Article Text

Abstract
The use of positron emission tomography (PET) in cardiology is growing rapidly. Technical features make PET a strong technology for the non-invasive evaluation of cardiac physiology. It is currently considered the most reliable tool for the identification of myocardial viability and also allows accurate assessment of myocardial perfusion and detection of coronary artery disease (CAD). The unique feature of PET is that myocardial perfusion can be measured in absolute terms, improving sensitivity in the detection of multivessel of disease and also allowing evaluation of very early changes in coronary vasoreactivity and the progression or regression of CAD. Use of the newest generation of PET systems with integrated multislice computed tomography (CT) is becoming a standard technique for cardiac imaging. Since the PET and CT techniques ideally complement each other the combination is particularly attractive for the non-invasive assessment of CAD but also has other functions. Finally, there are also promising future applications that involve molecular imaging of cardiac targets, which may further enhance the clinical utility of PET and hybrid imaging.
Statistics from Altmetric.com
Positron emission tomography (PET) represents highly advanced scintigraphic imaging technology. It allows non-invasive functional assessment of myocardial perfusion, substrate metabolism and cardiac innervation and receptors as well as gene expression in vivo and it has contributed significantly to advance our understanding of heart physiology and pathophysiology. Recent technical development and increased availability of the technique have facilitated the use of PET in clinical cardiology also.
Evaluation of the utilisation of myocardial glucose with [18F]fluorodeoxyglucose (FDG) and PET is currently considered the most reliable tool for the identification of myocardial viability. PET also allows accurate assessment of myocardial perfusion and detection of coronary artery disease (CAD).1 The unique feature of PET is that absolute measurements of myocardial perfusion can be made and this improves sensitivity in the detection of multivessel disease and also allows evaluation of very early changes in coronary vasoreactivity and the progression or regression of CAD.
Two years ago hybrid imaging systems with multidetector computed tomography and PET were introduced. This combination is powerful in the assessment of coronary heart disease and has the potential to become the major technique in cardiac imaging.2 In addition, new molecular imaging probes for PET are rapidly developing. The methods for atherosclerotic plaque characterisation, imaging of stem cells and gene therapy are approaching the clinical phase.
DEVELOPMENT OF PET TECHNOLOGY
The PET scanner technique was developed in 1970s but during the following two decades it was used only as a research tool.3 4 In the mid-nineties, the new scanner generation was specifically developed for clinical use with whole body imaging protocols and easy image visualisation tools. Wider clinical use especially in oncology increased very rapidly. In 2000 the first hybrid scanners were introduced and this revolutionised PET imaging in oncology. Very rapidly PET-CT studies became the standard technique in staging and monitoring of cancer.
This led to rapid expansion in the availability of PET scanners in clinics, and interest in clinical cardiac use increased. However, the availability of suitable tracers and processing software was still limiting the wider use of the technique as a routine method in cardiac patients.
During recent years several critical limitations for clinical cardiac PET have been overcome.1 PET scanners with 64-slice CT makes it possible to perform very rapid imaging protocols (<30 minutes) that combine CT coronary angiography and perfusion PET. The availability of PET perfusion tracers was improved by distribution of rubidium-82 (82Rb) generators. Development of clinical software for quantitative analysis of myocardial perfusion became available. In addition, in the near future, new perfusion tracers with improved characteristics will enter clinical use.
CURRENT PET TECHNOLOGY
Several technical features make PET a strong technology for the non-invasive evaluation of cardiac physiology. The sensitivity and contrast resolution of PET are exceptionally high. The spatial resolution is high enough for cardiac imaging and independent of depth. The temporal resolution (in the order of seconds) is high enough to enable imaging of physiological and metabolic processes. Finally, these processes can be measured in absolute quantitative units.3–5
PET tracers
PET imaging is based on tracers that are labelled with positron-emitting radionuclides.5 The PET scanner itself is only visualising the spatial and temporal distribution of the tracer. Thus, the physiological signal is completely dependent on the characteristics of the tracer that has been labelled. This character provides unique versatility but since these tracers have typically very short half-life and are not widely commercially available, the tracer availability is the major determinant of the usage of PET.
In the centres with radiotracer production facility, several tracers have been used. The most commonly used metabolic tracer has been FDG, which enables measurement of myocardial glucose utilisation and assessment of myocardial viability.6 7 The availability of FDG is currently very good owing to its routine use in oncology. In addition to FDG, there are many other metabolic tracers that have clinical potential, such as [11C]acetate, which allows robust non-invasive measurement of myocardial oxygen consumption in the left and right ventricles.8 9 This provides the means to estimate the oxygen cost of contractility, the efficiency of myocardial forward work—the measure that seems to have clinical potential, especially in patients with heart failure.
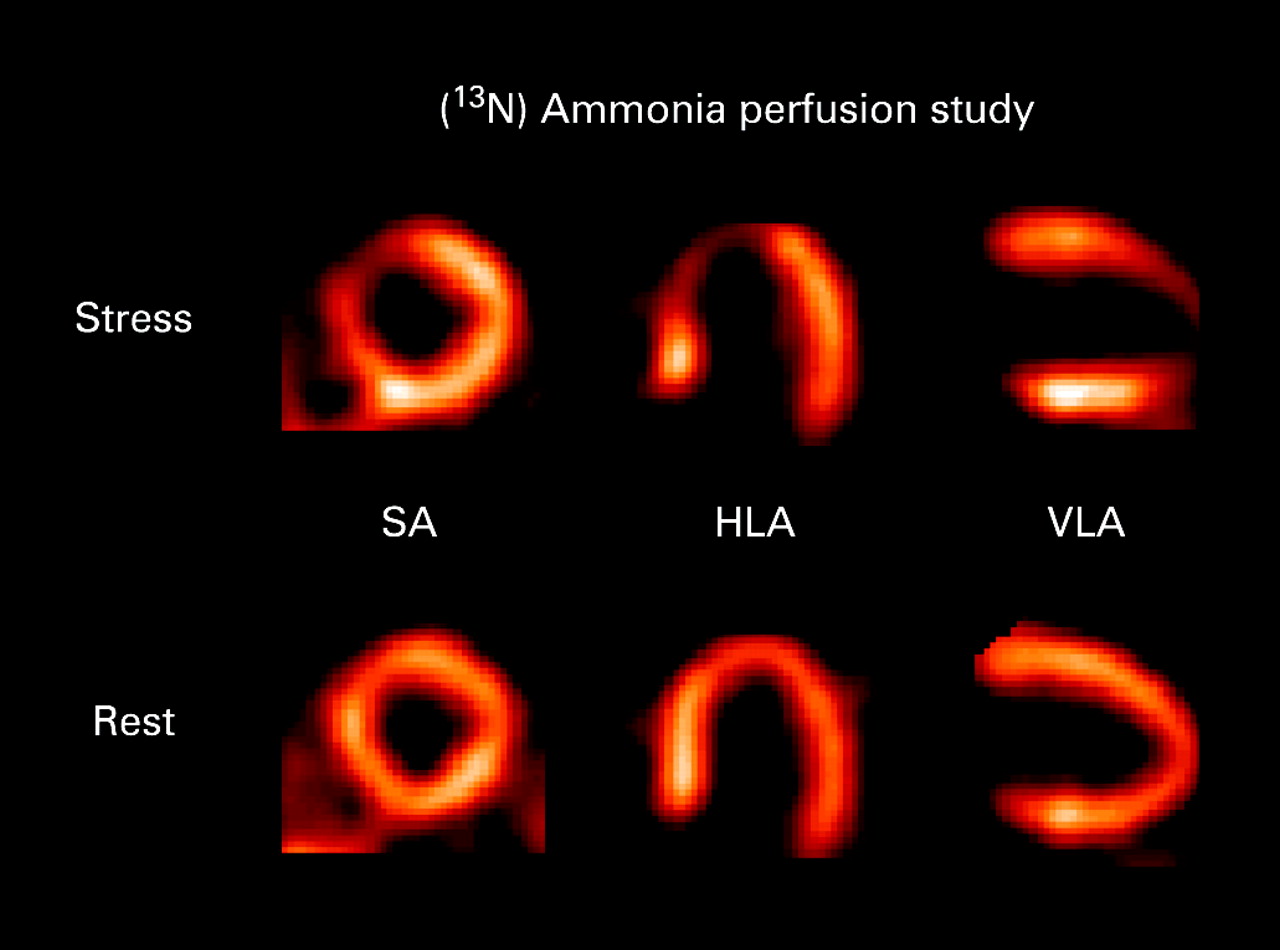
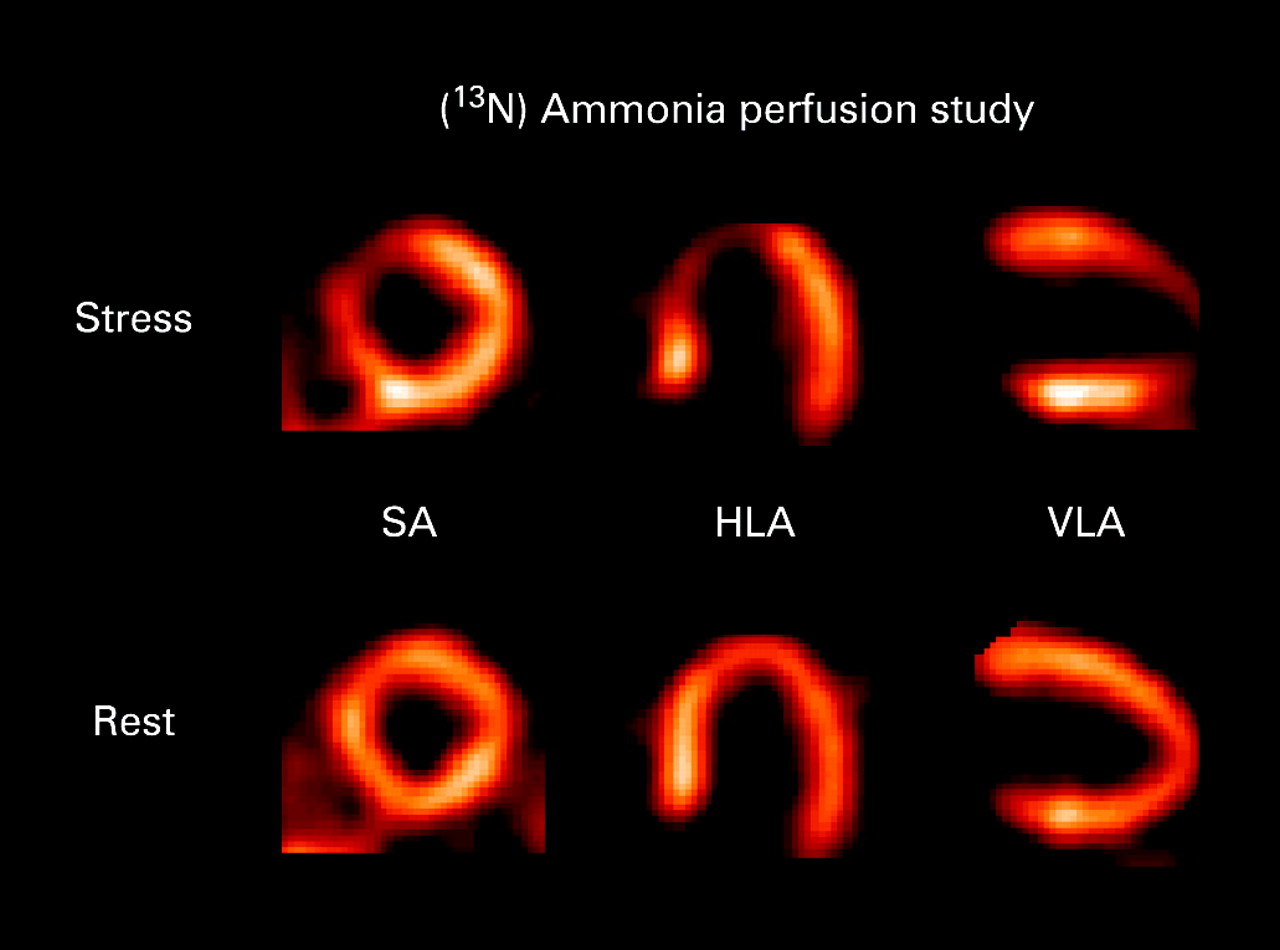
PET is a validated and highly reproducible method of providing regional measurement of myocardial blood flow at a microcirculatory level under rest and stress conditions.10–13 The three main tracers used in the imaging of perfusion are 15O-labelled water, 13N-labelled ammonia and the generator-produced 82Rb. Each of these tracers has specific advantages and limitations.5 10–12
The use of [13N]ammonia results in good quality images (fig 1) owing to high myocardial retention and rapid clearance of the tracer from the blood pool. Blood flow can be measured over a wide blood flow range.10 The application of [13N]ammonia provides today robust and reliable means for the regional measurement of blood flow not only under resting conditions, but also after various pharmacological interventions.
[15O]Water is the most physiological tracer currently available.11 The advantage of [15O]water in comparison with [13N]ammonia is the short physical half-life, which allows repetitive measurements within short time intervals and is, therefore, ideally suited for pharmacological intervention studies. Until recently, the difficult image processing and analysis have limited its use in patients with more advanced CAD. However, with the newest generation of scanners and analysis software, the use of [15O]water in clinical settings has become feasible (fig 2).

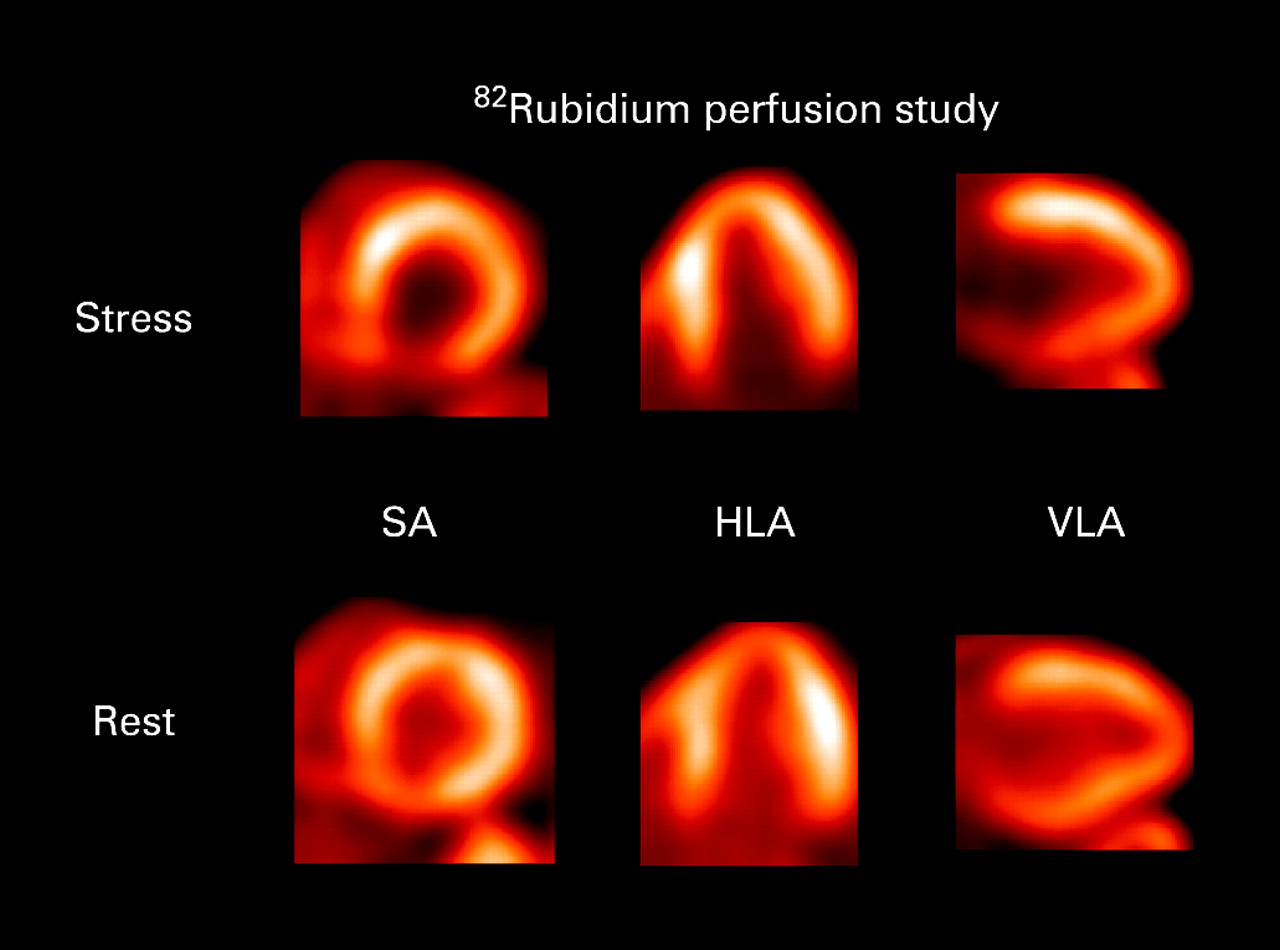
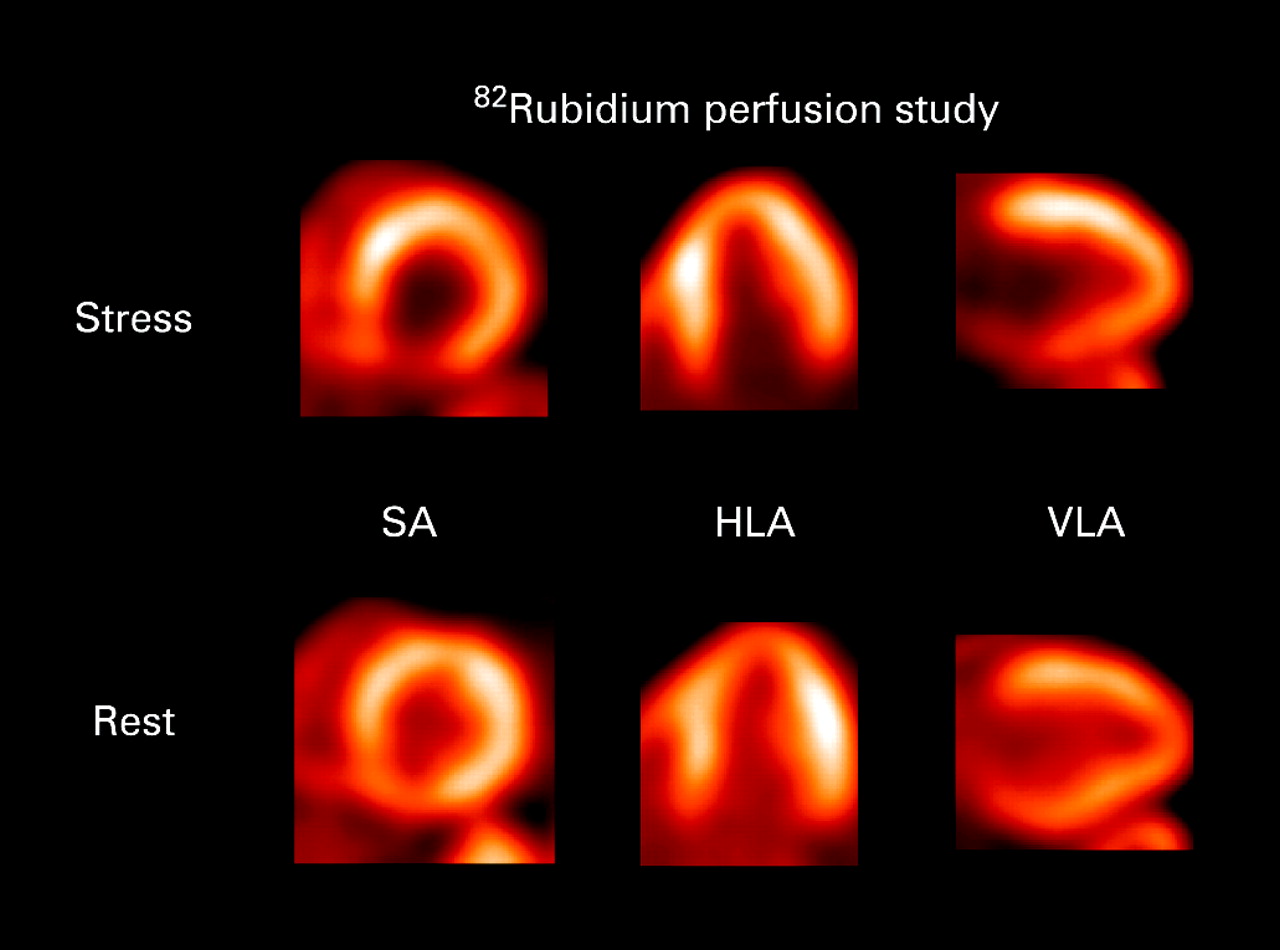
The potassium analogue 82Rb is a generator-produced tracer that has been increasingly used for clinical PET perfusion studies. The biological behaviour of 82Rb is similar to that of thallium-201 (201Tl), except for a lower myocardial extraction fraction.12 This generator-produced tracer is ideal for clinical semiquantitative evaluation of myocardial blood flow (fig 3). The potential for measurement of flow is still under investigation.
One unique area of PET is the study of cardiac neurotransmission and receptors on a molecular level. The regional distribution of cardiac nerve terminals can be visualised and a number of labelled analogues of norepinephrine have been investigated, but the most commonly used PET tracer is [11C]hydroxyephedrine (fig 4).14 15

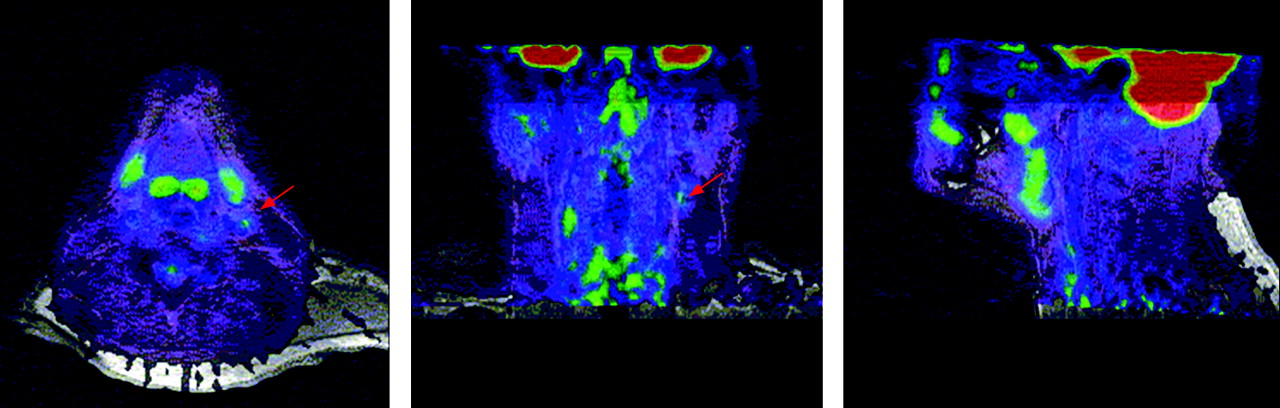
The short half-life of 11C limits its wider clinical use and the 18F-labelled tracers may have greater clinical potential. Tools to investigate β-receptors, α1-receptors, adenosine and muscarinic receptors have been also developed for PET, but clinical data are still limited.16 17 The new imaging targets are likely to become more important in the future when new treatments are developed. Tracers for imaging vulnerable atherosclerotic plaque18 and gene transfer imaging techniques19 are under evaluation and are likely to have great clinical potential (fig 5).20

Imaging protocols
Length of the imaging protocol depends on the tracer used. Typical perfusion imaging takes from 2 to 20 minutes. A dynamic scan is required for quantitative perfusion measurement. After decay of the tracer, the stress study is followed using pharmacological stressors such as adenosine, dipyridamole or dobutamine. Owing to short half-life of the PET tracers the stress study can be performed practically without delay after the rest study. The total time required for whole study session depends on the tracer used but typically the whole session can be finished in 30 minutes.21–23
Since the recent PET systems can list mode acquisition, the data can be collected simultaneously as an ECG gated mode that allows the assessment of regional and global left ventricular wall motion from the same scan data.21–23
For viability testing it is important that patients have been prepared accordingly since metabolic tracers are used. Typically uptake of FDG is compared against perfusion (fig 6) but quantitative analysis protocols have also been used. Currently, gated acquisition is preferred.7 21–23

When studies are performed using hybrid PET-CT scanners, both CT angiography and the PET study can be performed in the same session without a significant increase in time, making this approach very attractive.
Image analysis and interpretation
The analysis of PET studies follows the standard procedures explained in detail in guidelines.21–23 When hybrid PET-CT scanners are used analysis should be done also using fused images. In this way the individual coronary anatomy can be visualised together with functional information enabling accurate association between coronary anatomy and, for example, perfusion. If measurement of flow has been determined quantitatively, the absolute stress flow values should also be included in the analysis (see fig 2).
CLINICAL ROLE OF PET
PET in the detection of CAD
The diagnostic accuracy of the method in the detection of CAD has been investigated in a number of studies.21–37 It has been shown to be most accurate among non-invasive methods, with sensitivity and specificity of about 90%. In particular, the sensitivity for regional perfusion abnormalities is good and clearly better than with standard scintigraphy.35 This means that in the case of multivessel disease, anything other than the tightest stenosis can also be identified.
It is important to note that the accuracy above was mostly achieved using relative perfusion distribution. The quantification of myocardial blood flow and coronary vasodilator reserve is of diagnostic importance in patients with extensive CAD, in whom relative perfusion imaging such as SPECT may often disclose only the most severe lesion and miss the others. In addition, quantitative PET may diagnose CAD in patients with balanced ischaemia which may have a misleading normal regional perfusion pattern.
In the study by Parkash et al38 in patients with single-vessel CAD, defect sizes determined were smaller with quantification than with visual assessment, while in contrast, some regions with normal SPECT had impaired coronary reserve.39 This suggests that the quantification of coronary reserve by PET incorporates an additional value for the diagnosis of CAD and is thus likely to increase confidence in the interpretation.
Another unique feature of quantitative flow measurement is that it allows evaluation of very early changes in coronary vasoreactivity and the progression or regression of CAD at early stages.39–41 In the near future we will learn more about the clinical and prognostic significance of these early abnormalities.
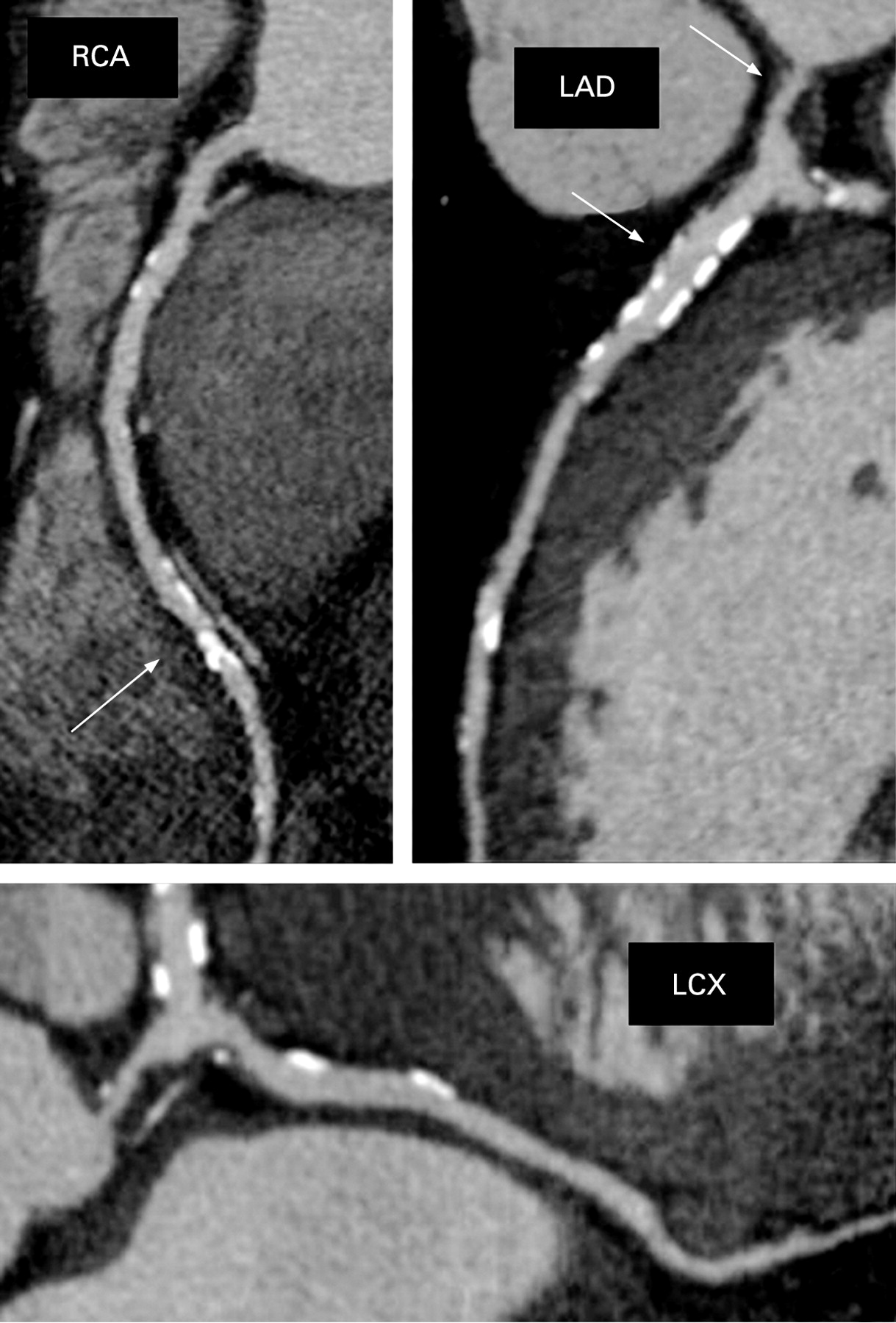
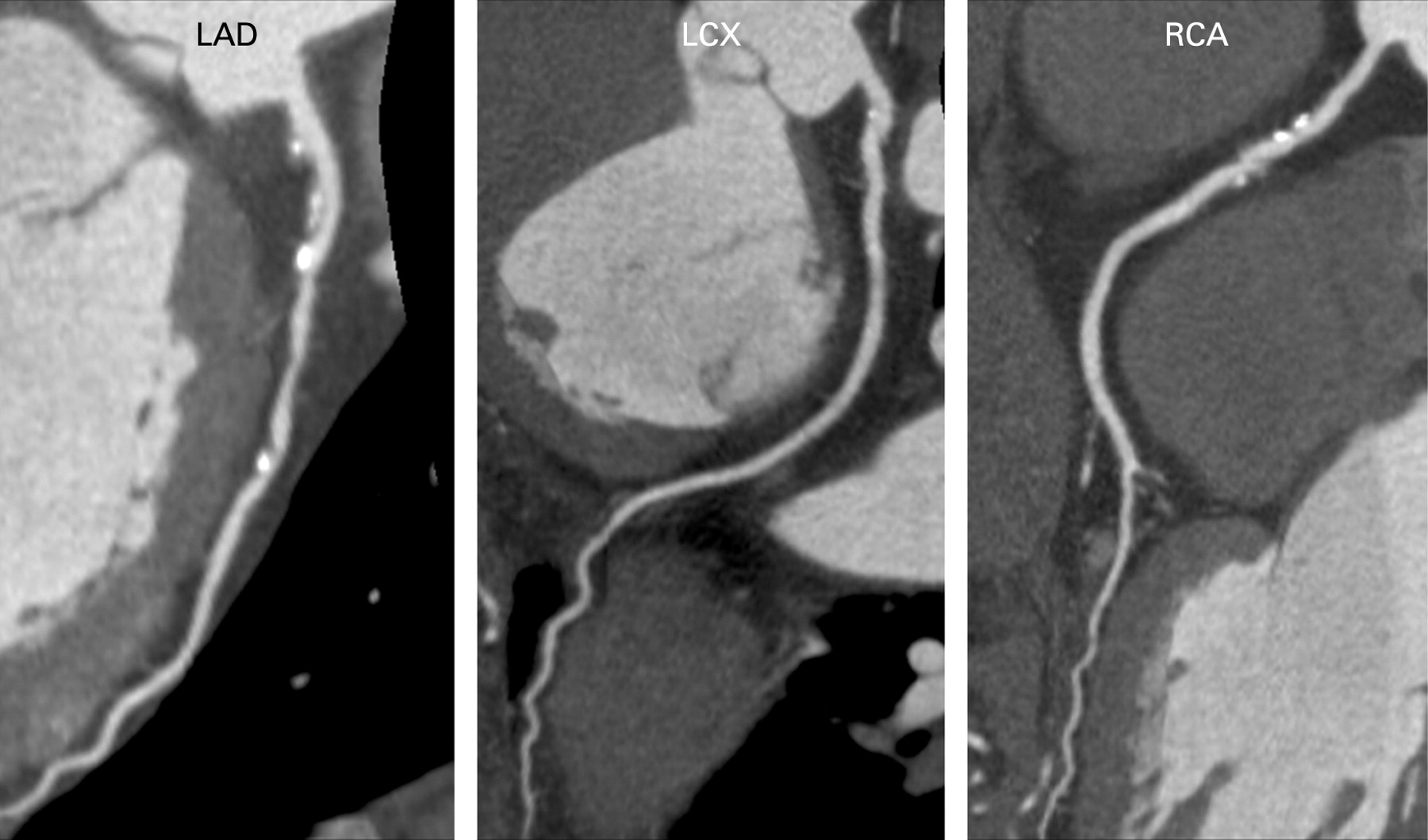
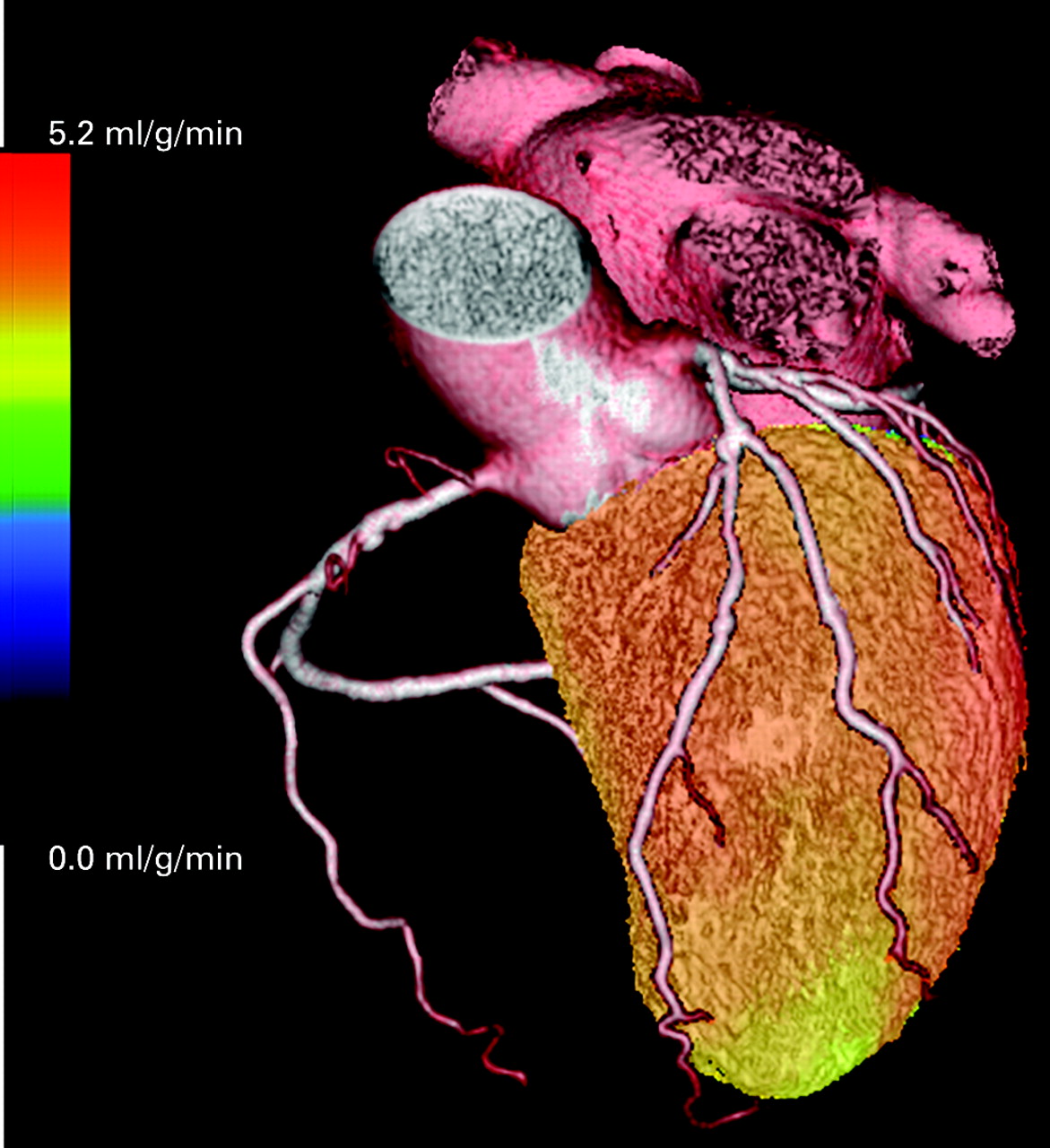
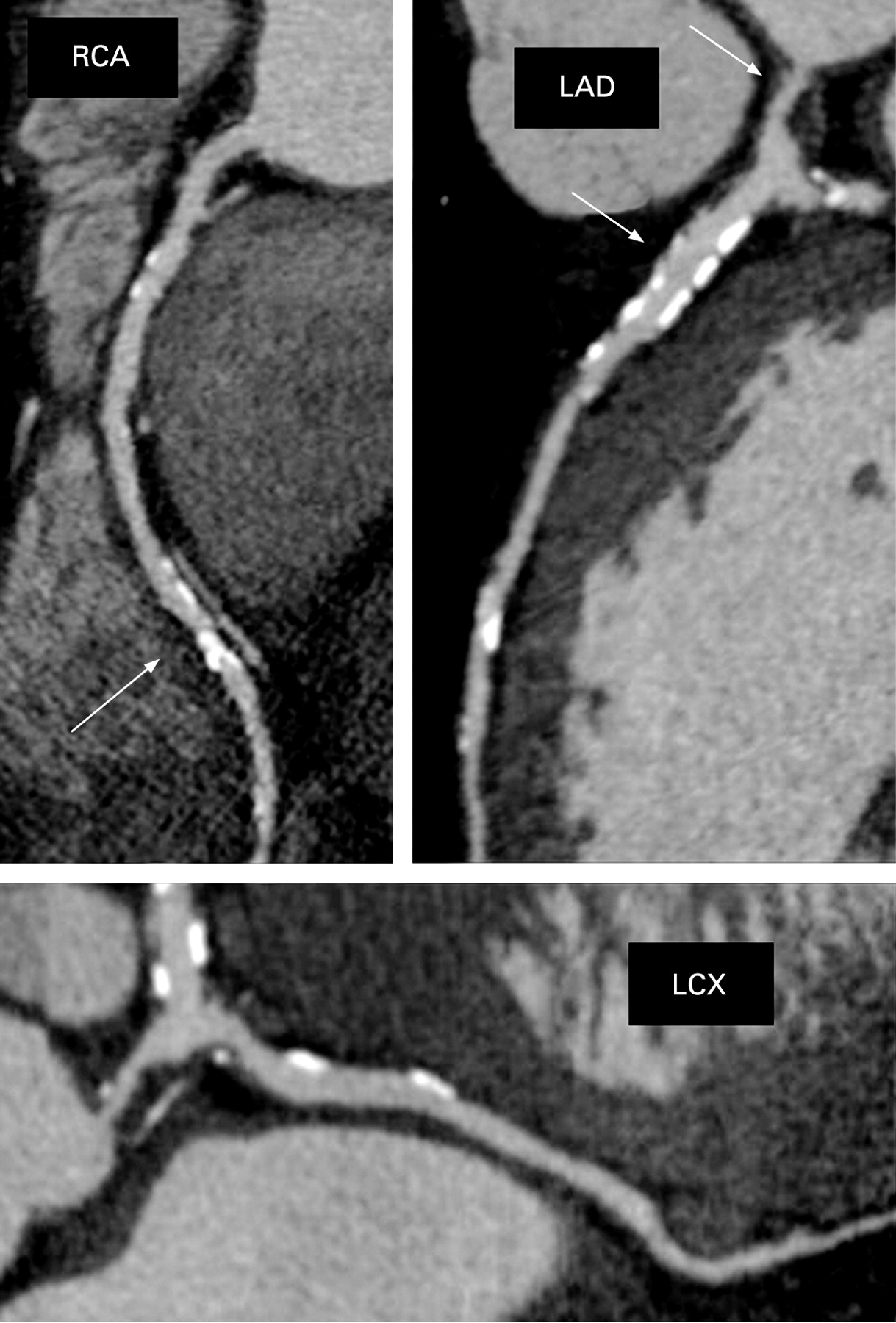
With hybrid systems, CT angiography and absolute perfusion can be done in the same session. CT angiography provides detailed information about coronary anatomy, plaque structure and location and has been reported to have a high negative predictive value. Combining this information with that obtained by PET perfusion, which provides functional information about the haemodynamic significance of coronary lesions, will probably also increase the positive predictive value of the test (figs 7–10).1 2 The clinical algorithms to be applied for hybrid systems are not yet established. One alternative is to start with CT angiography and continue with PET only if the CT finding is positive, and this may be particularly suitable for patients with a lower likelihood of CAD. For patients with a higher likelihood of disease starting with perfusion imaging may be justified owing to its higher specificity.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
PET in the assessment of viability
Evaluation of myocardial glucose utilisation with FDG and PET is currently considered the most reliable tool for identification of myocardial viability.7 PET imaging has been shown to predict improvement of regional and global function, improvement of heart failure symptoms, exercise capacity and long-term, event-free survival.42 43 In a recent consensus paper44 it was suggested that PET should be reserved for cases where clinical suspicion of viability or hibernation remains after other imaging techniques have proved negative. However, if PET is readily available it is a good alternative to other imaging techniques.
PET in the imaging of cardiac neuronal function
A number of positron-labelled tracers for imaging cardiac sympathetic and parasympathetic receptors with PET have been developed and validated.14 15 These include the catecholamine analogue [11C]hydroxyephedrine and tracers for the measurement of β-adrenoceptor and muscarinic receptors.16 17 These ligands allow the demonstration of abnormal autonomic function in different cardiac diseases, including dilated and hypertrophic cardiomyopathy and idiopathic arrhythmogenic diseases such as the Brugada syndrome.14 15 45 Imaging of myocardial neural function and innervation has been shown to have strong prognostic value in patients with heart failure.46
PET in monitoring of treatments
PET perfusion imaging in combination with pharmacological interventions has been applied extensively to the measurement of regional coronary flow reserve. A number of studies have evaluated regional coronary flow reserve in asymptomatic patients at risk for the development of CAD.39 40 Even in healthy young subjects, abnormal myocardial perfusion reserve is related to the number of conventional risk factors.40 All these studies have shown impaired vascular reactivity in patient populations at high risk for the development of CAD. In patients with heart failure flow reserve has important prognostic value.47 48 This approach also provides the means to monitor risk factor modifications using PET perfusion measurements as surrogate end point.41 49–54
In patients with heart failure, measurement of myocardial oxidative metabolism and cardiac efficiency of work can be used to monitor treatments. The new agents have been tested55 56 and resynchronisation therapy has been evaluated.57 Further large-scale clinical studies are needed to understand fully the value of this method in heart failure.
Neuronal imaging has been also used to identify responders to β-blockade treatment. Further clinical studies are required before the clinical value of these observations is known.
Imaging of vulnerable plaques, stem cells and gene therapy
The development of new specific tracers for inflammation, reporter genes and other specific targets holds great promise for the future clinical use of PET. In these new applications, hybrid imaging is needed since the anatomical landmarks from PET images with specific tracers are missing.
In the imaging of vulnerable plaque, non-invasive techniques such as multislice CT provide accurate localisation of plaques and also characterise morphological criteria associated with a high risk of atherosclerotic plaque rupture. In contrast, PET uses radiolabelled molecules designed to specifically target individual inflammatory activities in atherosclerotic plaques. Plaque rupture is usually a consequence of inflammatory cell activity within the plaque and techniques, which illustrate plaque anatomy and composition, do not provide information on plaque inflammation. In patients with symptomatic carotid atherosclerosis FDG PET-CT has been used to identify inflammation within plaques.58 A variety of cellular molecular targets involved in the progression and potential rupture of vulnerable plaques have been identified, including macrophage density, apoptosis and protease activity, and ligands for these targets are currently under development.
It might be suggested that the anatomical resolution of PET is a limitation of PET but this is less important than the sensitivity when aiming to image plaques that should be seen as hot spots. The resolution just defines the size of the hot spot that will be displayed in PET images. Sensitivity is the key factor and determines whether the target can be visualised and PET is known to have outstanding sensitivity. In addition, further development of advanced gating techniques (eg, both respiratory and ECG gating) is needed to detect these small moving targets.
The use of reporter genes and labelled reporter probes for non-invasive imaging of transgene expression is another emerging application of PET. This technique is based on a vector-mediated transfer of genes which translate into protein products such as enzymes or receptors that can be targeted by radiotracers. Accumulation of tracers thus indirectly reflects gene expression in target tissue. Several studies have reported proof of this principle for cardiac imaging.59–61 This methodology can be used to determine location, magnitude and persistence of transgene expression in the heart and the whole body. Coexpression of a reporter gene allows indirect imaging of the expression of a chosen therapeutic gene, and thus permits monitoring of cardiac gene therapy,62 but this promising approach is still in the experimental stage and has not yet been adapted for human application.
Even more than gene therapy, cardiac stem cell therapy is an innovative and promising therapeutic approach to heart disease. However, despite an increasing body of experimental and human data, several questions about the biological mechanisms of treatment remain to be answered, and unequivocal proof of clinical efficacy is needed. PET not only provides accurate non-invasive information about myocardial perfusion, contractile function and viability, which enables assessment of clinical benefits of treatment but is also well suited to tracking of transplanted cells by use of direct radionuclide labelling—for example, with FDG.63 Alternatively, reporter genes can be transferred to stem cells before transplantation for serial monitoring of cell viability using gene product imaging.64 This has the advantage of a direct link between the imaging signal and cell viability/function, but is technically more demanding owing to lower contrast and the need for genetic manipulation of therapeutic cells.
The gene- or cell-specific signal can be linked to physiological effects and can be used to refine the understanding of basic therapeutic mechanisms. Thereby, gene- and cell-targeted imaging will significantly enhance the determination of therapeutic effects in cardiovascular molecular therapy in the future.
CURRENT LIMITATIONS OF PET
Despite the exponential growth of PET scanners, their widespread availability for cardiac studies is still limited to large centres. This is, however, changing quickly and probably in the near future will not be a major limitation.
However, the availability of tracers will be more critical. The best perfusion tracers have currently very short half-lives and these need to be produced close to the imaging site. This makes routine application challenging and distribution of tracers impossible. Therefore, most clinical sites use generator based 82Rb, which, however, is not an ideal tracer for quantitative PET. Currently, new PET perfusion tracers are under development which are likely to improve the widespread acceptance of this technique for clinical routine.
As it is not much used in clinical routine, little information on the cost effectiveness of cardiac PET is available. Therefore, reimbursement is also an important limiting factor. Even more important, widespread clinical acceptance requires more data to confirm that PET can deliver its clinical promise. Although data show that PET is better, for example, than SPECT for diagnosing CAD,1 more data are needed. Despite the documented advantages of PET and reasonably large number of studies47–58 65 66 that have investigated the prognostic value of PET perfusion imaging, large trials have not been performed and databases have not been set up, and limited information about the additional value of the absolute perfusion is currently available.65 One might also argue that the achieved improvement in accuracy as compared with other imaging techniques is not sufficient justification for the use of this more demanding technique.
The same limitations are also valid with other applications of PET, perhaps with the exception of viability imaging. In heart failure monitoring small patient groups have been studied. The more specific the target, the less clinical information that is available. It is only with FDG PET that a considerable number of studies have proved the clinical value of PET.
PET uses radioactive compounds and, therefore, causes a radiation burden for patients. However, owing to the short half-lives of positron-emitting tracers the radiation dose is less of concern (stress–rest 13NH3 2.0 mSv, [15O]water 1.7 mSv, 82Rb 7.5 mSv) and clearly lower than that of SPECT imaging (stress–rest 201Tl 25 mSv, 99mTc-tracers 10–16 mSv or standard multislice CT angiography 9–20 mSv).21 When hybrid imaging is performed the radiation burden needs even more attention. With PET-CT the major part of the radiation is caused by CT angiography. However, recent development of CT imaging protocols is reducing the radiation dose strikingly and when these techniques are used, hybrid imaging with CT angiography and rest–stress PET perfusion can be performed with a total radiation dose clearly below 10 mSv.
FUTURE DEVELOPMENT OF PET
The continuing trend is for the fast spread of hybrid PET scanners with multislice CT. These systems are likely to fundamentally change the field of cardiac imaging since they allow comprehensive imaging of cardiac function with anatomical coregistration. With these devices coronary anatomy and quantitative perfusion can be studied in a single session of less than half of an hour.
Current limitations of the perfusion tracers are likely to be overcome in the near future. It is also expected that the more specific imaging targets such as plaque or gene expression will have clinical application. These new targets will give PET imaging a unique role.
Personalised medicine seems to be one of the future trends. This means that the demanding and expensive treatments of the future need to be targeted and patient subgroups selected carefully. This also means that imaging techniques, especially molecular imaging, may have a pivotal role in this process.20 PET provides a unique and powerful method to bridge the gap between molecular biology, pathophysiology and targeted treatment.
CONCLUSIONS
The use of PET in cardiology is growing rapidly. Technical features make PET a strong tool for the non-invasive evaluation of cardiac physiology. The newest generation of PET systems with integrated multislice CT have matured to a level at which they can be successfully used for clinical cardiac imaging. These hybrid systems are becoming a standard technique. The methods are complementary and make the combination particularly attractive for the assessment of CAD. Finally, there are also promising future applications that involve molecular imaging of cardiac targets and those may further enhance the clinical utility of PET and hybrid imaging.
REFERENCES
Footnotes
Competing interests: None.