Article Text

Abstract
Objective: To obtain a “snapshot” view of access-specific percutaneous cardiovascular procedures outcomes in the real world.
Design: Multicentre, prospective study performed over a 30-day period.
Setting: Nine hospitals with invasive cardiology facilities, reflecting the contemporary state of healthcare.
Patients: Unselected consecutive sample of patients undergoing any percutaneous cardiovascular procedure requiring an arterial access.
Interventions: Percutaneous cardiovascular procedures by radial or femoral access
Main outcome measures: The primary outcome was the combined incidence of in-hospital (a) major and minor haemorrhages; (b) peri-procedural stroke; and (c) entry-site vascular complications. The secondary outcome was the combined incidence of in-hospital death and myocardial infarction/reinfarction. For analysis purposes, outcomes were allocated to arterial access-determined study arms on an intention-to treat basis. Multivariable analysis adjusted using propensity score was performed to correct for selection bias related to arterial site.
Results: A total of 1052 patients were enrolled: 509 underwent radial access and 543 femoral access. In both groups, 40% underwent a coronary angioplasty. Relative to femoral access, radial access was associated with a lower incidence both of primary (4.2% vs 1.96%, p = 0.03, respectively) and secondary endpoints (3.1% vs 0.6%, p = 0.005, respectively). Multivariate analysis, adjusted for procedural and clinical confounders, confirmed that intention-to-access via the radial route was significantly and independently associated with a decreased risk both of primary (OR 0.37, 95% CI 0.16 to 0.84) and secondary endpoints (OR 0.14, 95% CI 0.03 to 0.62).
Conclusions: Our study indicates strikingly better outcomes of percutaneous cardiovascular procedures with radial access versus femoral access in contemporary, real-world clinical settings.
Statistics from Altmetric.com
In the recent years, invasive cardiology has gained a pivotal role in the management of acute and stable heart disease by improving outcomes and/or quality of life. Accordingly, the use of percutaneous cardiovascular procedures is increasing worldwide and, as a consequence, procedural complications are also rising, becoming a major health concern. Particularly, procedure-related bleedings have been associated with an unfavourable in-hospital and long-term prognosis.1 2 Several strategies have been tested to reduce haemorrhages, including new drugs and new technical strategies such as the use of radial artery access. In fact, because radial artery catheterisation has been associated with a significant reduction in the rate of access-site complications and in the rate of access-site-related haemorrhage compared to femoral artery catheterisation, any reduction in bleeding by means of radial access could have a positive effect on general outcome.3–7
Nevertheless, the reported reduction in complications with the radial approach may be biased by the inherent limitations of clinical trials, so that the same results might not be observed in real-world clinical settings. Indeed, previous randomised studies have been designed to identify radial access advantages over femoral access, when used by highly motivated and experienced operators, mainly in small populations or in single centres. Larger observational studies investigated arterial approach-related outcomes by analysing prospective registries focused on interventional procedures. However, these analysis have been perfomed retrospectively and/or using databases built for other purposes; therefore, the control of confounders could have been insufficient to draw any final conclusion.5–7 Additionally, all these studies spanned many years, and have involved different ways of classifying bleeding, often rendering difficult any generalisation of results to contemporary interventional cardiology, where recent advances in treatment have rapidly modified outcomes.8
Hence, to date, no large observational study has been specifically designed to control for possible confounders and appraise arterial access-related clinical outcomes across different centres and with different operators after both interventional and diagnostic procedures. Therefore, in order to assess if the contemporary use of the radial approach translates into real-world benefits as previously suggested, we designed a prospective multicentre study to be performed over a short period of time in a large unselected population of consecutive patients, using specific definitions of “bleeding”.
METHODS
The study was performed between 1 June and 30 June 2006 in the Lazio region, the second most populated region of Italy with over five million inhabitants. To recruit centres, an invitation letter was sent to all 22 hospitals with catheterisation laboratory facilities in the region. Sixteen hospitals responded, among whom nine centres were selected. These nine centres represent the state of healthcare in Italy and across the region as, according to 2005 official records, they contributed 54% of the cardiovascular interventional activity that took place in the Lazio region.9 Three of the centres were considered to be high-volume centres, with respect to these procedures (>2000 procedures/year); three were moderate-volume centres (between 1000 and 2000 procedures/year); and three were low-volume centres (<1000 procedures/year). A questionnaire asking about procedural activities had been distributed and completed by all participating centres before the enrolment phase. (The overall characteristics of the hospitals and operators are given in appendix table 1.)
All consecutive patients who underwent an invasive procedure requiring an arterial access in the catheterisation laboratory were included in the study. Patients were excluded if they were enrolled in other research protocols requiring specific therapy or a specific arterial access site. The choice of arterial access site and the technique employed was made by individual practitioners based upon their usual practice. Where required, the protocol was approved by the local hospital ethics committee, and informed consent was obtained from all patients.
Data regarding percutaneous coronary procedures were collected prospectively using a case report form, and thereafter transferred into an electronic database. Data consistency was assured by (a) random inspection of data accuracy, performed by the principal investigator throughout the study (in >20% of individual case report forms), and by (b) continuously correcting database errors (before its locking) by cross-checking data consistency between the database manager and the primary investigator at each centre.
In order to assess the global puncture-related safety of each access-site choice, the primary composite study outcome was defined as the combined incidence of the following in-hospital complications: (a) puncture-related bleeding; (b) pseudoaneurysms and arteriovenous fistulas requiring treatment (that is, compression and/or surgery); and (c) stroke. A haemorrhage was classified as “major” if any one of the following events occurred: retroperitoneal haematoma and/or death; a requirement for surgical intervention (vascular closure or local compartment decompression); a requirement for blood transfusion; a fall in haemoglobin concentration >4 g/dl; or a local haematoma involving >50% of the affected limb’s surface area, as determined by visual inspection, and being associated with severe patient discomfort and a prolonged hospital stay. In the absence of major bleeding criteria, a haemorrhage was classified as minor if associated with any of the following events: a fall in haemoglobin concentration ⩽4 g/dl, or any local haematoma involving ⩽50% of the affected limb’s surface area, as determined by visual inspection, and/or not being associated with severe patient discomfort and a prolonged hospital stay. These definitions have been recently published and were adopted according to recent considerations on the subject, which stressed the need for wide definitions of bleeding not to underestimate the incidence of clinically significant haemorrhages.4 10 11
The secondary outcome was the combined incidence of post-procedural, in-hospital (a) death; (b) myocardial infarction; and (c) myocardial re-infarction. Myocardial infarction was defined as an in-hospital event that was not the indication of the index procedure, associated with new diagnostic Q waves in two or more contiguous ECG leads and/or an elevation of creatine kinase myocardial band isoenzyme (CK-MB) levels three or more times the upper level of normal (ULN) within 36 hours of the procedure, or two or more times the ULN beyond this time limit. Re-infarction was defined as a recurrence of ST-segment elevation and/or any new significant Q wave and/or the occurrence of any increase in CK-MB levels above the last value, associated with recurrent symptoms.
Statistical analysis
Unless otherwise specified all study data were analysed on an intention-to-treat basis, thereby assigning each subject to the first arterial access site chosen by the relevant operator.
Continuous variables for each of the two subject groups, femoral and radial access, were reported as mean (SD); categorical variables were reported as the absolute number and percentage. Continuous variables were compared using independent-sample Student t or Mann-Whitney U tests, where appropriate. Categorical variables were compared by means of Pearson’s χ2 analysis or Fisher’s exact test, where appropriate. Multivariable binary logistic regression analysis was performed to appraise the independent predictive role of access site on the study outcomes, selecting variables for the final multivariable model using a backward stepwise algorithm. These results are reported as odds ratios (OR) with associated 95% confidence intervals (CI). To further account for baseline differences between the radial and femoral access groups, a non-parsimonious propensity analysis was performed, using a propensity score as a covariate in the logistic regression model, testing for its discrimination by means of a receiver operating characteristic (ROC) curve.12 13 This propensity score had evident discriminatory ability (the area under the ROC curve was 0.86 (95% CI 0.84 to 0.88)). (The variables used to build the multivariate model and the propensity score are showed in appendix table 2.)
ROC analysis was also performed for an exploratory evaluation of the best cut-off point of activity volume by radial access of each operator to predict primary and secondary endpoints.
To estimate the sample size required for the study, a priori, we assumed (a) that the combined incidence of the primary complications would be 5% among those in whom femoral access was performed; (b) a 0.20 odds ratio in the radial approach arm; and (c) an overall ratio of one radial access to every three femoral access procedures. Applying these assumption, we estimated that 860 patients would be necessary to detect a statistically significant difference between the radial and femoral approach with 80% power and an α error of 5%. Based upon official Italian interventional data for each of the nine participating centres, we calculated that four weeks would be necessary to complete the study, taking into account the potential for a 20% monthly variation of each hospital’s interventional activity relative to the official records.
A p value of <0.05 was considered statistically significant, with all reported p values two-tailed. Statistical analysis was performed using SPSS version 11.5.
RESULTS
Patients and procedural characteristics
Over the one month of observation, 1052 patients were enrolled (22% more than the sample size required), with 543 undergoing femoral access and 509 undergoing radial access. The clinical and procedural characteristics of the patients are listed in table 1.
Patients receiving radial artery catheterisation were more often males. The clinical presentation was more often stable angina pectoris in the radial than in the femoral access group, while the latter were more likely to have presented with an acute coronary syndrome. However interventional procedures were performed in a similar proportion of patients in the radial and femoral approach groups. Moreover, patients undergoing radial access had a trend towards a higher prevalence of coronary multivessel interventions, while the PCI success rate was similar in the radial and femoral approach groups. Despite these facts, patients who underwent radial access had, on average, a higher heparin dosage, smaller sheath size and more frequently underwent the administration of glycoprotein IIb/IIIa inhibitors than those in the femoral access group.
The average procedure duration, amount of administered dye and number of catheters used in each procedure were similar in the two study groups, even though patients undergoing radial artery access more often needed repeated arterial access than patients who underwent femoral access The femoral access group more often had closure devices than patients in the radial access group, as expected.
Primary and secondary outcomes
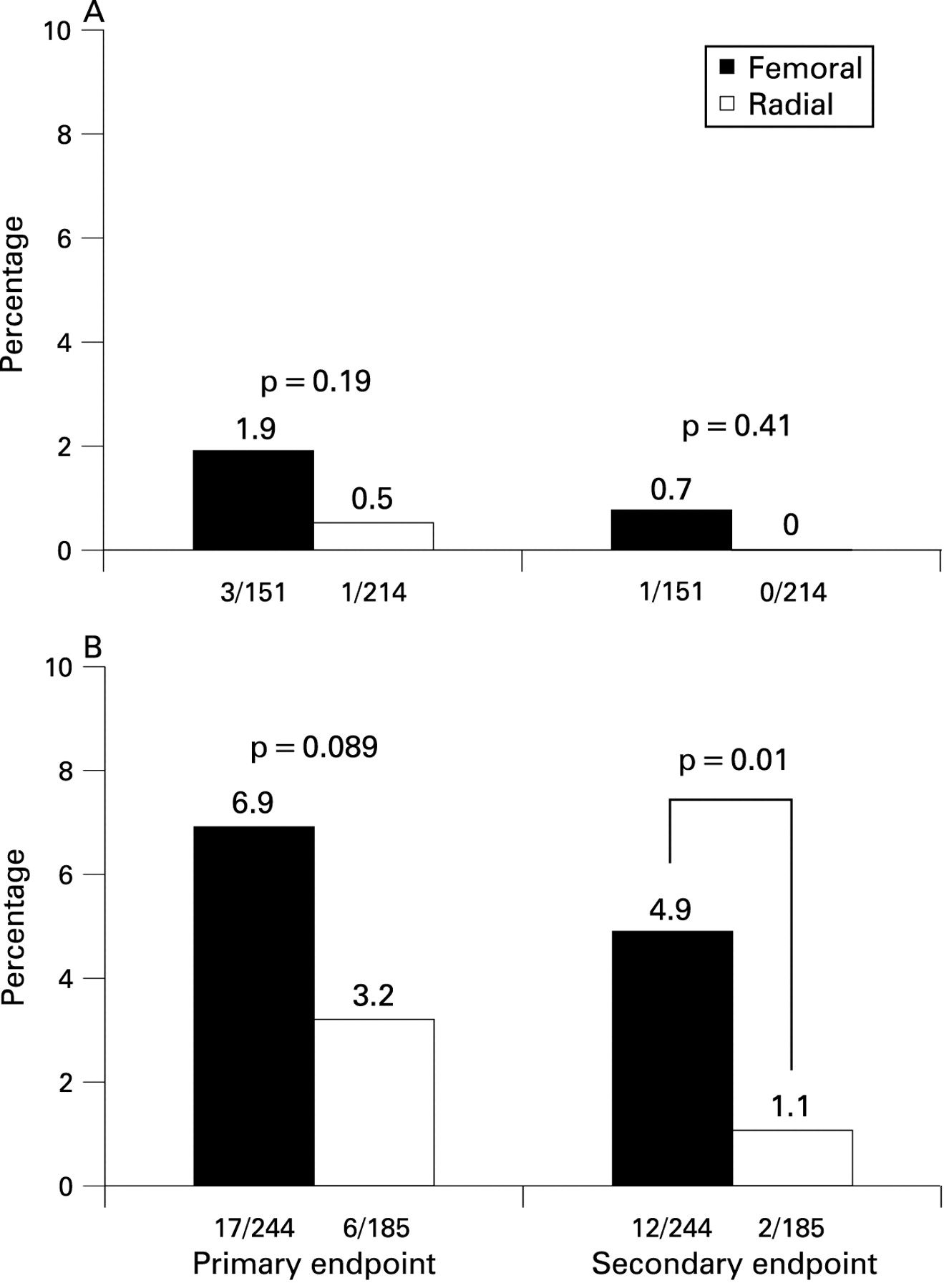
Intention-to-access via the radial artery carried a statistically significant lower incidence of primary endpoint than via the femoral artery. However, the two study groups were similar with respect to individual complications (fig 1). Interestingly, one major and one minor bleed in the radial access group were caused by femoral haemorrhages that occurred after crossover to femoral access. Indeed, when a per-treatment analysis was performed there was a statistically significant lower bleeding rate in radial compared to femoral access group (6/483 patients (1.2%) vs 19/569 patients (3.4%), p = 0.04, respectively). Multivariate logistic regression analysis results are given in table 2. Intention-to.access via the radial artery was independently associated with a lower risk of primary complications.

Secondary endpoint was significantly less frequent in the radial approach group, according to an intention-to-treat analysis. Upon breakdown analysis, a statistically lower incidence of in-hospital infarction or reinfarction was observed among the radial access patients, and a trend towards less frequent death was also observed in the radial access group (fig 2). Of note, one death in the femoral access group was caused directly by arterial access complications. Multivariate analysis results are shown in table 3. Intention-to-access via the radial artery was associated with a significant reduction in in-hospital death or myocardial infarction.

(The description of the characteristics of the patients with a primary complication or an ischaemic complication are given in appendix tables 3 and 4.)
As radial approach-associated outcome advantages may have been influenced by the selection of the patients with chronic stable angina to undergo radial access while acute patients more often underwent the femoral approach, we separately assessed the relative incidence of primary and secondary endpoints in these two subgroups. We found that the statistically significant outcome benefit of the radial approach was mainly observed in acute patients (fig 3).

Moreover, at non-parsimonious propensity analysis-adjusted logistic regression analysis, we found that intention-to-access via the radial route was associated with a significantly lower risk of both primary and secondary endpoints (fig 4). Testing this model for non-pre-specified outcomes, we could not identify any significant differences between the two groups in terms of the risk for major bleeding, minor bleeding, any bleeding, death and infarction/reinfarction.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Operator characteristics and study outcomes
On multivariate analysis, no significant associations were detected between all outcomes and the volume of interventional activity at each centre, and both the total activity volume or the activity volume by radial approach of each operator in the year before the study. With ROC analysis, no threshold for the propensity to perform radial access (as assessed by the percentage of cases performed via the radial artery by each operator during the study) was identified that predicted the incidence of either primary (area under the curve by extended trapezoidal rule: 0.61 (95% CI 0.51 to 0.71)) or secondary outcomes (0.53 (95% CI 0.39 to 0.67)).
Overall, the access site had to be changed in 6.5% of patients (table 1). However, patients whose radial access was done by operators who performed the radial approach more than 50% of the time were less likely to require an alternative arterial access site than patients whose radial catheterisation was performed by operators with a lower propensity to choose the radial approach (21/459 (4.6%) patients vs 12/49 (24.5%) patients; p<0.0001).
DISCUSSION
The PREVAIL study showed a statistically significant association between the use of the radial approach in the real world and both an improved access site-related procedural safety and a reduced incidence of in-hospital “hard” endpoints after unselected percutaneous cardiovascular procedures.
We believe that this study is the first multicentre, prospective study of consecutive patients specifically providing insight into how radial and femoral approaches compare in contemporary clinical cardiology practice. Other advantages of this study over previous research are that the study involved intention-to-treat analysis, a wide array of diagnostic and interventional procedures, a very limited time frame and a high variability in radial access rate among the centres.
In our study, despite an overall lower than expected incidence of primary endpoint, the use of the radial approach was still associated with an independent, risk-adjusted, statistically significant 63% reduction in risk, relative to the femoral approach.
However, the impossibility of detecting any statistically significant difference in haemorrhage rate (a post-hoc breakdown in our study) when intention-to-treat analysis was employed, may be related to the average expertise of the operators, because it is well known that the radial approach has a long learning curve.3 Indeed, in the PREVAIL study, the overall access site crossover rate with the radial approach was 6.5%, which compares well with the 7.2% average procedural failure reported in a recent meta-analysis that combined studies involving operators with a broad range of expertise, but it was higher than the 3.9% observed in a recent large observational study performed at a single centre, at which radial access was performed in a high percentage of cases.3 4
In the PREVAIL study, only one patient experienced a procedure-related stroke, in the femoral access group.
We did show, for the first time to our knowledge, a 86%, clinical and procedural variables-adjusted, intention-to-treat reduction in the risk of in-hospital death or infarction/reinfarction in patients undergoing any percutaneous cardiovascular procedures by the radial approach.
Albeit, probably on a per-treatment rather than intent-to-treat basis and without any adjustment for baseline characteristics, similar results recently have been reported from the RIVIERA trial, a large multicentre observational study aimed at other study endpoints and performed in patients exclusively undergoing elective or primary PCI.6 The MORTAL study, in a retrospective evaluation of a prospective database of patients solely undergoing PCI, also showed a significant reduction in the risk of death at 30 days and one year by the radial approach, although probably on a per-treatment analysis.7 However the latter results were analysed with incomplete procedural data for a thorough control of confounders and without considering any ischaemic endpoint.7
The interpretation of our results is uncertain. Of course biases related to an observational study are present in the PREVAIL study. However the benefit of radial access was confirmed on multivariate analysis, even when adjusted for a propensity score with good discriminatory ability. Moreover the fact that the highest baseline risk patients (such as those with acute coronary syndromes or STEMI) contributed mostly to the observed outcome benefit by the radial approach, suggests that the influence of this selection bias could be less relevant in this study. As also supported by another study, one possible explanation may be that radial approach may influence outcome by reducing bleeding rates.7 However, this effect may also induce operators to use more liberal doses and combinations of anticoagulant and anti-platelet therapies, thereby possibly achieving a simultaneous better efficacy on anti-ischaemic targets, a conjecture confirmed by the higher mean heparin dosage and the more frequent use of glycoprotein IIb/IIIa inhibition utilised in the radial approach arm despite the lower observed prevalence of acute coronary syndromes in this group of patients.14 Indeed patients with an ischaemic complication after the index procedure (mainly after acute coronary syndromes and femoral approach) showed a trend towards a lower heparin dose than in acute coronary syndrome controls via the radial route (appendix fig 1). This hypothesis also may partially explain the neutral results observed in older randomised studies, the vast majority of which were performed in stable patients and before the most recent advances in anticoagulant and anti-platelet therapy.3 Moreover, reducing the duration of bed rest, given that prolonged bed rest itself is associated with a worse prognosis in heart disease, may be another mechanism by which the radial approach improves patient outcomes.15–17 Given the non-randomised nature of this study, specifically designed randomised studies are warranted to confirm and explain our results.
Finally, with respect to procedure feasibility, in the PREVAIL study the two groups were similar in the procedure length, fluoroscopy time, amount of administered dye and number of catheters used, and the expertise of the operators and the volume of activity of each centre did not influence the study outcomes.
In conclusion, our study was able to show that, in contemporary real-world practice, a cheap and simple technical variation such as radial approach was globally associated with significantly lower peri-procedural risk than the femoral approach, also improving the incidence of ischaemic endpoints probably by safely increasing anti-platelet and anticoagulant doses to optimally prevent myocardial ischaemia. Moreover, the use of radial access in unselected percutaneous cardiovascular procedures, is feasible and yields good results, even when performed by less experienced operators at low procedural volume hospitals.
Finally, our data show that, because the advantages we observed were detectable in a community in which fewer than half of catheterisation procedures are via radial access, additional improvements in the outcomes of percutaneous cardiovascular procedures should be expected with further use of the radial approach. This could translate into community reductions in adverse events and, consequently, monetary savings to the health-care community at large.
Limitations of the study
This study has all the limitations of an observational trial, in which adjustments to compensate for potential confounders are always incomplete. It is possible that variables not included on the case report forms may have influenced the final results of the study, making the arterial site nothing more than a surrogate of some other clinical factor(s). In particular, we did not systematically assess either the left ventricular function or appropriate elements to calculate any clinical risk score, two important prognostic factors. Moreover, the finding that more men and more stable patients underwent radial procedures and the inclusion of two cardiogenic shock patients does represent a bias in the study. None the less the study was designed to specifically eliminate or minimise the effects of a number of pre-specified possible confounders, especially via the use of multivariate analysis and propensity adjustment. Furthermore, the acute coronary syndrome patients were considered separately to address this specific issue and the exclusion of the two shock patients from statistical analysis did not change any study result (data not shown).
Acknowledgments
The PREVAIL study group is aknowledged in the appendices section online.
We are indebted to Stefano Bonassi, MD, for his help in the statistical analysis and to Antonella Giornetti for her invaluable management of the study.
REFERENCES
Supplementary materials
web only appendices 95/6/476
Files in this Data Supplement:
Footnotes
Appendices are published online only at http://heart.bmj.com/content/vol95/issue6
Funding: None.
Competing interests: None.