Article Text

Abstract
Background: Patients with similar grade diastolic dysfunction at rest may have a spectrum of alterations in diastolic function during exercise.
Objective: To evaluate (a) whether exercise could unmask further diastolic abnormalities not evident during rest; (b) whether diastolic functional reserve during exercise is associated with exercise capacity.
Methods: 141 subjects (77 male, mean (SD) age 62 (9)) with abnormal left ventricular (LV) relaxation (mitral E/A <0.75) and/or deceleration time >240 ms, underwent graded supine bicycle exercise with simultaneous respiratory gas analysis and two-dimensional and Doppler echocardiographic study. Mitral inflow and annular velocities were measured at rest and during exercise. The LV diastolic function reserve index (DFRI) was calculated.
Results: Patients were classified into two groups: group 1 (n = 64), DFRI <13.5; group 2 (n = 77), DFRI ⩾13.5. The ratio of E/E′ to stroke volume was used as an index of ventricular elastance (Ed). No significant differences between the groups in mitral inflow and annular velocities at rest were found. Mean (SD) Ed was not significantly different at rest between the groups (0.19 (0.07) vs 0.18 (0.06), p = 0.29). Ed was significantly higher during exercise in group 1 than in group 2 (25 W, 0.21 (0.09) vs 0.14 (0.04), p<0.001; 50 W, 0.22 (0.10) vs 0.15 (0.04), p<0.001). Group 1 subjects had a shorter exercise duration (8.2 (2.7) vs 9.4 (3.7) min, p = 0.04) and lower peak oxygen consumption (17.5 (4.5) vs 20.2 (5.4) ml/kg/min, p = 0.005).
Conclusions: Despite similar mitral flow and annular velocities at rest, different responses to exercise were seen in patients with abnormal LV relaxation at rest. Lower LV diastolic functional reserve was associated with higher ventricular elastance during exercise, and reduced exercise capacity.
Statistics from Altmetric.com
A reduced early (E) to late (A) diastolic filling ratio or prolonged deceleration time (DT) of E velocity reflects a slowing of left ventricular (LV) relaxation.1 This finding is the most common type of LV diastolic dysfunction in the elderly,2–4 and is believed to indicate significant diastolic dysfunction. However, many elderly subjects and patients with hypertension or LV hypertrophy have Doppler echocardiographic evidence of abnormal LV relaxation with no symptoms of heart failure at rest.3 In addition, in patients with a similar grade of diastolic dysfunction at rest, there can be a spectrum of alterations in diastolic function during exercise. Therefore, exercise could unmask diastolic abnormalities not evident under rest conditions. However, most measures to characterise LV function are obtained at rest. Recently, the assessment of diastolic function during exercise using diastolic stress echocardiography has been possible.5–8 We hypothesised that (a) in patients with abnormal myocardial relaxation at rest, a spectrum of alterations in diastolic function can exist during exercise; (b) decreased LV diastolic functional reserve is associated with an increase in ventricular elastance during exercise and (c) decreased LV diastolic functional reserve is associated with exercise intolerance.
PATIENTS AND METHODS
Study group
From January 2003 to January 2007, 947 patients were referred to the stress echocardiography laboratory for a diastolic stress test. Among them, 253 patients with abnormal LV relaxation, defined as the presence of a mitral E/A <0.75 and/or DT >240 ms, were identified. Patients with a LV ejection fraction (EF) <50% (n = 14) were excluded. Premature tachycardia during a low level of exercise made the analysis uninterpretable in 42 (17%) patients. Patients who could not exercise at a workload of more than 25 W (n = 56) were also excluded from the analysis. This left a total of 141 patients, who constituted the study group. All patients underwent a symptom-limited exercise test on a supine bicycle ergometer with simultaneous respiratory gas analysis. Study approval was obtained from the Internal Review Board of Yonsei University College of Medicine. The reason for performing an exercise echocardiography was evaluation of exertional dyspnoea in 24 patients and assessment of LV functional reserve during exercise in patients with hypertension and diabetes mellitus in 61 and 24 patients, respectively. Drugs included angiotensin-converting enzyme inhibitors, β blockers, calcium channel blockers, diuretics and angiotensin receptor blockers in 12, 34, 52, 18 and 40 patients, respectively. However, all drugs were withheld before the exercise stress test.
Resting echocardiographic examination
Standard two-dimensional measurements (LV diastolic and systolic dimensions, ventricular septum and posterior wall thickness, left atrial volume, LV outflow tract diameter) were obtained with the patient in the left lateral position. The LVEF was calculated by the modified Quinones method.9 Left atrial volume was calculated using the prolate ellipsoid model. The left atrial volume index was determined as left atrial volume divided by body surface area and reported in units of ml/m2.10 11 Stroke volume (SV) was measured from the LV outflow tract diameter and the pulse-wave Doppler signal, as previously described.12 To provide a continuous variable that might estimate ventricular elastance (Ed), the E/E′ ratio was used as an estimate of mean left atrial pressure.13–15 Operant Ed was estimated as E/E′ divided by the volume of filling during diastole (SV), assuming the absence of significant aortic regurgitation.16
Diastolic stress echocardiography5
After obtaining rest images from standard parasternal and apical views, multistage supine bicycle exercise testing was performed with a variable load bicycle ergometer (Medical Positioning, Kansas City, Missouri, USA). Patients pedalled at a constant speed, starting with a workload of 25 W. The speed was then increased by an increment of 25 W every 3 min. Echocardiography was performed using a GE Vingmed System 7 ultrasound system (GE Medical, Milwaukee, Wisconsin, USA) with a 2.5 MHz transducer during rest, each stage of exercise and recovery in the sequence described as follows. From the apical window, a 1–2 mm pulsed Doppler sample volume was placed at the mitral valve tip. Mitral flow velocities from 5 to 10 cardiac cycles were then recorded. Mitral inflow velocities were traced and the following variables were obtained: peak velocity of E and A filling and DT of the E velocity. Tricuspid regurgitant jet velocity was also obtained whenever possible to estimate pulmonary artery systolic pressure using continuous-wave Doppler imaging. Mitral annular velocity was measured by Doppler tissue imaging using the pulsed-wave Doppler mode. The filter was set to exclude high-frequency signals and the Nyquist limit was adjusted to a range of 15–20 cm/s. Gain and sample volume were minimised to allow for a clear tissue signal with minimal background noise. Early diastolic (E′) velocity of the mitral annulus was measured from the apical four-chamber view, with a 2–5 mm sample volume placed at the septal corner of the mitral annulus. These measurements were performed at baseline, at each stage of exercise and recovery in the same sequence.
All data were stored digitally and measurements were made at the completion of each study. Two-dimensional echocardiographic images from apical views at rest and during peak exercise were acquired, digitised, recorded and analysed. Both digitised and videotaped images were used for wall motion analysis. It has been shown that E′ is inversely correlated with the time constant of isovolumic relaxation (τ), and when the transmitral gradient increased, E′ is unchanged in subjects with diastolic dysfunction but increased in subjects with normal τ.17 A similar result has been shown in humans.18 Therefore, the primary mechanism for the increase of E′ during exercise may be increased sympathetic tone and resultant faster myocardial relaxation. Based on these findings, an LV diastolic function reserve index (DFRI) was calculated using a new formula as follows.
LV diastolic function reserve index = ΔE′×E′base
where ΔE′ is the change of E′ from baseline to 25 W or 50 W of exercise, E′base is early diastolic mitral annular velocity at rest.
The underlying concept for design of the new index was to express the change in E′ with exercise relative to E′ at baseline.19
Metabolic exercise testing
All patients underwent symptom-limited exercise testing on a supine bicycle ergometer with simultaneous respiratory gas analysis and blood pressure recording. Oxygen uptake, CO2 production and minute ventilation were measured using a breath-by-breath gas analysis (Medical Graphics, St Paul, Minnesota, USA). A 12-lead electrocardiogram was continuously registered to exclude significant myocardial ischaemia, and blood pressure was recorded every 3 min with a cuff sphygmomanometer. Peak oxygen consumption (Vo2) was defined as the mean of the highest values obtained over the last 10 s of exercise.
Statistical analysis
Continuous variables were summarised as a mean (SD). Categorical variables were summarised as a percentage of the group total. An unpaired Student t test and χ2 analysis were used to compare continuous and categorical variables, respectively. All p values reported in the text are two sided. Significance was defined as p<0.05. Owing to the exploratory nature of the study, no adjustment was made to the significance level for the multiplicity of testing.
RESULTS
Table 1 presents the clinical characteristics of the study group.
None had echocardiographic or electrocardiographic evidence of myocardial ischaemia at rest; five (3.5%) had echocardiographic evidence of ischaemia during exercise. The median DFRI at 50 W was 13.5. Patients were classified into two groups: group 1 (n = 64), DFRI <13.5 and group 2 (n = 77), DFRI ⩾13.5. There were no significant differences in age, gender, height, weight, body surface area, history of smoking, hypertension and hypercholesterolaemia between the groups. Diabetes mellitus was more common in patients with a lower DFRI (table 2).
Baseline echocardiographic characteristics
LV size, EF and left atrial volume index were similar between the groups. However, LV mass index was significantly higher in patients with a lower DFRI. There were no significant differences in mitral inflow velocities (E, A, E/A, DT) between the two groups. E′ and E/E′ were also similar between the groups. E′, a surrogate of myocardial relaxation, was <0.1 m/s in all patients (mean (SD) 0.05 (0.01) m/s), further supporting the presence of impaired myocardial relaxation in this study group. Tricuspid regurgitation velocity at rest did not differ significantly between the groups (table 3).
Exercise haemodynamic changes
Leg fatigue was the most common cause for stopping the exercise—in 80/141 patients. Forty-three patients stopped exercise, with dyspnoea as the primary reason. Nineteen (30%) of 64 patients of group 1 and 24 (31%) of 77 patients of group 2 stopped exercise owing to dyspnoea. Heart rate, systolic blood pressure and diastolic blood pressure increased in both groups during exercise in comparison with those at rest. However, no significant differences were seen in the changes of systolic and diastolic blood pressures at rest or during exercise between the groups. Heart rate during exercise was lower in patients with lower diastolic function reserve, although this difference was not significant (table 4).
However, exercise duration was significantly shorter in patients with a lower DFRI than in patients with a higher DFRI (8.2 (2.7) vs 9.4 (3.7) min, p = 0.04). Peak oxygen consumption (Vo2) was also significantly lower in patients with a lower DFRI than in those with a higher DFRI (17.5 (4.5) vs 20.2 (5.4) ml/kg/min, p = 0.005) (table 4). This finding suggests a lower exercise capacity in patients with lower diastolic functional reserve. There were no significant differences in mitral inflow velocities (E, A, E/A, DT) during exercise between the two groups (table 5).
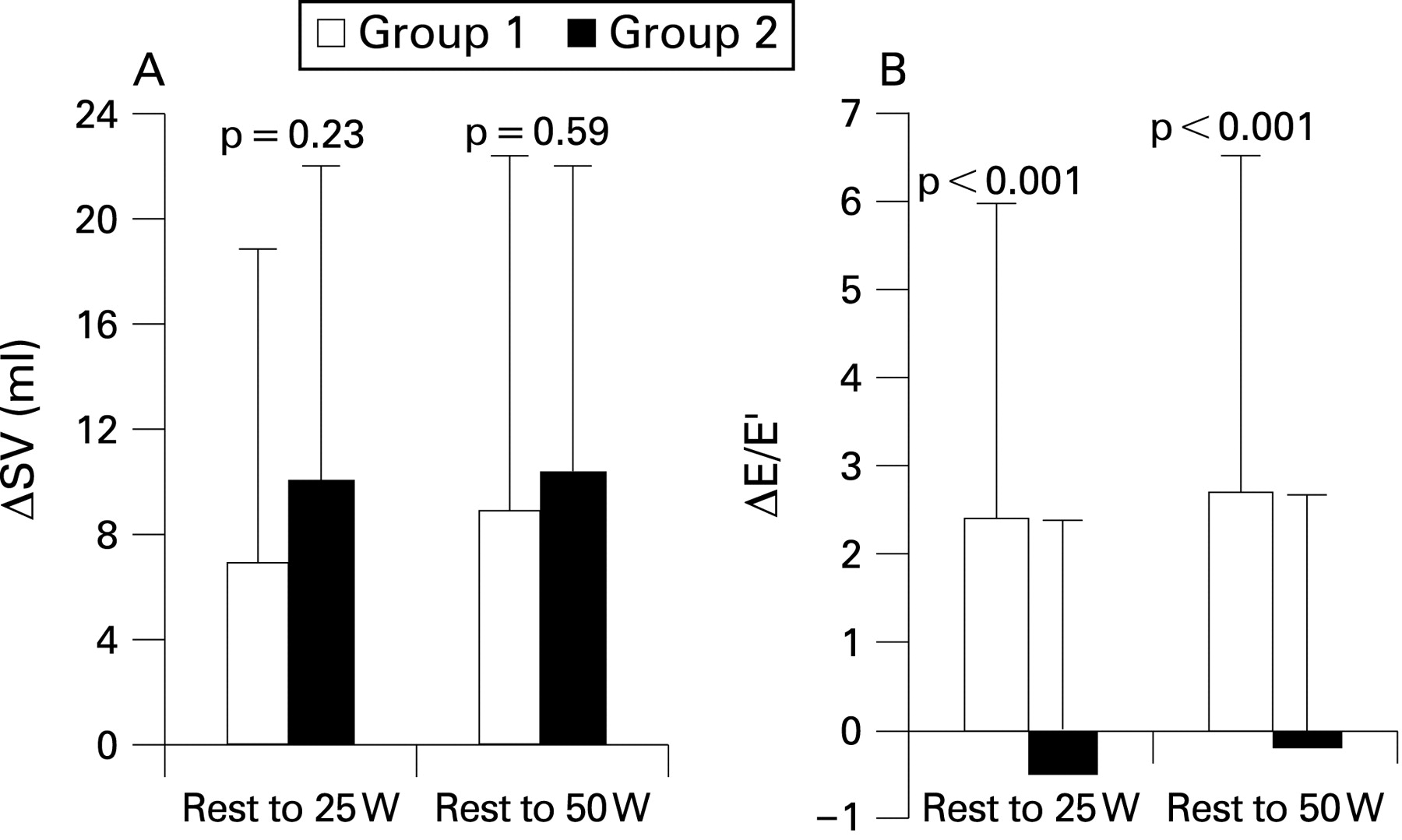
At rest, E/E′ did not differ significantly between the groups (12.5 (4.0) vs 11.4 (3.6), p = 0.10). However, during exercise E/E′ became significantly higher in patients with a lower DFRI than in patients with a higher DFRI (25 W, 14.8 (4.7) vs 10.9 (2.8), p<0.001; 50 W, 15.2 (4.4) vs 11.1 (2.9), p<0.001) (fig 1). In addition, the magnitude of change in E/E′ from rest to exercise was significantly higher in the group with lower DFRI (from rest to 25 W, 2.4 (3.6) vs −0.5 (3.0), p<0.001; from rest to 50 W, 2.7 (3.9) vs −0.2 (3.0), p<0.001) (fig 2B). However, SV at rest and during exercise were similar between the groups. The magnitude of change in SV from rest to exercise was also similar between the groups (from rest to 25 W, 6.9 (12.8) vs 10.0 (12.5) ml, p = 0.23; from rest to 50 W, 8.9 (14.1) vs 10.4 (11.8) ml, p = 0.59) (fig 2A).


For LV diastolic elastance, Ed was not significantly different between the groups at rest (0.19 (0.07) vs 0.18 (0.06), p = 0.29). However, during exercise Ed became significantly higher in patients with lower DFRI than in patients with higher DFRI (25 W, 0.21 (0.09) vs 0.14 (0.04), p<0.001; 50 W, 0.22 (0.10) vs 0.15 (0.04), p<0.001) (fig 3).

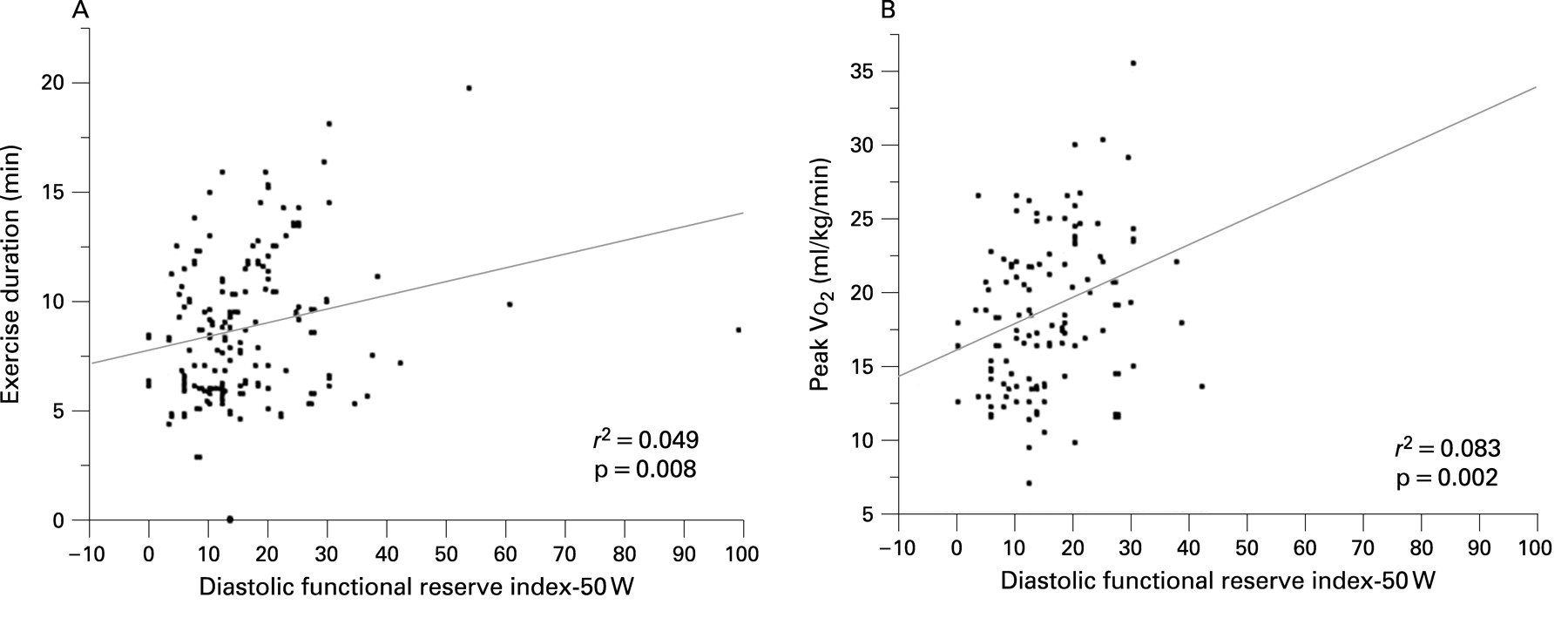
There was no significant correlation between age, LV end-diastolic and end-systolic dimensions, EF, left atrial volume index and DFRI (age, r = 0.09, p = 0.30; LV end-diastolic dimension, r = 0.1, p = 0.21; LV end-systolic dimension, r = 0.1, p = 0.22; EF, r = −0.04, p = 0.56; left atrial volume index, r = 0.14, p = 0.14). None of the conventional Doppler indices (E, A, E/A, DT) correlated with DFRI (E, r = −0.01, p = 0.87; A, r = −0.008, p = 0.93; E/A, r = 0.03, p = 0.66; DT, r = 0.13, p = 0.13). However, DFRI was significantly correlated with E′ (r = 0.33, p<0.001), E/E′ (r = 0.2, p = 0.018), peak VO2 (r2 = 0.083, p = 0.002) and exercise duration (r2 = 0.049, p = 0.008) (fig 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
DISCUSSION
The principal findings of this study are that (a) despite a similar grade of diastolic dysfunction (impaired myocardial relaxation) at rest, a wide spectrum of alterations in diastolic function can be seen during exercise; and (b) this difference translates into physiological significance. In patients with lower diastolic functional reserve, LV becomes stiffer with exercise. In addition, exercise duration and peak Vo2 were significantly lower than in those with higher diastolic reserve. To our knowledge, this is the first study to demonstrate that exercise-induced changes in diastolic function, despite similar degrees of diastolic dysfunction at rest, are important physiologically. These results emphasise the importance of assessing diastolic functional reserve in patients with abnormal LV relaxation at rest.
Impaired myocardial relaxation is the most common type of LV diastolic dysfunction and it is recognised as an early manifestation in the spectrum of diastolic abnormalities. However, because of its ubiquity, this abnormality is often recognised as an incidental finding. In fact, most people with impaired relaxation do not have symptoms or signs of heart failure at rest.3 This is because increased LV filling pressure is unusual in the absence of systolic dysfunction or comorbidities such as myocardial infarction or hypertensive heart disease.20 However, exertional dyspnoea is quite common in these patients and therefore impaired relaxation is suggested as a precursor to overt heart failure.3 If this is the case, symptoms of heart failure should be unmasked during exercise in patients with this abnormality. However, it is not yet known whether impaired LV relaxation leads invariably to higher LV filling pressure during exercise. In this study, we found that patients with impaired myocardial relaxation and normal EF at rest exhibit a wide spectrum of alterations in diastolic function during exercise. Interestingly, patients with lower diastolic functional reserve had greater ventricular stiffness with exercise, higher LV filling pressures during exercise and showed lower exercise capacity. These findings underline the importance of assessing diastolic functional reserve in patients with abnormal LV relaxation at rest to further stratify their functional capacity.
In our study, diabetes was more common in patients with a lower DFRI. Impaired myocardial relaxation is an important hallmark of the myocardial response in diabetic and hypertensive heart disease. Diabetes mellitus is an important cause of heart failure21 and the prognosis of diabetic patients with heart failure is worse than that of patients without diabetes.22 23 Many epidemiological and clinical trials have shown that diabetes is commonly associated with heart failure presenting with a normal EF. From the results of this study, it can be speculated that despite similar resting diastolic functional measures, patients with diabetes may be more prone to develop significant diastolic dysfunction with exercise than non-diabetic subjects. Therefore, the results of this study can partially explain the higher incidence of heart failure with normal EF and worse clinical outcome in patients with type 2 diabetes. In addition, LV mass index was significantly higher in patients with a lower DFRI, although blood pressure at rest and during exercise were similar and their histories of hypertension did not differ significantly. These findings underline the importance of a structural substrate that contributes to exercise-induced deterioration of diastolic function.
During exercise, the increased cardiac output is achieved by an LV SV either maintained or increased concomitantly with an increase in heart rate. Because tachycardia decreases the duration of diastole, there is less time for diastolic filling of the left ventricle. Thus, the mean mitral flow rate must increase during exercise to maintain or augment SV. This can be achieved by faster relaxation and an augmented suction effect induced by higher sympathetic tone during exercise.24 25 However, in patients with diastolic dysfunction the abnormal relaxation prevents augmentation of relaxation as the heart rate increases during exercise.26–28 Previous work has shown that marked abnormalities in LV diastolic function may occur with exercise in patients with clinical evidence of heart failure and a normal resting systolic function.29 The cause of exercise intolerance in some patients with LV failure is diminished cardiac output, so that inadequate oxygen is delivered to working skeletal muscle to meet the demands of aerobic metabolism. However, in other patients exercise intolerance is due to a rise in pulmonary capillary wedge pressure, resulting in marked dyspnoea.29 From the results of this study, an increase in LV filling pressure rather than abnormal SV response may be a more important haemodynamic contributor during low level supine exercise in patients with impaired relaxation at rest.
Study limitations
There are obvious limitations using the decreased mitral E/A ratio and prolonged DT as surrogate markers of LV relaxation abnormality; but this simple non-invasive assessment is well accepted and integrated into our day-to-day clinical evaluation of diastolic function. In addition, E′, a surrogate of myocardial relaxation, was <0.1 m/s in all patients (mean (SD) 0.05 (0.01) m/s), further supporting the presence of impaired myocardial relaxation in this study group. The association between LV diastolic functional reserve and LV diastolic elastance may not be surprising since E′ was used to calculate both variables. It would be more accurate to calculate LV diastolic elastance using invasive haemodynamic measurement, although it is not practical especially during exercise. Recently, Westermann and colleagues conducted a study using an invasive pressure–volume loop approach and measured cardiac function at rest and during atrial pacing and handgrip exercise and showed that increased ventricular stiffness was seen in patients with heart failure with a normal EF at rest.30 Furthermore, increased stiffness was associated with increased end-diastolic pressures during handgrip exercise and with decreased stroke volume and a leftward shift of pressure–volume loops during atrial pacing. The recruitment of patients might have been affected by selection bias because our study group comprised patients referred for a diastolic stress test. There were no specific factors for the recruitment of patients in this study. Owing to limited number of patients referred for a diastolic stress test, we analysed the data of all available patients.
Clinical implications
Most patients with chronic heart failure do not have symptoms at rest but, rather, develop symptoms of dyspnoea with exertion. However, the majority of measures used to characterise LV function are obtained at rest. Because alterations in diastolic function during exercise are quite variable in patients with abnormal relaxation, it may be important to assess haemodynamic performance during some forms of stress, especially exercise. This could unmask further diastolic abnormalities despite similar diastolic dysfunction at rest. Moreover, to better understand the pathophysiology of patients with impaired relaxation at rest, assessment of haemodynamic performance during exercise would be more revealing. Therefore, the current findings might be particularly useful in further risk stratification in patients with abnormal myocardial relaxation.
CONCLUSION
In this study, we found that patients with preserved LV systolic function and impaired myocardial relaxation at rest exhibit a wide spectrum of alterations in diastolic function during exercise. Patients with lower diastolic functional reserve had greater ventricular stiffness during exercise and demonstrated a lower exercise capacity.
REFERENCES
Footnotes
-
Funding: This work was supported by the Korea Science and Engineering Foundation (KOSEF) grant funded by the Korean government (M10642120001-06N4212-00110).
-
Competing interests: None.
-
Ethics approval: Ethics committee approval obtained.