Article Text

Abstract
Objective: To explore if hypoglycaemic episodes during hospitalisation influence the subsequent prognosis in patients with diabetes and acute myocardial infarction.
Design, setting and patients: Within the framework of the clinical trial DIGAMI 2 hypoglycaemic episodes (blood glucose <3.0 mmol/l with or without symptoms) were recorded in 1253 patients (mean age 68 years; 67% males) with type 2 diabetes and myocardial infarction. The patients were followed during a median of 2.1 years. A total of 947 patients were randomised to an initial insulin infusion while 306 received routinely used glucose lowering therapy.
Main outcome measures: Unadjusted and adjusted (age, sex, smoking, previous infarction, heart failure, renal function, diabetes duration, coronary interventions, pharmacological treatment and B-glucose at hospital admission) hazard ratios (HR) and 95% confidence intervals (CI) for total mortality and cardiovascular events (death, re-infarction or stroke) were related to hypoglycaemic episodes during the index hospitalisation.
Results: During the first 24 hours hypoglycaemic episodes were noted in 111 (12%) insulin-treated (symptomatic 23%) and three (1.0%) routinely treated patients (symptomatic 33%). Symptomatic hypoglycaemia related to mortality (unadjusted HR 1.99; 95% CI 1.20 to 3.29; p = 0.0074) but this difference disappeared following adjustment (HR 1.09; 95% CI 0.64 to 1.87; p = 0.7403). Body weight (OR 0.97; 95% CI 0.95 to 0.98; p<0.0001) and diabetes duration (OR 1.03; 95% CI 1.01 to 1.05; p = 0.0085) were independent predictors of hypoglycaemia
Conclusions: Hypoglycaemia during the initial hospitalisation was not an independent risk factor for future morbidity or mortality in patients with type 2 diabetes and myocardial infarction. Such episodes were, however, more prevalent in patients at high risk for other reasons.
Statistics from Altmetric.com
Diabetic patients with myocardial infarction have a poor prognosis and hyperglycaemia is a well-established predictor of mortality.1 The recently published European guidelines on diabetes and cardiovascular disease states that diabetic patients with myocardial infarction benefit from a tight glycaemic control, which may be accomplished with different treatment strategies.1 However, registry and trial-based retrospective subgroup analyses indicate that not only hyperglycaemia but also hypoglycaemia may impair the prognosis in patients with acute coronary syndrome.2–5 The first DIGAMI trial, randomising patients with diabetes and acute myocardial infarction to receive insulin or conventional treatment, verified that hyperglycaemia is a pronounced risk factor but, although not explored in detail, there was no indication that hypoglycaemia caused harm.6 Thus, the correlation between hypoglycaemic episodes during the initial phase of a myocardial infarction and subsequent cardiovascular events warrants a more thorough investigation for at least two reasons. A fear for induction of hypoglycaemia may counteract the use of sufficient doses of glucose-lowering agents, not least insulin, for tight glycaemic control in patients with diabetes and myocardial infarction. Moreover insights into potential mechanisms behind the relation between hypoglycaemia and subsequent cardiovascular events are of interest.
The aim of this report from the second DIGAMI trial is to further explore the impact of and reasons for hypoglycaemia during the initial phase of a myocardial infarction in patients with diabetes.
RESEARCH DESIGN AND METHODS
Patients
DIGAMI 2, a prospective, randomised trial compared three different management strategies in patients with established type 2 diabetes or an admission blood glucose >11.0 mmol/l, admitted to participating coronary care units (CCU) because of a suspected acute myocardial infarction.7 A total of 1253 patients were randomised during the period January 1998–May 2003 to one of three study arms receiving: (a) a 24-hour insulin-glucose infusion followed by subcutaneous insulin-based long-term glucose control (n = 474); (b) the same initial treatment followed by standard glucose control (n = 473); or (c) glucose-lowering treatment according to local practice (n = 306). The objective was to compare total mortality and morbidity between these management strategies. During the median follow-up time of 2.1 years (interquartile range 1.03–3.00 years) that ended 31 December 2003, there was no significant difference in total mortality or cardiovascular events between the three groups.
The protocol stated that the use of concomitant treatment should be as uniform and extensive as possible according to evidence-based international guidelines for acute myocardial infarction.8 9 Thus, all patients without contraindications were prescribed aspirin, thrombolytic agents, β-blockers, lipid-lowering drugs, angiotensin-converting enzyme (ACE) inhibitors and revascularisation procedures when appropriate. At hospital discharge 84% of the patients fulfilled the diagnosis of myocardial infarction (ST-elevation infarction = 45%). Almost all remaining patients had coronary artery disease, mostly unstable angina pectoris. Newly detected type 2 diabetes, defined as of duration less than one year, was seen in 23% of the patients. A more extensive description of the study design and the patient population has been presented elsewhere.7
Glucose-lowering treatment
Groups 1 and 2 were treated with a glucose-insulin infusion immediately after arrival at the coronary care unit (CCU) (500 ml 5% glucose and 80 IU of soluble insulin; initial infusion rate 30 ml/h to be adjusted in relation to subsequent glucose levels). The infusion was continued until stable normoglycaemia and at least for 24 hours. The aim was to reach blood glucose levels between 7–10 mmol/l as fast as possible. Samples for determination of blood glucose were drawn from an intravenous cannula at time intervals outlined in the protocol (at least every second hour during the complete infusion period and within one hour following dose adjustments). Besides these stipulated samples glucose was always checked in the presence of symptoms indicating hypoglycaemia. These bedside analyses were performed by the CCU nurse with a calibrated reflectance meter. A more detailed description of the infusion protocol has been given elsewhere.6 In group 1 the infusion was followed by multidose, subcutaneous insulin, short-acting and intermediate long-acting, targeting a fasting blood glucose between 5–7 mmol/l and non-fasting <10 mmol/l. Besides initial insulin-glucose infusions (as outlined for group 1) patients in group 2 had no protocol defined glucose-lowering treatment recommendations or glucose target. Patients in group 3, serving as controls, were treated at the discretion of the responsible physician from the beginning.
Laboratory investigations
A random blood glucose measurement was obtained as soon as possible after hospital admission. During the first 24–48 hours the blood glucose level was followed frequently in groups 1 and 2 as outlined above. Patients in group 3 had their glucose levels monitored at the discretion of their attending physician. Fasting glucose was recorded daily until hospital discharge and subsequently at each follow-up visit. Glucose samples were analysed at the local hospital laboratories in whole blood and expressed as mmol/l. Likewise blood lipids, serum creatinine and electrolytes were analysed at the local laboratories.
Follow-up
Outpatient visits were scheduled after 3, 6, 9 and 12 months and thereafter every sixth month. All patients were followed for a minimum of 6 months and a maximum of 36 months. At each follow-up a case record form was completed comprising information on fasting glucose, glycated haemoglobin (HbA1c), a detailed report on ongoing glucose-lowering and other therapies and adverse events. Events including mortality, non-fatal infarctions, stroke and coronary interventions were reported by means of special event forms.
Endpoints
In the present report the primary objective was to study the impact of hypoglycaemic episodes during the hospital phase of the DIGAMI 2 trial on total mortality and the rate of non-fatal re-infarctions and stroke during follow-up.
Definitions
Myocardial infarction was diagnosed according to the joint European Society of Cardiology/American College of Cardiology recommendations.10 A re-infarction was defined as an event >72 hours from the index infarction.
Stroke was defined as unequivocal signs of focal or global neurological deficit of sudden onset and vascular origin, lasting >24 hours.
Deaths were verified with death certificates and autopsy reports when available. Sudden cardiovascular deaths were those that occurred within 24 hours following onset of symptoms and without any other obvious reason for the fatal outcome. Deaths were labelled as cardiovascular or non-cardiovascular.
An independent committee composed of three experienced cardiologists, blinded for study group allocation, adjudicated all these events.
Hypoglycaemic episodes defined as blood glucose levels below 3.0 mmol/l were recorded during the hospital phase. Moreover, each of these episodes was labelled as with or without symptoms.
Ethical approval
Local ethics review boards approved the protocol. Written informed consent was obtained from all patients before enrolment.
Statistical methods
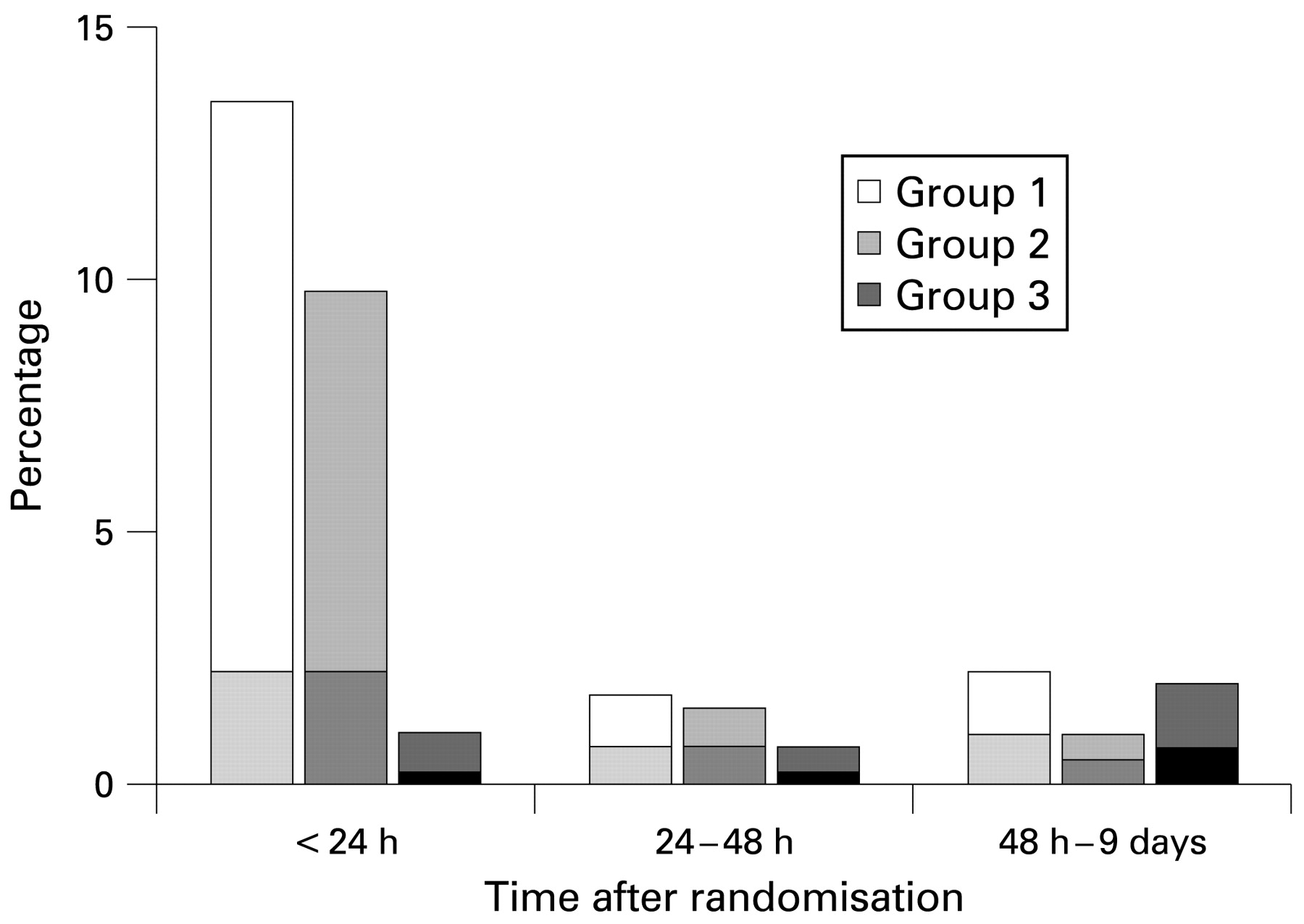
Hypoglycaemic episodes included in the present report were all recorded during the period in hospital, from time of randomisation until day 9, which was the last day of documented hypoglycaemia during hospitalisation. A time-dependent, adjusted Cox proportional hazard model was the basis for the analysis with “updated hypoglycaemia” as the main variable.11 The term “updated hypoglycaemia” relates to when the hypoglycaemic event occurred, during 0–24 hours, 24–48 hours or 48 hours–9 days respectively (see fig 1). Endpoints were considered during the complete period of follow-up—that is, both during hospitalisation and after hospital discharge.

Hypoglycaemia (blood glucose <3.0 mmol/l) by treatment group during the initial hospitalisation. The shaded area in each bar represents the proportion with symptoms.
In all adjusted multivariable models the following covariates, recorded at the time of hospital admission, were included: age, gender, smoking habits, previous myocardial infarction, congestive heart failure, pharmacological treatment, serum creatinine, diabetes duration, blood glucose and coronary interventions before admission and during hospitalisation. The same set of variables was used for all endpoints. No interaction terms was used owing to limited power. Since the time-dependent Cox model did not permit the construction of conventional Kaplan-Meier curves we chose to present such curves starting 48 hours after hospital admission. In these curves hypoglycaemic episodes, recorded during the first 48 hours, were related to events during the remaining period of follow-up. Adjustments were made for variables at hospital admission using hypoglycaemia/no hypoglycaemia as two strata.
Stepwise logistic regression was used to predict hypoglycaemic episodes during the initial 48 hours of hospitalisation. This analysis was based on the following potential risk factors as recorded at the time for hospital admission: age, weight, diabetes duration, congestive heart failure and treatment with lipid-lowering drugs and diuretics.
Two-tailed statistical tests were used at a 5% significance level. SAS version 8:02 was used for all statistical analyses.
RESULTS
Baseline characteristics
None of the 1253 patients, of whom 947 were randomised to insulin infusion during at least 24 hours and 306 were treated routinely, was lost to follow-up. Hypoglycaemic episodes during hospitalisation are reported in figure 1. Hypoglycaemia was experienced by 153 (12%) patients out of whom 45 (29%) were symptomatic. Most episodes in insulin-treated patients occurred during the first 24 hours (n = 111; 12%; symptomatic n = 26; 23%). The corresponding numbers in patients on routine treatment were three (1.0%) and one, respectively. As outlined in figure 1 there were relatively few hypoglycaemic episodes during the remainder of the hospital phase without any significant differences between the three treatment groups. The mean (SD) duration of hospitalisation was 9.5 (16.7) days for patients without and 10.2 (9.5) for those with hypoglycaemic episodes.
Patient characteristics at admission for patients with and without hypoglycaemia are presented in table 1. Patients experiencing hypoglycaemia were older, had a lower body weight and body mass index and more often presented with a history of heart failure. Moreover, they were less often treated with lipid-lowering drugs but more often with diuretics. HbA1c, admission blood glucose and glucose lowering treatment at admission did not differ. The duration of diabetes was longer among patients with than in those without hypoglycaemic episodes. Following the stepwise logistic regression analysis body weight (+1 kg; OR 0.97; 95% CI 0.95 to 0.98; p<0.0001) and diabetes duration (+1 year; OR 1.03; 95% CI 1.01 to 1.05; p = 0.0085) remained as independent predictors for subsequent hypoglycaemic events.
Mortality and morbidity
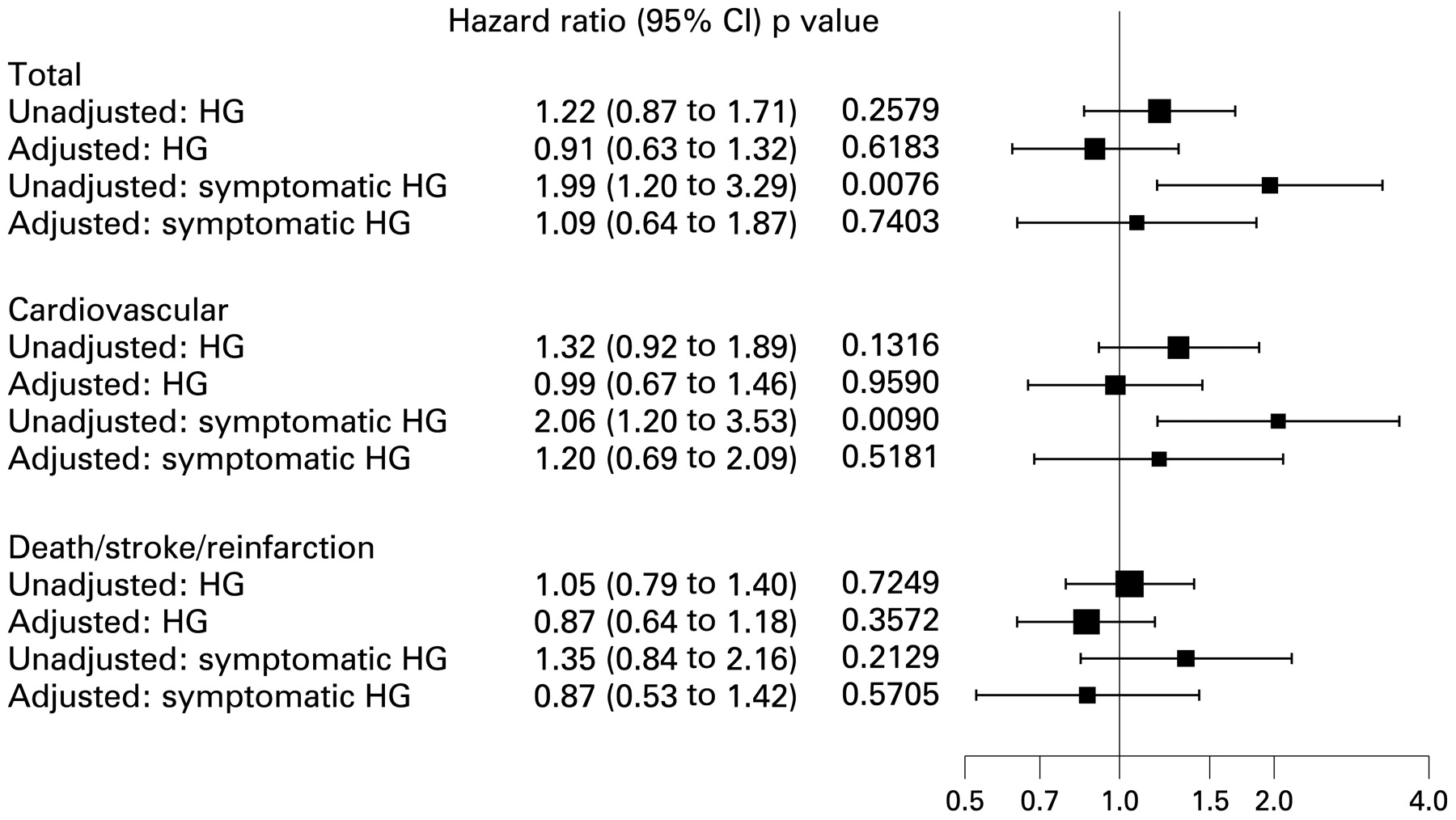
Two hundred and seventy seven (22.1%) of the 1253 patients died during the period of follow-up, the majority for cardiovascular reasons, and 217 (17.3%) patients suffered from a non-fatal re-infarction or stroke (table 2). Besides a somewhat higher total and cardiovascular mortality among patients with symptomatic hypoglycaemia the event rate showed a similar pattern in those with and without hypoglycaemic episodes. This mortality difference disappeared following adjustment for confounders. Kaplan-Meier curves for mortality and the combination of mortality and non-fatal events in patients with and without hypoglycaemic episodes are presented in figure 2A–D, while adjusted and unadjusted hazard ratios and 95% confidence levels are outlined in figure 3. Further regression analyses among patients receiving glucose-insulin infusions, testing an even lower cut-off level (2.7 mmol/l) for hypoglycaemia did not change these results.

Kaplan-Meier curves for mortality (A and C) and the combination of mortality, non-fatal myocardial infarction or stroke (B and D) in patients with (solid line) and without (broken line) hypoglycaemic episodes. Panels A and B: all patients; panels C and D: symptomatic patients only.
{kind=link}
{kind=link}
{kind=link}
Effect of hypoglycaemic events (HG), with and without symptoms, during the initial hospitalisation on subsequent mortality and morbidity.
DISCUSSION
Hypoglycaemia during the initial hospitalisation did not relate to subsequent mortality or cardiovascular morbidity in patients with type 2 diabetes and acute myocardial infarction. It was more frequent in patients who, for other reasons, had a more serious prognosis and in whom glucose-lowering treatment should be used with great caution.
The prevalence of hypoglycaemia in trials addressing the possibility to improve the prognosis in diabetic patients with myocardial infarction by glucose-lowering treatment based on insulin infusions is not negligible. The present 12% during the complete hospitalisation may be compared with 15% during the first 24 hours (all in the infusion group) in DIGAMI 16 and 6% in HI-5 (10% in the insulin and 1% in the control group).12 Concerns have been raised that adrenergic response and haemodynamic changes during periods with too low blood glucose may be harmful for an already vulnerable myocardium, thereby deteriorating the ischaemic damage or provoking arrhythmias, which may be deleterious especially in patients with acute myocardial infarction.13 14 The evidence behind these assumptions is primarily based on mechanistic studies and case reports leaving the clinical implications to be further explored.13–17 Three recent studies addressed this important question reporting on a U-shaped relation between admission glucose3 4 or retrospectively collected glucose recordings during the hospital period2 5 and mortality—that is, that hypoglycaemia and hyperglycaemia during the initial period of an acute myocardial infarction relate to a more serious prognosis. As underlined in an accompanying editorial the link between hypoglycaemia and adverse outcome still remained unclear since hypoglycaemia may merely reflect the severity of the underlying disease, and that it is this condition rather than the glycaemic state in itself that causes the unfavourable outcome.18 This could, however, not be clarified by these retrospective registry group or subgroup-based reports.
Hyperglycaemia was a strong and independent predictor of an unfavourable prognosis in the two DIGAMI trials.6 7 DIGAMI 2 does not, however, support the existence of an independent relation between hypoglycaemia and mortality and adds further information by also including data on a lack of a relation between hypoglycaemic episodes during hospitalisation and subsequent non-fatal re-infarction and stroke. In this respect this is the first report of its kind, to the best of our knowledge. The present definition of hypoglycaemia, ⩽3 mmol/l, is the same as that applied by Svensson et al2 and lower than the 81 mg/dl (≅4.5 mmol/l) used by Pinto et al3 4 and the 70 mg/dl (≅3.8 mmol/l) in the study by Kosiborod et al.5 Thus the discrepancy between the previous and present results is not explained by a too high cut off level in DIGAMI 2. If hypoglycaemic episodes are prognostically important the present criteria would strengthen rather than weaken such a relation. This assumption gets further support by the separate analysis of symptomatic hypoglycaemia and the application of a lower cut-off level, 2.7 mmol/l, in DIGAMI 2 performed in the belief that such episodes may represent more profound and/or long-lasting episodes than those disclosed by the protocol-prescribed glucose monitoring and, thereby, are potentially more prognostically important. These analyses did, however, not change the present finding.
The strengths of the present observation are that it originates from a large cohort of prospectively recruited, regularly followed group of diabetic patients with a sizeable number of adjudicated events. The prospective study design permitted a thorough adjustment for potential confounders. Moreover, DIGAMI 2 was designed to study the impact of glucose control and different glucose-lowering treatments. This ascertained a protocol driven, rigorous monitoring of blood glucose during the hospital period in the two infusion groups at highest risk for hypoglycaemia and should have encouraged glucose monitoring in the third group even if this was left to the discretion of the attending physician. Previous reports of the negative prognostic impact of hypoglycaemia were based on retrospective analyses rather than systematic monitoring. The implication is that asymptomatic hypoglycaemic episodes may have passed undetected in the two studies that related in-hospital hypoglycaemia to morbidity and mortality.2 5 This makes it reasonable to assume that those identified were severe enough to trigger the analysis of blood glucose. In addition the absence of a predefined glucose-monitoring protocol may have caused delays in detecting and treating hypoglycaemia while the DIGAMI 2 protocol ascertained early management.
The present findings are congruent with a report by Van den Berghe et al pooling data from two prospective trials in patients in intensive care.19 A blood glucose target of 110 mg/dl (6.1 mmol/l) was most effective despite a higher risk for the induction of hypoglycaemia, which in itself did not relate to mortality or neurological deficits. Likewise in a nested case-control intensive care study Vriesendorp et al could not find an association between incidental hypoglycaemia and mortality.20 The fear of hypoglycaemia has been mentioned as an obstacle in attempts to achieve normoglycaemia in a long-term as well as in a short-term perspective.7 12 21 For example healthcare professionals were reported to be reluctant to lower glucose because of fear that the insulin induced hypoglycaemia may outweigh treatment benefits in the Hyperglycaemia: Intensive Insulin Infusion in Infarction (HI-5) study.12 The present observation indicates that hypoglycaemic episodes are less harmful than previously believed, at least in carefully monitored patients.
A question left open by previous studies is whether there is a causal relation between hypoglycaemia and subsequent mortality, or if as speculated upon hypoglycaemia rather is an expression for other risk factors that are linked to a less favourable prognosis.2–5 In the present study the prognostic impact of hypoglycaemia disappeared following adjustments. Accordingly the risk for hypoglycaemia was linked to patients who, for other reasons, had a more severe prognosis. This assumption gains support from observations of hypoglycaemia as a risk marker for or a manifestation of underlying diseases—for example, renal insufficiency, hepatic disease, sepsis or malnutrition.22 23 The subgroup of DIGAMI 2 patients that was more prone to hypoglycaemia were older, with a lower body weight and more frequent co-morbidities, not least previous heart failure, and a longer duration of diabetes. These conditions may be related to an intrinsic defect counter-regulation in response to decreasing blood glucose.24
Study limitations
The present findings do not represent the outcome of a prospective randomised trial. Such a trial, exposing patients to intentionally induced hypoglycaemia can for obvious reasons not be conducted. The data derived from DIGAMI 2 are, however, based on a predefined protocol including a possibility to correct for a variety of confounders, which should improve the validity of the conclusions. DIGAMI 2 studied mortality and cardiovascular morbidity, including stroke. Minor neurological symptoms, potentially triggered by hypoglycaemia, were not recorded. It has been claimed that spontaneous, rather than treatment-induced, hypoglycaemia is of prognostic importance.23 Thus it would have been an advantage to separate such episodes from each other, but as revealed by the few episodes of hypoglycaemia in the control group such episodes seem to be uncommon, in particular considering that several patients (41%) in this study arm received occasional insulin injections that may have contributed. Finally, it should be acknowledged that the present results do not reflect the potential impact of hypoglycaemic episodes during long-term glucose-lowering treatment following hospital discharge. Thus it can still not be excluded that hypoglycaemia, at least to some extent, may account for the recently reported negative impact of insulin on cardiovascular morbidity in patients with coronary artery disease.25 26
In summary hypoglycaemic episodes during hospitalisation did not increase the risk for subsequent cardiovascular mortality and morbidity in patients with type 2 diabetes and myocardial infarction. Such episodes characterise patients, who for other reasons are at high risk, in particular those with long diabetes duration and a low body weight. These findings underline the safety of using insulin in hyperglycaemic patients with type 2 diabetes during the acute phase of a myocardial infarction provided a careful blood glucose monitoring to ascertain early detection and treatment of hypoglycaemic episodes.
Acknowledgments
The authors are grateful to Aldina Pivodic, Statistical Consulting Group, Gothenburg, for excellent support with data handling.
REFERENCES
Footnotes
Funding: Supported by the Swedish Heart-Lung Foundation, AFA Insurance and by unconditional research grants from Aventis Sweden and Novo Nordisk Denmark.
Competing interests: KM is professor of cardiology at Karolinska Institutet, Stockholm for 25% of his time and employed by AstraZeneca for 75%. This company has not been involved in the trial and has no interest in this paper.