explored and revealed a relatively high proportion of non-calcified (41%) plaques.
Finally, the relation between the coronary calcium score and CAD on non-invasive angiography was evaluated. In line with the high prevalence of non-calcified plaques, considerable atherosclerosis was noted in patients without (or with minimal) coronary artery calcium. These findings suggest that non-invasive angiography with MSCT may provide additional information to calcium scoring for detection of CAD.
Prevalence of CAD
In diabetic patients, the diagnosis of CAD is frequently missed or delayed since the typical symptoms of myocardial ischaemia are often masked. Before symptoms of ischaemia occur, diffuse multi-vessel atherosclerosis is often present. It has been shown that risk and mortality from CAD in patients with type 2 diabetes are similar to those in patients without diabetes, but with previous myocardial infarction.4 Moreover, the combination of CAD and diabetes strongly increases adverse outcome and underscores the need to develop practical approaches for detecting CAD at an early stage before clinical complications have occurred. This approach may permit prevention of complications and reduce morbidity and mortality in these patients.
Two recent studies used nuclear imaging with SPECT and showed a prevalence of (silent) myocardial ischaemia ranging from 18% to 21% in truly asymptomatic patients with type 2 diabetes.7 19 However, SPECT reflects the presence of CAD only indirectly, since it is based on the detection of coronary lesions that result in compromised blood flow during stress, whereas the actual prevalence of any atherosclerosis in asymptomatic patients with diabetes mellitus may be higher. Indeed, in the current study with MSCT, CAD was observed in 80% of asymptomatic patients with type 2 diabetes mellitus. Furthermore, the majority of patients showed diffuse involvement of all three coronary arteries. The high prevalence of coronary atherosclerosis among diabetic patients without clinical CAD has been defined previously in a large autopsy cohort of 293 decedents.20 In line with the current observations, coronary atherosclerosis was observed in almost 75% of individuals, with 50% having diffuse multi-vessel CAD.
Non-invasively, calcium scoring has been proposed to determine the prevalence of atherosclerosis. Previous studies in the general population have demonstrated that the extent of coronary artery calcium strongly correlates with the overall magnitude of atherosclerotic plaque burden and subsequent risk of coronary events.21–23
In the current study, coronary calcifications (calcium score >10) were observed in 56% of patients. Moreover, extensive calcifications were observed in 19% of patients. These observations are in line with previous investigations.24 25
Plaque morphology
In addition to the presence of (significant) CAD, plaque characteristics were also assessed in the current study. Analysis of the relative proportion of non-obstructive and obstructive plaques revealed that plaques were mainly non-obstructive (82%). A similar relation between diabetes and non-obstructive plaques has been shown in studies using invasive coronary angiography.26 It is important to realise that many of these non-obstructive lesions will not be associated with stress-inducible ischaemia, thus showing normal perfusion during stress nuclear imaging. Nonetheless, it has been suggested that plaque rupture may occur frequently in non-obstructive plaques24–27 and detection of an increased non-obstructive plaque burden using atherosclerosis imaging may therefore be of clinical importance in asymptomatic patients with diabetes.
With regard to plaque constitution, 41% of the plaques were classified as non-calcified plaques, 20% as mixed and 39% as calcified plaques. Recently, Mollet et al reported on plaque constitution in patients with stable CAD using MSCT. In this population, plaques were non-calcified in 24%, while the vast majority of lesions (65%) were calcified.23 Accordingly, asymptomatic diabetic patients appear to have a higher prevalence of non-calcified plaques, which are mainly non-obstructive. These findings are of clinical importance, since these plaques may be vulnerable to rupture and may be related to the high cardiovascular mortality and morbidity in diabetic patients. Indeed, in a large study by Raggi et al involving 903 asymptomatic diabetic patients, similar event rates were observed at a lower calcium score than in non-diabetic patients, suggesting that non-calcified plaques may (to some extent) determine the event rate in diabetic patients.22
Value of calcium scoring versus non-invasive angiography to detect CAD
In a next step, the relationship between calcium score and the extent of CAD on MSCT was investigated. The prevalence of obstructive CAD paralleled the increasing calcium score, with 54% of patients with a calcium score >400 having at least one significant stenosis. Nevertheless, a calcium score <10 was associated with normal coronary arteries on MSCT in only 45% of patients, whereas 55% of patients still had (non-calcified) atherosclerosis. These findings underscore the additional value of non-invasive angiography to calcium scoring for assessment of CAD using MSCT.
Clinical implications
Identification of CAD in asymptomatic patients with type 2 diabetes can be of clinical relevance since clinical outcome may considerably improve if aggressive medical therapy is initiated at an early stage. Screening of asymptomatic diabetic patients, however, is a heavily debated topic.27 28 Recently, calcium scoring has been suggested as a first screening tool for CAD in asymptomatic diabetic patients.19 Recent findings, however, indicate that non-calcified atherosclerotic plaques are frequently present, in the absence of coronary artery calcium. Whether screening of asymptomatic patients is useful, and whether calcium scoring with or without MSCT angiography has a role in this process, needs to be addressed in large future studies.
LIMITATIONS
Several limitations should be mentioned. First, only a limited number of patients were studied and data concerning the prevalence of atherosclerosis as determined by MSCT in larger populations are needed. Also, despite the excellent diagnostic accuracy of MSCT, uninterpretable segments due to motion artefacts remain problematic. In the current study, three (4%) patients were excluded from analysis for this reason. Finally, the radiation burden (10–15 mSv) of MSCT remains a drawback of this imaging modality. However, a reduction in radiation burden is anticipated with the new generation of 256-slice MSCT scanners and dose-modulation strategies that are currently being developed.
CONCLUSIONS
MSCT angiography detected a high prevalence of CAD in asymptomatic patients with type 2 diabetes. A relatively high proportion of plaques were non-calcified (41%) and calcified (39%). Accordingly, a calcium score <10 did not exclude CAD in this particular cohort of patients and appeared of limited value. MSCT angiography may provide additional information over calcium scoring in asymptomatic patients with type 2 diabetes.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Acknowledgments
The study is supported by an unrestricted grant from BMS Medical Imaging.
REFERENCES
Footnotes
Competing interests: None declared.