Article Text

Abstract
Objectives: Ejection fraction (EF) and end-systolic volume index (ESVI) are established predictors of outcomes following ST-segment elevation myocardial infarction (STEMI). We sought to assess the relative impact of infarct size, EF and ESVI on clinical outcomes and left ventricular (LV) remodelling.
Design: Prospective cohort study.
Setting: Academic hospital in Chicago, USA.
Patients: 122 patients with STEMI following acute percutaneous reperfusion.
Main outcome measures: Death, recurrent myocardial infarction (MI) and heart failure.
Methods: Cardiac magnetic resonance imaging was obtained within 1 week following STEMI in 122 subjects. ESVI, EF and infarct size were tested for the association with outcomes over 2 years in 113 subjects, and a repeat study was obtained 4 months later to assess LV remodelling in 91 subjects.
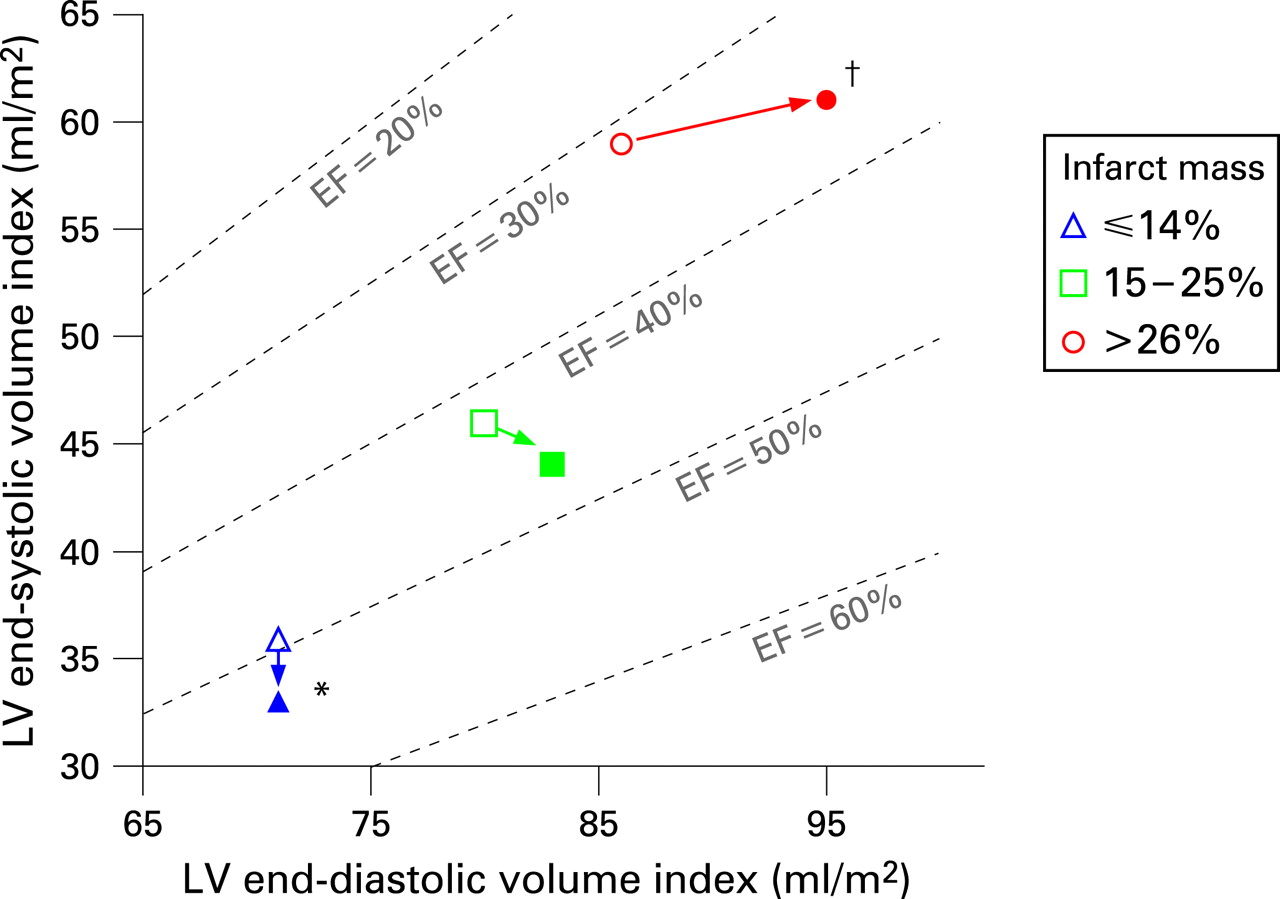
Results: Acute infarct size correlated linearly with the initial ESVI (r = 0.69, p<0.001), end-diastolic volume index (EDVI) (r = 0.42, p<0.001) and EF (r = −0.75, p<0.001). All were independently associated with outcomes (one death, one recurrent MI and 16 heart failure admissions). However, infarct size was the only significant predictor of adverse outcomes (p<0.05) by multivariate analysis. The smallest infarct size tertile had an increased EF (49% (SD 8%) to 53% (6%); p = 0.002) and unchanged EDVI (p = 0.7). In contrast, subjects with the largest infarct tertile also had improved EF (32% (9%) to 36% (11%); p = 0.002) at the expense of a dramatic increase in EDVI (86 (19) to 95 (21) ml/m2; p = 0.005).
Conclusions: Infarct size, EF and ESVI can predict the development of future cardiac events. Acute infarct size, which is independent of LV stunning and loading, directly relates to LV remodelling and is a stronger predictor of future events than measures of LV systolic performance.
Statistics from Altmetric.com
Clinical outcomes following an acute myocardial infarction are significantly determined by the initial structural and functional alterations resulting from myocardial necrosis.1–3 Both left ventricular (LV) ejection fraction (EF) and LV end-systolic volume have been well established as powerful predictors of short-term and long-term morbidity and mortality in both the pre-thrombolytic and post-thrombolytic eras.4 5 In addition to myocardial necrosis and subsequent scar formation, LV dysfunction can also occur in salvaged and viable myocardium following acute myocardial infarction (MI) due to either myocardial stunning6 or hibernation.7
Cardiac magnetic resonance (CMR) imaging is an emerging technique gaining widespread acceptance and applicability. Particularly, contrast-enhanced CMR imaging offers an opportunity to distinguish and quantify viable from irreversibly injured myocardium with unusual precision8 9 independently of abnormal wall function or perfusion that may occur following reperfusion. Volumes and systolic function can be accurately measured with better interstudy reproducibility than echocardiography10 and in identifying small subendocardial infarcts otherwise not detected by nuclear scintigraphy.11 12
The present study was undertaken to evaluate the relative impact of the acute infarct size, EF and end-systolic volume on the subsequent adaptive volumetric remodelling changes following an acute ST-segment elevation myocardial infarction (STEMI). In particular, we sought to investigate only a focused cohort of patients receiving an optimal revascularisation strategy treated with primary percutaneous coronary intervention (PCI). We hypothesised that the initial infarct burden quantified as the acute infarct size by CMR would predict subsequent LV remodelling and hence identify patients at risk of future adverse cardiac events with greater accuracy than end-systolic volume or EF.
METHODS
Patient selection
We prospectively enrolled 124 patients admitted to the coronary care unit at Northwestern Memorial Hospital for STEMI between April 1999 and June 2006. Patients were included if they fulfilled the criteria of documented acute STEMI with (1) chest pain for more than 30 minutes, (2) at least 1.0 mm ST-segment elevation in two contiguous leads and (3) elevated creatinine phosphokinase MB (CPK-MB) isoenzyme levels, and if they agreed to undergo a CMR evaluation within 1 week and again at least 3 months after presentation. We did not recruit patients with a known history of previous acute MI, PCI or coronary artery bypass surgery. We also excluded patients with frequent and recurring ventricular arrhythmias, unstable haemodynamics requiring intravenous inotropic agents, or contraindications to CMR such as pacemakers or defibrillators.
Of the 124 patients with STEMI originally enrolled, two patients were unable to complete the acute CMR because of claustrophobia. A total of 91 patients returned for an additional follow-up CMR examination. Of the remaining 31 patients, five had an implantable cardioverter defibrillator and one had a pacemaker placed >1 week after STEMI, four withdrew from the study because of claustrophobia, two moved from the area and 19 patients were unable to be contacted for a follow-up CMR study. Before the first CMR study, all participants gave written informed consent to the study protocol, which was approved by the Northwestern University institutional review board.
Cardiac magnetic resonance
CMR was performed in a 1.5 T clinical scanner (Sonata or Avanto, Siemens, Erlangen, Germany). All images were acquired during repeated breath-holds and were electrocardiographically gated as previously described by our group.8 9 13 14 Functional assessment of the left ventricle was performed without contrast using a cine steady-state free precession sequence. Sequential short axis images were acquired every 10 mm to cover the entire left ventricle. Infarct images acquired at identical slice positions were then obtained starting 10 minutes after the administration of gadopentetate dimeglumine (gadolinium-DTPA; Berlex, Montville, NJ, USA) 0.2 mmol/kg of body weight using a T1-weighted, inversion-recovery, fast gradient-echo pulse sequence with inversion times were set to null normal myocardium.13 Matrix size was 256 resulting in a typical voxel size of 1.4 by 1.4 by 6.0 mm.
All CMR images had identifying data removed for analysis and images were randomised and blinded to other study data and outcomes. Quantitative analysis of LV mass, end-diastolic volume, end-systolic volume, and EF was performed by manually tracing the epicardial border (excluding epicardial fat) and endocardial borders (excluding papillary muscles) at end-diastole and end-systole for each short-axis slice using ImageJ (National Institutes of Health, Bethesda, MD, USA). Three-dimensional volumes were calculated as the sum of (area × (slice thickness + distance between slices)) for all short axis slices. Volume indices were calculated by dividing the end-diastolic volume (EDVI) or end-systolic volume (ESVI) by the body surface area. Adverse LV remodelling was defined as an increase in EDVI ⩾20%.15 17
Contrast-enhanced CMR images were analysed to determine infarct volume. Each slice was magnified and interpolated by a factor of 3, and the hyper-enhanced infarct features were evaluated and hand planimetered by a single, expert observer in each short axis slice.8 9 13 Infarct size was calculated as a percentage of the hyper-enhanced areas to the total LV volume. Areas of microvascular obstruction (dark areas of absent contrast surrounded by hyper-enhanced infarct tissue on delayed contrast enhanced images) were included in the total infarct size.16 17 Using a 17-segment model,18 the number of segments with microvascular obstruction were summed to calculate the microvascular obstruction score, and the number of segments with transmural hyper-enhancement were summed to calculate the infarct transmural score.
Outcome measures
Major cardiac events (MACE) were defined as cardiac death, non-fatal re-infarction and symptomatic congestive heart failure requiring hospitalisation. Only one event was tabulated per subject. The subjects’ individual managing physician determined treatment following STEMI. Follow-up information was collected at the time of the follow-up CMR study, patient telephone interviews and chart reviews. Office and hospital chart follow-up reviews were able to be obtained in 12 of the 19 subjects lost to CMR follow-up.
Statistical analysis
Results are expressed as mean (SD), unless otherwise noted. Proportions were compared across patient groups using χ2 tests. LV morphological and infarct-related continuous variables were compared between baseline and follow-up studies using paired t tests. Correlation between variables was calculated using Spearman’s rho or Pearson’s correlation, as appropriate. Cox proportional hazards regression model was used to identify predictors of MACE. Proportional hazards assumption was tested with a time-dependent covariate. Multivariate linear regression was performed to identify independent determinants of subsequent follow-up ESVI and EF separately for each end point of interest. All covariates with a univariate p value ⩽0.2 were eligible for inclusion in the multivariate regression models. Receiver operating characteristic (ROC) curve analysis was performed to establish diagnostic accuracy in the prediction of MACE. Event-free survival curves for MACE and remodelling were constructed using the Kaplan-Meier method, and statistical differences between the curves were assessed by log-rank test. A two-tailed p value<0.05 was considered statistically significant.
RESULTS
Baseline characteristics
The clinical and angiographic characteristics are shown in table 1. All subjects had successful reperfusion with PCI within 24 hours of presentation to the hospital except for one subject with thrombolysis in myocardial infarction (TIMI) grade 1 flow following PCI, one subject who had an unsuccessful PCI attempt to a left circumflex occlusion and one subject with PCI to the non-infarct related artery. In all, 119 subjects received intracoronary stents (64 bare metal stents and 55 drug-eluting stents).
Acute CMR study
The acute CMR data in 122 subjects are listed in table 2, column 1. No images were excluded from analysis. The median number of days from admission to the acute CMR study was 2 (25–75 percentiles: 2–4) days.
All subjects, except for one, had evidence of hyper-enhancement on the acute CMR study. Figure 1 shows a sample patient with an infarct size of 39%. For the entire cohort excluding the one patient without hyper-enhancement, the infarct size ranged from 3% to 63%.

The acute infarct size correlated significantly with the acute EDVI, ESVI and EF (fig 2A, B, and C). The acute infarct size also correlated significantly with the peak CPK-MB (r = 0.56; p<0.001), transmural infarct score (r = 0.76; p<0.001) and microvascular obstruction score (r = 0.57; p<0.001). Patients with microvascular obstruction (n = 51) had larger infarct sizes (29% (14%) than without (17% (11%), p<0.001). Additionally, patients with occlusion in the left anterior descending artery (n = 64) had larger infarct sizes (28% (15%) than other arterial territories (16% (9%), p<0.001). There was no difference in the mean infarct size (22.3% (13.4%) versus 22.2% (14.1%); p = 1.0) and the mean EF (39% (13%) versus 42% (11%); p = 0.3) between the 98 patients taking angiotensin converting enzyme (ACE) inhibitors and those that were not.

Outcome measures
Clinical follow-up data were collected for 113 subjects. The median length of clinical follow-up was 538 (25–75 percentiles: 198–694) days. During this period, there was one cardiac death, one patient with a documented recurrent myocardial infarction and 14 patients readmitted for congestive heart failure. These 16 subjects had significantly greater acute infarct size as well as other indices of adverse remodelling (table 3). Other significant predictors of MACE included TIMI flow grade following PCI (p<0.001) and the number of vessels with significant CAD (p = 0.01). Of note, there were no differences based on age, gender or medical treatment including ACE inhibitors.
Univariate analysis using a Cox regression for the prediction of MACE found infarct size, ESVI and EF to be independently significant. However when evaluating only these three variables in a multivariate analysis, the acute infarct size was the strongest significant predictor of MACE. The acute ESVI or EF did not significantly improve the predictive model (table 4). To maximise sensitivity in this high-risk population for adverse clinical events, a cut-off infarct size ⩾18.5% had a sensitivity of 88% and a negative predictive value of 96%. Kaplan-Meier analysis demonstrated that this infarct size cut-off of ⩾18.5% was a significant predictor of MACE (fig 3A).

Follow-up CMR study
A total of 91 subjects returned for a follow-up CMR study (median days from STEMI to CMR 125 (25–75 percentiles: 98–174)). There were no statistical differences in the baseline clinical characteristics or CMR findings between this subgroup and the 31 subjects whom did not return for a follow-up CMR study (table 2). During the period between the acute and follow-up CMR, one subject underwent PCI for in-stent restenosis, one subject was readmitted for unstable angina with subsequent PCI to other coronary lesions, and one subject had coronary bypass surgery.
The correlation coefficients between the acute infarct size increased with the follow-up EDVI, ESVI and EF studies (fig 2D, E, and F). The follow-up infarct size decreased by 22.0% of the initial size—an absolute decrease of 4.3% (5.5%).
Left ventricular remodelling
Univariate predictors for the follow-up ESVI included the acute infarct size, acute EDVI and ESVI, number of days till the follow-up CMR study, peak CPK-MB, microvascular obstruction score, infarct transmural score, TIMI perfusion scores and history of tobacco use and hypercholesterolaemia. Of note, ACE inhibitor use was not a significant predictor of ESVI. By multivariate linear regression analysis, the acute ESVI (p<0.001) and the acute infarct size (p = 0.001) were the only significant independent predictors for the follow-up ESVI.
Similarly univariate predictors for the follow-up EF included the acute infarct size, acute and follow-up EDVI and ESVI, number of days till CMR study, peak CPK-MB, microvascular obstruction score, infarct transmural score, anterior infarct location, TIMI perfusion scores and history of hypertension, tobacco use and hypercholesterolaemia. When controlling for the EDVI and ESVI, multivariate linear regression analysis found the acute infarct size (p<0.001) and microvascular obstruction score (p = 0.04) were the only significant independent predictors for the follow-up EF.
The presence of adverse LV remodelling was also predictive of cardiac events (fig 3B). Adverse LV remodelling occurred in 15 subjects (16%) who had significantly larger infarct size (30% (16%)) than those subjects without remodelling (19% (11%), p<0.05). Using the same infarct size cut-off of 18.5%, the sensitivity for detecting LV remodelling was 73% and specificity was 52%. The negative predictive value remained high at 91%. Furthermore, differences in LV remodelling can be illustrated when subdividing the 91 subjects into tertiles based on the acute infarct size, the EF significantly improved within each tertile. However, different adaptive changes in the ESVI and EDVI were observed according to the acute infarct size (fig 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
DISCUSSION
Despite optimal interventional management of acute STEMI and application of evidence-based secondary prevention measures in a large, metropolitan academic hospital, we demonstrated that both early and late volumetric changes associated with adverse LV remodelling occur in a linear relation with the acute infarct size. In fact, LV enlargement is readily evident within the first few days following STEMI. Additionally reaffirming previous clinical trials, infarct size, ESVI and EF performed within 1 week after an acute STEMI can predict the development of future cardiac events. The different adaptive volumetric changes were observed in response to different degrees of acute infarct burden to maintain overall LVEF. However, despite the presence of LV functional adaptation and infarct healing, the initial infarct burden as delineated by the infarct size was the strongest predictor of persistent LV enlargement and future cardiac events. These pathophysiological events are well demonstrated by CMR imaging.
Predictors of events
Several non-invasive techniques have been used to assess ESVI and EF after acute myocardial infarction, including contrast ventriculography, radionuclide angiography and echocardiography. White et al in 1986 established that determination of end-systolic volume 1–2 months following acute myocardial infarction is the major determinant of subsequent survival.5 Additionally, Bolognese et al in 2002 using echocardiography identified age and end-systolic volume as the baseline and 6-month predictors for cardiac death.15 Consistent with these previous studies, our study indicates that ESVI and EF are similarly strong predictors of cardiac outcomes in a cohort of patients following acute PCI reperfusion and subsequent secondary prevention treatments.
However, both ESVI and EF within 7 days of a STEMI can be inaccurate measures of the extent of irreversible myocardial injury because of ischaemic stunning or previous areas of chronic hibernation. In either case, LV function may be severely depressed despite the presence of viable myocardium.14 In this study, directly measuring the acute infarct size was more predictive of events than either the acute ESVI or EF. CMR can determine the true extent of myocardial damage before hospital discharge and, as demonstrated by the current data, predict the LV volumetric adaptive changes that develop weeks to several months following STEMI. Additionally, this CMR hyper-enhancement technique is not affected by resting wall function abnormalities, which can overestimate the infarct size caused by myocardial stunning,19 nor by impaired resting perfusion in the peri-necrotic areas despite epicardial arterial reperfusion as hypothesised by nuclear perfusion studies.20
Nuclear myocardial perfusion imaging has been well established for estimating the amount of acutely infarcted tissue and has shown a strong association with other markers of infarct size and survival.21 22 The same association between acute infarct size and events was reported in other smaller CMR studies by Wu et al in 44 patients23 and by Hombach et al in 116 patients (60 patients with STEMI).17 However in the study by Burns et al in using technetium-99m single photon emission computed tomography to measure the acute infarct size 6–16 days after STEMI in 753 patients, EF remained the strongest predictor of mortality over infarct size and ESVI by multivariate analysis.4
There are several differences in our study that could explain these apparently disparate results. In the study by Burns et al, revascularisation was performed with thrombolytics while our population underwent acute reperfusion with PCI. Burns et al evaluated mortality at 6 months where as we followed subjects for up to 2 years. Additionally, Burns et al measured EF and infarct size 1–2 weeks following acute infarction to negate ischaemic stunning while we evaluated these parameters a median of 2 days following STEMI. The Pearson correlation between infarct size and EF was −0.67 measured by nuclear scintigraphy by Burns et al; in this study of only 122 subjects, there was a better correlation (r = −0.75) by CMR. Lastly, infarct size measurements by CMR and nuclear SPECT are dissimilar. Myocardial infarct areas by nuclear SPECT are seen as tracer uptake defects caused by impaired coronary perfusion, whereas infarct areas by CMR are seen as gadolinium contrast accumulation within necrotic areas as a result of increased extracellular space. These subtle differences may represent different pathophysiological states following acute myocardial infarction, and therefore the results from from different non-invasive measurements of infarct size may diverge.
LV volumetric adaptation and remodelling
“Infarct expansion” within the first few days following acute myocardial infarction is characterised by early LV enlargement24 and similar patterns of enlargement were observed in our study. The enlarged LV volumes appear to develop in an attempt to adapt to the loss of functioning myocardium and to improve global cardiac performance both acutely and chronically. These compensatory responses develop to maintain LV stroke volume as EF declines. Our data indicate that not only are these indices of remodelling closely related to the degree of irreversibly injured myocardium at the time of hospital discharge, but also have a strong linear relation with subsequent LV volumes several months later despite infarct healing. Our data support the observations of Bolognese et al15 that a 20% or greater increase in EDVI was associated with increase in adverse events.
Moreover, LV volumetric adaptation to the initial infarct burden compensates differently in the months following STEMI in relation to the initial infarct size. All subjects had an improvement in EF, but this improvement in EF resulted from different changes in volumes. Patients with the smallest infarcts improved the stroke volume and EF, primarily through a reduction in the ESVI. As infarct sizes increase, any improvement in the EF came at the expense of increases in EDVI with little changes in the ESVI. Subjects with the largest infarct sizes not only had the largest volumes on the baseline study, but also continued to have insidious LV dilation beyond the early LV enlargement.
Clinical implications
To maximise sensitivity in a population of patients following STEMI, an infarct size cut-off of 18.5% was chosen. The negative predictive value for both predicting which patients following STEMI will not develop MACE or adverse LV remodelling were both high at over 90%. This high negative predictive value would suggest that quantifying the amount of infarcted myocardium can be a good negative screening test in patients. Therefore, CMR can prospectively discern which patients warrant close monitoring as well as identify a cohort to focus future investigative therapies to prevent both LV remodelling and MACE.
Limitations
Twelve subjects lost to CMR follow-up were confirmed by office and hospital chart reviews to assess for MACE, and no information was able to be obtained in nine subjects. The lack of direct contact to confirm clinical outcomes may influence these results. Additionally, the limited events and the small sample size restrict the conclusions by multivariate analysis, especially evaluating other potential CMR markers for MACE including infarct transmurality25 or microvascular obstruction.17 23 In fact, none of nine patients with microvascular obstruction and an infarct size <18.5% had MACE. Our study did find TIMI perfusion scores, the extent of CAD, infarct transmurality and microvascular obstruction as other significant predictors of MACE. The limited MACE outcomes constrained our multivariate analysis to compare only CMR infarct size to the two long-established, non-invasive variables in EF and ESVI on remodelling and clinical outcomes based on the established previous works by White et al and Burns et al.
Infarct size largely determines LV contraction and thus ESVI and EF, and the results of this study reveal a strong linear relation between infarct size, ESVI and EF. Low EF is a powerful predictor of long-term clinical outcomes, and a reduction in EF in relation to the infarct size likely represent large areas of viable, hibernating myocardium.8 This altered relation was not seen readily during the 3-month follow-up (fig 2F), and therefore further increasing the sample size in a larger clinical study may show a better prognostic ability for EF during long-term clinical follow-up.
Furthermore, the incidence of LV remodelling could potentially be found if CMR imaging was performed within the first day of acute STEMI. It is also currently unclear whether infarct sizes significantly changes within the first week after STEMI.
Conclusion
Infarct size, ESVI and EF measured within 1 week after an acute STEMI can predict the development of adverse cardiac events within a 2-year follow-up period. Infarct size measured by contrast-enhanced CMR, which is independent of LV stunning and loading, can predict the development of adverse events independently of LV ESVI and EF. Determining the acute infarct size before hospital discharge has the potential to accurately identify high-risk individuals for targeted therapy or closer follow-up.
Acknowledgments
The authors express their gratitude to Schnabel Samson, RN, for her efforts in patient recruitment, data collection and project coordination.
REFERENCES
Supplementary materials
web only media 94/6/730
Footnotes
▸ A video view of figure 1 is published online only athttp://heart.bmj.com/content/vol94/issue6
Funding: This work was supported in part by grants from the GlaxoSmithKline Research and Education Foundation for Cardiovascular Disease (EW) and the American Heart Association Scientist Development Grant (EW), by the Department of Medicine, and the Feinberg Cardiovascular Research Institute of Northwestern University. JTO was supported by the Working Group on Ischemic Cardiomyopathy of the Spanish Society of Cardiology.
Competing interests: None.