Article Text

Abstract
Background: Familial hypercholesterolaemia (FH) is associated with highly raised low-density lipoprotein-cholesterol and causes early-onset cardiovascular disease. Its autosomal dominant inheritance allows family cascade screening to be performed once an index case has been identified. However, the vast majority of people with FH in the United Kingdom have not been identified, and there is no national screening programme.
Objective: To assess the utility of combined computer- and notes-based searches in identifying index cases of FH in primary care, and to uncover the degree of case overlap with secondary care.
Methods: Four computer searches were conducted in one South London practice with a registered population of 12 100 patients. Selected notes were reviewed by a general practitioner and consultant lipidologist to give a Dutch score for the probability of FH.
Results: 402/12 100 (3.3%) patients had a Dutch score high enough to require a notes review. Twelve cases of definite FH were found, of whom two were unknown to the practice. Eight probable cases were found, seven of whom were previously unknown. 2/12 (17%) definite cases and 4/8 (50%) probable cases were unknown to a secondary care lipid clinic. 216/402 (54%) patients scored as possible cases. After specialist review 47/216 (21.8%) patients would merit recalling for a detailed family history and xanthoma examination.
Conclusions: There are both diagnosed and undiagnosed cases of FH in primary care not known to secondary care. Significant potential exists to identify new cases of FH in primary care who could act as new index cases for a family screening programme.
Statistics from Altmetric.com
Familial hypercholesterolaemia (FH) is an important treatable cause of premature ischaemic heart disease (IHD) and is caused by mutations in three genes associated with the function of the low-density lipoprotein (LDL) receptor.1 High levels of morbidity and mortality are associated with untreated FH, and before statin treatment men with FH had more than a 50% risk of IHD by the age of 50, and women had a risk of 30% by the age of 60.2 3 Early treatment increases life expectancy.4 The prevalence of FH is approximately 1 in 500 of the general population giving an estimated 116 000 cases in the UK. Less than 10% are thought to be known within secondary care lipid clinics.5 6 For a primary care trust (PCT) of 200 000 people there may be 400 cases, while a practice of 12 000 patients might have 25 cases.
The diagnosis of FH is based on cholesterol levels, a personal history of premature IHD, the presence of tendon xanthoma and a family history of premature IHD.7–9 By scoring these features the Dutch criteria (appendix 1) can be used to give a definite (>8), probable (6–8) or possible (3–5) score for FH.8 The alternative Simon Broome criteria uses a more straightforward diagnostic algorithm dividing patients into definite and probable cases.7 Current UK guidelines advise detailed investigation of patients with a total cholesterol >7.5 mmol/l.10
Because FH shows autosomal dominant inheritance, one in two close relatives will also have the condition. Family screening programmes have been established in other countries—for example, Holland,8 and a pilot screening study is taking place in the UK.11 12 A number of methods have been employed to uncover new index cases.13–15 However, the most cost-effective method is thought to be screening the relatives of known cases,16 and the Dutch community-based follow-up of index cases has been successful.8 Given the patchy geographical provision of current UK secondary care lipid clinics and the limitations of existing secondary care cohorts, additional case-finding strategies in the UK will be required.6 The scope for primary care to yield new index cases has not been looked at in depth, although the potential of primary care is acknowledged.16 Opportunistic screening combined with targeted testing, or targeting primary care patients with identified risk factors, may be effective screening strategies.5 15
Until recently, a systematic search for new cases of FH in primary care would have involved manual searching of case notes. UK primary care patient records are in a state of flux, with older information—for example, pretreatment cholesterol results, only being available in the written notes, and newer information only in the computer-based record. Major diagnoses such as lipid disorders and IHD can now be Read coded. Read codes are the current primary care, NHS wide, alpha-numeric coding system, enabling computerised patient records to be electronically searched. Laboratory results are now transmitted directly into the computer record while prescribing is also computerised. Because of national initiatives such as the National Service Framework for Coronary Heart Disease,17 virtually all practices are computerised and have improved their coding of major diseases. All these factors may enable computerised records to be used to identify which written records could be reviewed for potential cases of FH. The computerised or written record may not contain all the information required to score a patient fully. The exact questions required to do so may never have been asked in the past or the patient may not have had a cholesterol test. No previous work on this subject has been done in primary care so the nature of the searches that would best identify records can only be surmised.
We aimed to design a number of computer searches to identify which written records might be reviewed. We also aimed to quantify the number of known and unknown cases of FH, and to quantify the number of patients whose records did not contain enough information to provide a Dutch score. These patients would require face to face interview for detailed family history and xanthoma examination, but we did not intend to carry out these interviews in this study. For each search we aimed to calculate the sensitivity, yield and number of notes searched to find one case. It was expected that this information would help us to understand which search strategy might be the most cost effective. We aimed to assess the agreement between the computerised and written patient record with respect to the highest computer-based cholesterol and lowest age of IHD onset for each patient. As a family history of early onset IHD is central to making the diagnosis of FH, the quality of the family history in the patient record was also assessed. We also set out to identify how many primary care recognised cases of FH are not known to the local specialist referral centre, the only current source of a family cascade screening programme, and how many records of patients with FH contained information about a recommendation to carry out family screening and whether this had been undertaken.
METHODS
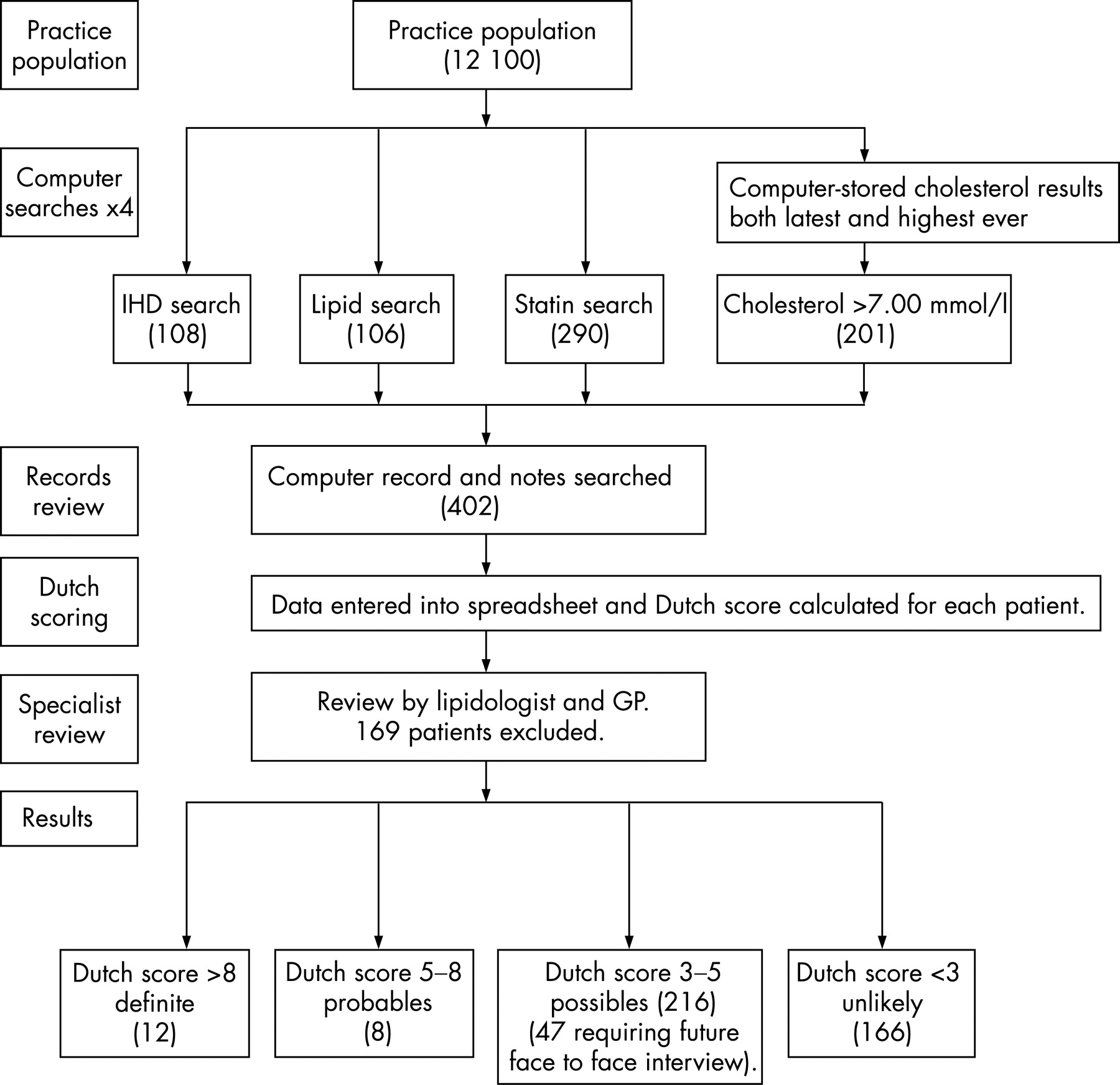
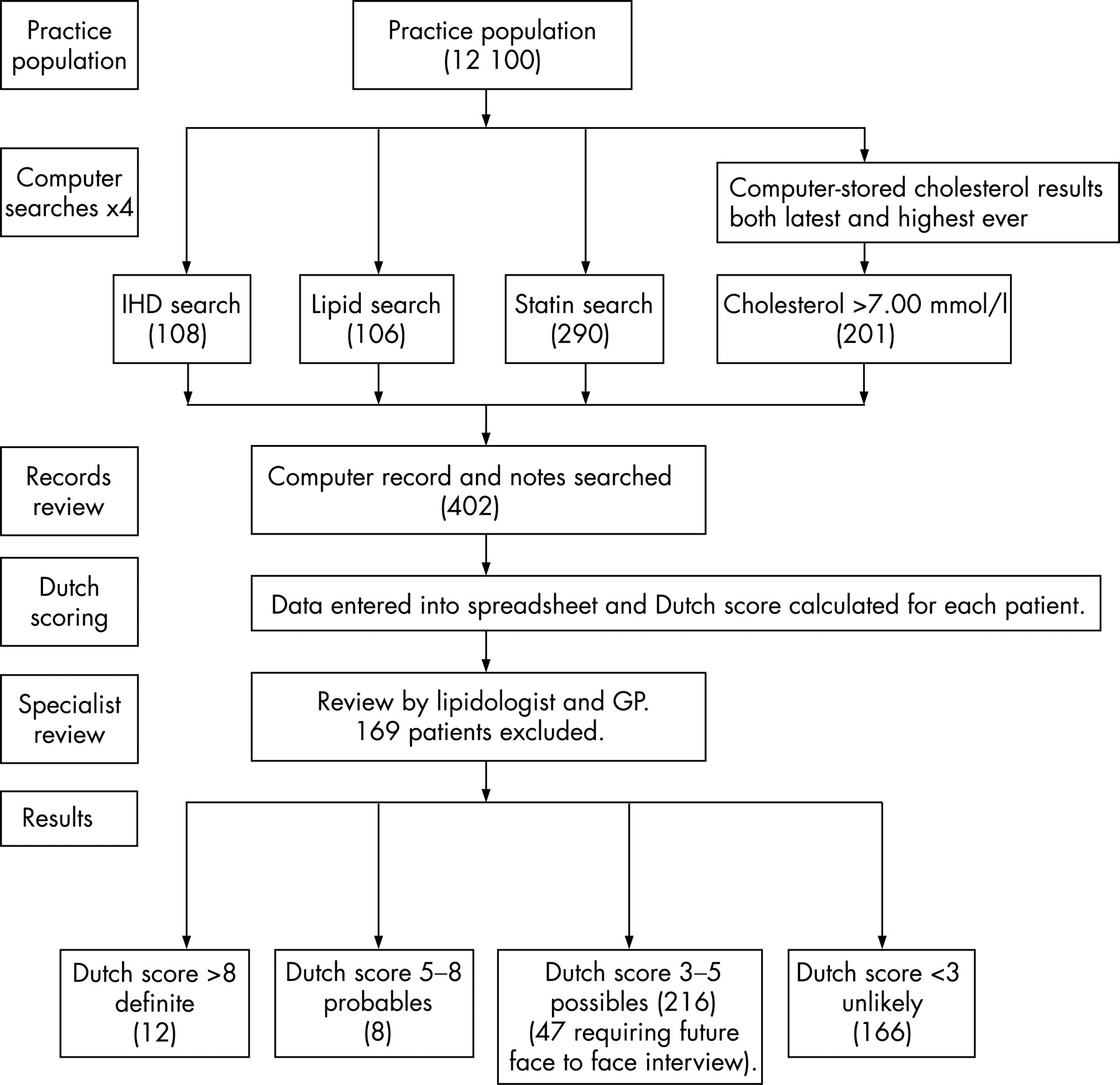
The study took place in a single primary care centre of 12 100 patients in South London. Ethical approval was deemed unnecessary by the local ethics committee as only notes searching was involved. Figure 1 outlines the method used.
{kind=link}
Four computer-based search strategies considered by the authors (JG and MM) to be the most likely to identify potential cases of FH were chosen. These were (a) the IHD search for G3 Read coded cases of “IHD”; (b) the lipid search for C32 Read-coded cases of “Lipid Disorder”, which includes FH, pure hypercholesterolaemia (PH), and mixed hyperlipidaemia; (c) the statin search for current or repeat “Statin” prescribing as defined by The British National Formulary section 3.10; and (d) the cholesterol search. The latest serum total cholesterol, and the highest ever serum total cholesterol test results were downloaded to create a highest-recorded cholesterol variable. The effect of using only a computer-based highest cholesterol was investigated, but the highest cholesterol from either the notes or the computer record was used to calculate the Dutch score for the patient. The paper and computer records for all patients retrieved in the four searches were examined for evidence of IHD, the date of onset of IHD, physical findings of tendon xanthoma, a written family history or pedigree drawing of early onset IHD (defined as onset occurring at <55 years of age in men or <60 years of age in women), pretreatment cholesterol levels, and attendance at a lipid clinic, as indicated by a hospital letter. A spreadsheet was used to calculate the Dutch score for each patient. The data were transferred to SPSS 14.0 to calculate the sensitivity, yield and number of notes needed to find one case, for the individual searches, a combined search (IHD, lipid diagnosis and statin prescription), and the combined and cholesterol >7.0 mmol/l search. A Poisson distribution statistic was used to calculate confidence limits for small samples. All cases were reviewed by the lipidologist (ASW) and a general practitioner (JG) to decide how many patients scoring between 3 and 5 (possible cases) on the available evidence could be excluded without further investigation. This decision was made on the basis of age >75 for first onset of IHD, or first statin prescription, the presence of secondary causes of hyperlipidaemia such as diabetes or hypothyroidism, or a triglyceride to cholesterol ratio of >0.5.
RESULTS
A total of 706/12 100 (5.8%) patients were identified by the four searches. Overlap of cases within the searches gave a total of 402/12 100 (3.3%) individual patients with notes to review (fig 1 and table 1).
Search results
Of 12 100 patients, 108 (0.89%) patients had IHD, including 35 with early onset IHD, 106 (0.87%) had a lipid diagnosis (subdivided in table 1 as above), and 290 (2.4%) were receiving a statin. A total of 1596 (13.2%) patients had a cholesterol test recorded on the computer and 125 (1.0%), 201 (1.7%) and 327 (2.7%) patients had a cholesterol of >7.5, >7.0 and >6.5 mmol/l, respectively.
After notes searching, 12/402 (3.0%) patients scored >8 (definite cases) and 8/402 (2.0%) patients scored between 6 and 8 (probable cases). Together these 20/12 100 (0.17%) patients give a prevalence in this practice comparable to the national estimate of 0.2% and a 95% Poisson confidence interval of 15.4 to 35.7. Two (16.7%) of the 12 definite cases and 7/8 (87.5%) of the probable cases were unknown and uncoded by the practice. Of 402 patients, 216 (53.7%) scored between 3 and 5 (possible cases). One hundred and sixty-nine patients were excluded at the clinical review stage, leaving 47/402 (11.7%) requiring face to face interview and xanthoma examination. This was not undertaken in this study.
Table 1 shows the results of both the individual and combined searches. Because of the methodology used here, the “combined and cholesterol >7 mmol/l” search gives a 100% sensitivity. So did the “cholesterol >7.0 mmol/l” search, which used data from both the notes and the computer record, but a cholesterol search based solely on the highest computer-recorded cholesterol only gives a 65% sensitivity. Statin prescription had a 90.0% sensitivity. The IHD search showed a 45% sensitivity, all in the early onset IHD group.
The proportion of patients in any one search confirmed as a definite or probable case is shown in table 1, column 6. Of the 15 patients coded as FH, 11 (73.3%) were confirmed to have FH. Early onset IHD had a 25.7% (n = 9) yield and this fell to a 5.8% (n = 20) yield for the combined search. The number of notes needed to search to find one case is shown in table 1, column 7 and ranges from 1.4 in the FH search to 20.1 in the “combined and cholesterol>7 mmol/l” search. If the exclusion criteria are applied at the computer search stage rather than at the clinical review stage the total number of notes required to search falls from 402 to 252 in the “combined and cholesterol >7 mmol/l” search at a cost of three probable cases not being discovered. The yield increases from 4.98% to 6.75% with 14.8 rather than 20.1 sets of notes examined to find one case.
Two of the 12 (16.6%) definite and 4/8 (50%) probable cases were not already known to a secondary care lipid clinic. A family history was present in the notes of 20/20 (100%) patients with definite or probable FH, but only 130/216 (60%) of possible cases of FH. This information was never of sufficient detail to construct a family tree and no drawn family pedigrees were found in the notes. A note about family screening being discussed with the patient was made in 8/12 (67%) definite cases, but no details about the process or outcome were found in any of the case notes.
Accuracy of the computer record
Patient age of IHD onset recorded on the computer did not match that shown in the written notes in 20/108 (18.5%) cases, with the notes revealing an earlier age of onset than the computer in nine cases with a maximum discrepancy of 13 years. In three cases the age difference was large enough for the patient to score additional points for early-onset IHD.
Twenty-two patients had a cholesterol of between 1 and 3 mmol/l higher in the notes than in the computer record and in another eight patients it was more than 3 mmol/l higher. Furthermore, 20 of these, six of whom were definite or probable cases, did not have a computer recorded cholesterol >7.0 mmol/l and would not have been detected using a computerised cholesterol test alone.
DISCUSSION
Principal findings
This work has established that it is possible to use note searching to define a population of patients with FH in primary care. Screening for FH in one practice of 12 100 patients identified 12 patients scoring > 8 (definite), eight patients scoring between 6 and 8, (probable), and after exclusions, 47 scoring between 3 and 5 (possible) on the Dutch scale. Of the 12 definite cases, two cases were unknown both to the practice and to the lipid clinic. Seven of eight of the probable cases were previously uncoded as FH at the practice and only 4/8 (50%) were known to the lipid clinic. Therefore, there are known and unknown cases of FH in this practice that are not known to the local lipid clinic. All of these cases are potential new index cases for any programme of relative tracing.
Table 1 shows that, in this practice, the combined search shows the highest sensitivity and yield and is independent of the cholesterol result. However, we would not recommend that the cholesterol search is ignored because there are bound to be patients in other practices whose raised cholesterol is the only pointer to the diagnosis. We therefore recommend that the “combined and cholesterol >7 mmol/l” search is used by other practices wishing to repeat this work.
Although our search strategies did identify the expected number of cases of FH given the confidence limits for this practice population and the national expected prevalence, it is highly likely that some undiagnosed cases of FH remain amongst the 47 patients we categorised as “possible” cases. These cases may be allocated additional points when a complete family history and xanthoma examination is obtained (this information is currently missing from the existing patient record), but additional patient interviews were beyond the scope of this study. A total of 402 or 3.3% of the registered practice population had their notes searched. This is a realistic number of notes on which to undertake searching given the potential health benefits to be gained. It took about half an hour to search a set of notes. This study shows that the combined and cholesterol search required 20.1 sets of notes to be searched to find one case of definite or probable FH. Using the exclusion criteria at the computer search stage rather than the lipidologist review stage improves this to 14.8 but at the cost of not detecting three probable cases.
Limitations
These findings only apply to one practice and this study needs to be repeated in a range of practices with varying disease coding qualities to see if significant differences in the yield of the different searches or coding of lipid disorders emerge. For example, if a practice is a low coding practice then the statin search may yield more cases of FH than the FH search itself. This study was not powered to distinguish between the sensitivity and yield of the different searches, and because the number of cases found in any search is low a large number of searches would have to be run to show a significant difference. Therefore, the benefit of a future larger multipractice study would be to see if yields can be maintained despite varying levels of coding across practices.
This study did not include interviewing any patients and if additional cases of FH were found these might change the conclusions as to the best search to use. The rarity of tendon xanthoma, especially at a young age, means that the family history of early onset IHD is the key to making a diagnosis of FH. This aspect of the patient record is more likely to be missing in those patients where IHD has not already occurred. The prevalence of IHD in this practice is lower than the national average because of the young age profile and low deprivation of this practice population. This might result in fewer cases of FH being found. All the patients with FH cases who also had IHD were found in the early-onset IHD group, but again the computer record on its own was not sufficient to detect all these cases owing to the inaccurate coding of age of onset of IHD on the computer. In 30 cases a higher cholesterol reading was recorded in the paper notes than on the computer records, suggesting that computer records have not captured all the available information and that computer-based cholesterol on its own is not reliable either for finding or for scoring patients. The comprehensiveness of computer records may improve in the future as all cholesterol results are transmitted directly to a computer record. At present, a comprehensive review of patient records in primary care with a view to detecting cases of FH must include the additional searches for IHD, lipid disorders and statins. Because of the large numbers involved we did not look for FH cases in the group of patients with a cholesterol reading of <7.0 mmol/l, though many of these patients will be possibles, scoring 3 on the Dutch scale simply by virtue of having a cholesterol of >6.74 mmol/l.
SUMMARY
We have established that it is possible to define a population of patients with FH in primary care. There appears to be a misunderstanding of how to make the diagnosis of FH in clinical practice: 26.7% of coded patients with FH were judged by the investigators not to have sufficient evidence in the notes to confirm a diagnosis of FH. In all cases this was because a family history of “raised cholesterol” was incorrectly taken to be synonymous with FH. It is also of considerable concern that treatment of patients with statins is being started in primary care without the realisation that the condition being treated might be FH requiring additional family screening. The failure to follow through with family screening is a possible and avoidable cause of mortality and needs to be considered more seriously. At present there is no allocated resource to do this in either primary or secondary care aside from the recent pilot work based in secondary care.11 The National Institute for Health and Clinical Excellence will shortly produce a guideline for familial hypercholesterolaemia as well as reviews of hyperlipidaemia management. Although DNA testing is not yet widely available, mutations can be found in 70% of cases of FH,18 so that DNA testing may help in the future to distinguish between cases of FH and those of polygenic raised cholesterol, especially in older age groups where the overlap in cholesterol values between the two groups is significant.
In summary, we have shown that cases of FH can be found in primary care and that it is practical to find these starting with a small number of computer searches followed by a review of the written record by researchers and experienced clinicians. Where the patient records are incomplete, face to face interviews will be required to establish a diagnosis. It might be feasible to extend this method throughout the NHS, but this work needs to be repeated in a larger sample of practices to assess the effect of variable practice coding levels and to include patient-derived information.
Acknowledgments
We thank Martin Wall, University of East London, for statistical advice.
Appendix 1
Defesche criteria
Family history
First-degree relative known with premature (men <55 years, women <60 years) coronary and vascular disease (1 point)
First-degree relative known with LDL-cholesterol >95th centile
and/or
First-degree relative with tendon xanthomata or arcus cornealis, or both (2 points)
Children <18 years with LDL-cholesterol >95th centile (2 points)
Clinical history
Patient has premature (men <55 years, women <60 years) coronary artery disease (2 points)
Patient has premature (men <55 years, women <60 years) cerebral or peripheral vascular disease (1 point)
Physical examination
Tendon xanthomata (6 points)
Arcus cornealis below age of 45 years (4 points)
Laboratory analysis
LDL-cholesterol >8.5 mmol/l; total cholesterol >10.25 mmol/l (8 points)
LDL-cholesterol 6.5–8.4 mmol/l; total cholesterol 8.25–10.15 mmol/l (5 points)
LDL-cholesterol 5.0–6.4 mmol/l; total cholesterol 6.75–8.15 mmol/l (3 points)
LDL-cholesterol 4.0–4.9 mmol/l; total cholesterol 5.75–6.65 mmol/l (1 point)
Diagnosis of FH is
Definite: >8 points; probable: 6–8 points; possible: 3–5 points.
REFERENCES
Footnotes
See Editorial, p 695
Competing interests: None declared.
Ethics approval: Deemed unnecessary as only note searching undertaken.