Article Text

Abstract
Background The extent of clopidogrel-mediated platelet inhibition varies considerably from one person to the next. Numerous studies have shown that low responders have significantly more adverse events after coronary stenting than patients who respond well to antithrombotic treatment with clopidogrel. Dihydropyridine calcium-channel blockers (CCBs) inhibit the cytochrome P450 3A4 enzyme, which metabolises clopidogrel to its active form.
Objective To investigate the influence of CCBs on clopidogrel-mediated platelet inhibition.
Methods Adenosine-5-diphosphate (ADP)-inducible platelet reactivity was assessed by light transmission aggregometry (LTA) and the VerifyNow P2Y12 assay in 162 patients after percutaneous intervention with stent implantation. Results in the fourth quartiles of both assays were considered as high on-treatment residual ADP-inducible platelet reactivity.
Results Patients with concomitant CCB therapy showed a significantly higher on-treatment platelet reactivity than patients without CCB medication (p=0.001 for both assays). Further, high on-treatment residual ADP-inducible platelet reactivity was significantly more common among patients currently taking CCBs (p=0.001 for LTA and p=0.004 for the VerifyNow P2Y12 assay). A multivariate regression analysis confirmed CCB therapy as an independent predictor of reduced clopidogrel-mediated platelet inhibition (p=0.006 for LTA and p=0.004 for the VerifyNow P2Y12 assay).
Conclusion CCBs decrease clopidogrel-mediated platelet inhibition in patients undergoing angioplasty and stenting for cardiovascular disease.
- Clopidogrel
- calcium-channel blockers
- platelet function testing
- coronary stenting
- non-coronary intervention
- antiplatelet treatment
Statistics from Altmetric.com
- Clopidogrel
- calcium-channel blockers
- platelet function testing
- coronary stenting
- non-coronary intervention
- antiplatelet treatment
Introduction
The thienopyridine clopidogrel is an important component of the antiplatelet regimen after percutaneous intervention with stent implantation. After conversion to its active metabolite in the liver, it inhibits adenosine-5-diphosphate (ADP)-induced platelet aggregation by irreversibly blocking the platelet P2Y12 receptor.1–3 However, the response to clopidogrel shows a wide interindividual variability, and recent studies suggest that patients with high on-treatment residual ADP-inducible platelet reactivity are at an increased risk for adverse events after coronary stenting.4–11
Dihydropyridine calcium-channel blockers (CCBs) inhibit the cytochrome P450 3A4 enzyme, which metabolises clopidogrel to its active form.12 Thereby, CCBs may lead to an attenuation of clopidogrel-mediated platelet inhibition. Indeed, Siller-Matula et al revealed a reduction of the antiplatelet effect of clopidogrel in patients with concomitant CCB therapy.13 In their study, platelet function was assessed by the vasodilator-stimulated phosphoprotein (VASP) phosphorylation assay and multiple electrode aggregometry (MEA). As these tests are relatively new, clinical outcome data are widely missing for both assays. In contrast, light transmission aggregometry (LTA) is well established and numerous studies have associated its results with adverse events after coronary stenting.8–11 Therefore, LTA is still considered the “gold standard” method for the assessment of platelet function during antiplatelet therapy with clopidogrel. The VerifyNow P2Y12 assay is a fast point-of-care test, which has been shown to correlate strongly with LTA.14 As it is standardised and easy to perform, its results might have better reproducibility and less operator-dependency than LTA. For these reasons, we chose LTA and the VerifyNow P2Y12 assay to investigate the influence of CCBs on clopidogrel-mediated platelet inhibition in patients undergoing angioplasty and stenting for cardiovascular disease.
Patients and methods
Patients
The study was a prospective observational study to investigate the influence of CCBs on clopidogrel-mediated platelet inhibition. The study population consisted of 162 consecutive patients receiving dual antiplatelet therapy after percutaneous intervention with endovascular stent implantation. All patients received daily acetylsalicylic acid treatment (100 mg/day) before percutaneous intervention. Except for 15 patients, who were already on continuous clopidogrel treatment, all patients received a loading dose of 300 or 600 mg clopidogrel before intervention followed by a daily dose of 75 mg clopidogrel. Fifty-three patients (32.7%) received concomitant CCB therapy, whereby 52 of these patients (98.1%) were treated with dihydropyridine CCBs (84.6% amlodipine, 5.8% nifedipine, 3.85% nisoldipine, 3.85% lercanidipine and 1.9% nitrendipine) and only one patient (1.9%) received a phenylalkylamine CCB (verapamil). Exclusion criteria were a known aspirin or clopidogrel intolerance (allergic reactions, gastrointestinal bleeding), therapy with vitamin K antagonists (warfarin, phenprocoumon, acenocoumarol), therapy with ticlopidine, dipyridamole or non-steroidal anti-inflammatory drugs, a family or personal history of bleeding disorders, malignant paraproteinaemias, myeloproliferative disorders or heparin-induced thrombocytopenia, severe hepatic failure, known qualitative defects in thrombocyte function, a major surgical procedure within 1 week before enrolment, a platelet count <100 000 or >450 000/μl and a haematocrit <30%.
The study protocol was approved by the ethics committee of the Medical University of Vienna in accordance with the Declaration of Helsinki and written informed consent was obtained from all study participants.
Blood sampling
Blood was drawn by clean venepuncture from an antecubital vein using a 21-gauge butterfly needle (0.8×19 mm; Greiner Bio-One, Kremsmünster, Austria) 24 h after the percutaneous intervention.15 To avoid procedural deviations, all blood samples were taken by the same doctor applying a light tourniquet, which was immediately released and the samples were mixed adequately by gently inverting the tubes. After the initial 3 ml of blood had been discarded to reduce procedurally induced platelet activation, blood was drawn into a 3.8% sodium citrate Vacuette tube (Greiner Bio-One; nine parts of whole blood, one part of sodium citrate 0.129 mol/l) for evaluations by LTA. Further, blood was drawn into a 3.2% sodium citrate Vacuette tube (Greiner Bio-One; nine parts of whole blood, one part of sodium citrate 0.109 mol/l) for the VerifyNow P2Y12 assay. The time interval between blood sampling and testing was at least 1 h and did not exceed 3 h. To avoid investigator-related variations of the results, each of the different tests was performed by just one corresponding operator, who was blinded to the results from the other operators. Results from LTA were available for all patients; results from the VerifyNow P2Y12 assay were available for 161 patients.
LTA
LTA was performed as previously described.14 In brief, citrate-anticoagulated whole blood was centrifuged at 150×g for 10 min at room temperature to obtain platelet-rich plasma. Platelet-poor plasma was obtained from the remaining specimen by re-centrifugation at 2000×g for 10 min. Platelet counts were not adjusted as mean platelet count was 216±57 G/l. The baseline optical density was set with platelet-poor plasma. Aggregation was performed using adenosine-5-diphosphate (ADP 10 μM; Rolf Greiner BioChemica, Flacht, Germany). Optical density changes were recorded photoelectrically for 10 min as platelets began to aggregate. The maximal aggregation response was registered and used to differentiate between patients without and with residual ADP-inducible platelet reactivity.
VerifyNow P2Y12 assay
The VerifyNow P2Y12 assay (Accumetrics, San Diego, California, USA) was performed as previously described.14 Briefly, citrate-anticoagulated whole blood was automatically dispensed from the blood collection tube into the assay device by the instrument. ADP was incorporated into the assay channel to induce platelet activation, and light transmittance increased as activated platelets bound and aggregated fibrinogen-coated beads. The instrument measured this change by an optical signal and reported results in P2Y12 reaction units (PRU). With this assay, a higher PRU reflects greater ADP-mediated platelet reactivity.
Statistical analysis
Statistical analysis was performed using the Statistical Package for Social Sciences (SPSS version 15.0). Mean and SD of continuous variables are shown. The Kolmogorov–Smirnov test was used to test for normal distribution. Since all platelet function data were normally distributed, we performed t tests to test for differences of ADP-inducible platelet reactivity between patients without and with concomitant CCB therapy. Patients in the fourth quartile of LTA and the VerifyNow P2Y12 assay were considered as patients with high on-treatment residual ADP-inducible platelet reactivity, respectively. The corresponding cut-off values were a maximal aggregation ≥63% for LTA and PRU ≥272 for the VerifyNow P2Y12 assay. The χ2 test was used to detect differences in categorical variables. By univariate and multivariate regression analysis, we evaluated the impact of CCBs, cardiovascular risk factors and factors known to influence clopidogrel-mediated platelet inhibition on ADP-inducible platelet reactivity. Two-sided p values <0.05 were considered statistically significant.
Results
Clinical, laboratory and procedural characteristics of patients without and with CCB therapy are shown in table 1.
Clinical, laboratory and procedural characteristics of the investigated patients
Patients with CCB therapy were older (69±10 vs 64±12, p=0.04) and suffered more frequently from hypertension (100% vs 90.8%, p=0.02) and diabetes mellitus (50.9% vs 25.7%, p=0.001) than patients without CCB medication. Further, peripheral angioplasty (75.5% vs 48.6%, p=0.001) was performed more often in patients receiving CCBs, whereas previous myocardial infarction (46.8% vs 17%, p<0.001) and coronary stenting (41.3 vs 15.1%, p=0.001) were more common in patients without concomitant CCB therapy. The ADP-inducible platelet reactivity showed no significant differences between subjects with peripheral or carotid artery disease and patients with coronary artery disease (p>0.3). Further, no significant differences of the platelet response to ADP were observed between patients without clopidogrel loading dose, patients with a loading dose of 300 mg clopidogrel and patients with a loading dose of 600 mg clopidogrel (p>0.2).
ADP-inducible platelet reactivity by LTA and the VerifyNow P2Y12 assay in patients without and with CCB therapy is shown in table 2.
ADP-inducible platelet reactivity in patients without and with CCB treatment
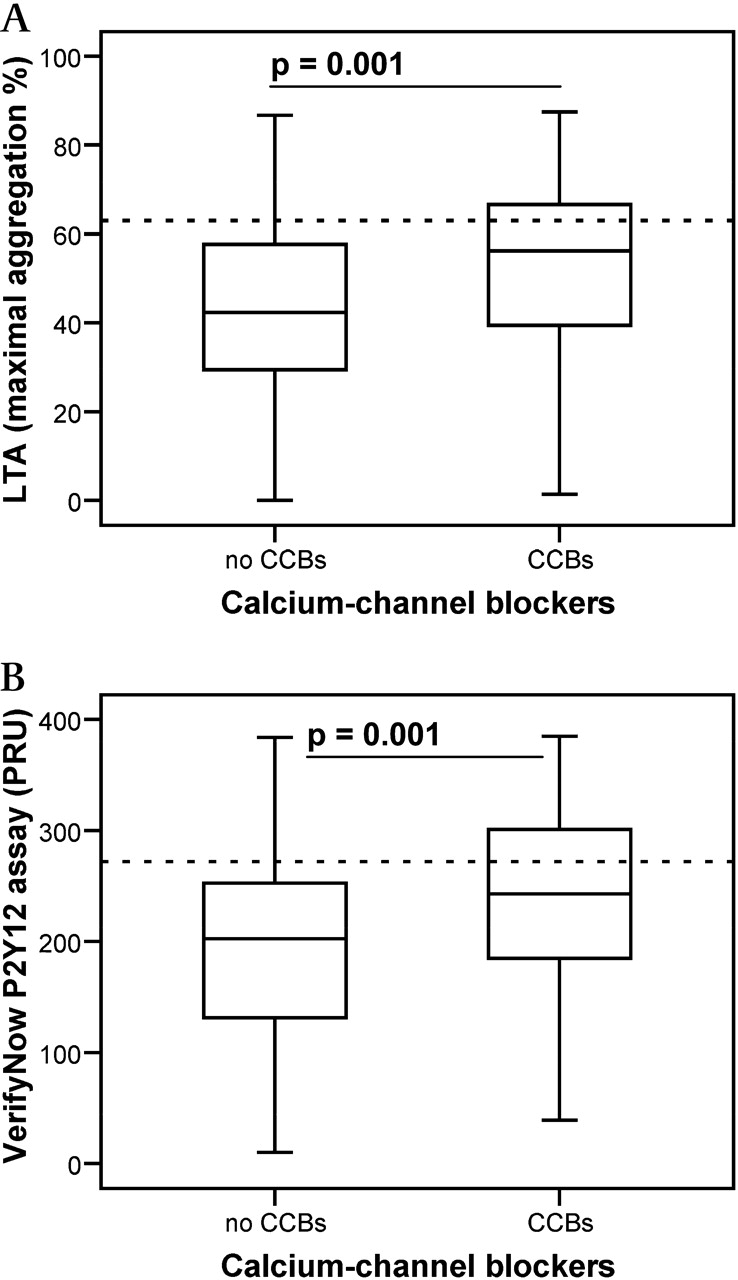
In both assays, patients with concomitant CCB therapy displayed a significantly higher ADP-inducible platelet reactivity than patients without CCB therapy (figure 1; p=0.001 for LTA and for the VerifyNow P2Y12 assay).
{kind=link}
Box-and-whisker plot showing (A) maximal aggregation % by LTA and (B) PRU by the VerifyNow P2Y12 assay in patients without and with CCB treatment. Cut-off values for high residual ADP-inducible platelet reactivity during treatment are indicated by the dotted lines. CCB, calcium-channel blocker; LTA, light transmission aggregometry; PRU, P2Y12 reaction units.
Using the above-mentioned cut-off values, high on-treatment residual ADP-inducible platelet reactivity was found in 40 patients (24.7%) by LTA and in 41 patients (25.5%) by the VerifyNow P2Y12 assay. High on-treatment residual ADP-inducible platelet reactivity was significantly more common among patients receiving CCBs than among patients without CCB therapy (41.5% vs 16.5% by LTA, p=0.001; 39.6% vs 18.5% by the VerifyNow P2Y12 assay, p=0.004). By univariate and multivariate regression analysis, we evaluated the impact of CCBs, statins, proton pump inhibitors (PPIs), age ≥65, diabetes, two different clopidogrel loading dosages, hypertension, hyperlipidaemia, creatinine, C-reactive protein, smoking status and the type of intervention (peripheral, coronary or carotid artery stenting) on ADP-inducible platelet reactivity. Thereby, CCB therapy was found to be an independent predictor of reduced clopidogrel-mediated platelet inhibition in both assays (table 3; p=0.006 for LTA and p=0.004 for the VerifyNow P2Y12 assay).
p Values of UA and MA analyses of potential influencing variables for on-treatment platelet reactivity assessed by LTA and the VerifyNow P2Y12 assay
Discussion
The major finding of our study is that concomitant CCB therapy is associated with decreased platelet inhibition by clopidogrel. To the best of our knowledge, our study is the first showing this association for platelet function data assessed by LTA and the VerifyNow P2Y12 assay.
We assessed clopidogrel-mediated platelet inhibition 24 h after the intervention. Thereby, all tests were performed at least 24 h after the administration of the clopidogrel loading dose. Although this point of time may not be the final steady state, the major antiplatelet effect of clopidogrel should have occurred.16–18
LTA still remains the gold standard method for the assessment of platelet function during antithrombotic therapy with clopidogrel. Numerous studies have verified the clinical relevance of LTA in the field of interventional cardiology.8–11 Recently, Geisler et al revealed a strong correlation between the results from LTA and the occurrence of major adverse cardiovascular events after percutaneous coronary intervention.8 The major disadvantages of LTA are the lack of standardisation and the extensive operator dependency of its results. Further, the method is labour intensive and by separating platelets from other blood components, their interaction is lost. Therefore, in addition to LTA, we chose a fast and standardised whole blood point-of-care test, the VerifyNow P2Y12 assay, as a second platelet function test to assess ADP-inducible platelet reactivity. In previous studies, we and others have already shown a strong correlation between the results from LTA and the VerifyNow P2Y12 assay.14 19 Moreover, Price et al associated the results from the VerifyNow P2Y12 assay with adverse outcomes after coronary stenting, showing a clinical validity of the assay similar to LTA.20
Recently, Siller-Matula et al revealed a reduction of the antiplatelet effect of clopidogrel in patients with coadministration of CCBs.13 In their study, platelet reactivity was assessed by the VASP assay and MEA. The VASP assay, run by flow cytometry, is the most specific method to assess ADP receptor blockage, while MEA, a whole blood assay, is based on the principle of impedance aggregometry.21–23 Beyond question, both assays provide valuable information on platelet function during antithrombotic treatment with clopidogrel. However, as these assays are relatively new, clinical outcome data are widely missing for both methods. Further, they might be superior to LTA concerning feasibility of performance and standardisation, but they are still operator dependent and certainly more time consuming than the VerifyNow P2Y12 assay. In summary, each of the described methods provides important information despite several limitations.
As in a previous study, we defined the fourth quartile of both assays as high on-treatment residual ADP-inducible platelet reactivity.14 Thereby, we obtained a cut-off value of ≥63% for LTA. Geisler et al defined a maximal aggregation >70% by LTA as low response to clopidogrel.8 In a retrospective analysis of their results, they found this cut-off level to be almost identical with the lower bound of the fourth quartile of ADP-inducible platelet aggregation. Considering the use of a higher agonist concentration for LTA by Geisler et al compared with our study (20 vs 10 μmol ADP), the cut-off values from both studies seem comparable. Siller-Matula et al based the cut-off value for high on-treatment residual ADP-inducible platelet reactivity on the lower limit of the VASP assay in healthy volunteers.13 By this method, they found high on-treatment residual ADP-inducible platelet reactivity in 25% of their patients, which was the definition of high on-treatment residual ADP-inducible platelet reactivity in our study. Therefore, the results are comparable.
As CCBs inhibit cytochrome P450 3A4, a reduced conversion of clopidogrel to its active metabolite may be responsible for the attenuation of clopidogrel-mediated platelet inhibition in patients with concomitant CCB therapy.12 24 Consequently, the reduction of the antiplatelet effect of clopidogrel by CCBs occurs only in vivo. This assumption is supported by a recent experiment, which showed that in vitro incubation of blood from patients taking clopidogrel with CCBs did not significantly affect ADP-inducible platelet aggregation.13
Omeprazole was shown to significantly reduce clopidogrel-mediated platelet inhibition.25 However, all patients from our study with concomitant PPI therapy received either esomeprazole (n=20) or pantoprazole (n=76), and there was no significant difference of clopidogrel-mediated platelet inhibition between patients without and with PPI treatment. This observation is in line with a recent study showing that esomeprazole and pantoprazole did not impair the antiplatelet effect of clopidogrel.26 Thus, the inhibitory effects of PPIs on clopidogrel-mediated platelet inhibition may vary from one drug to the next.
In conclusion, CCBs decrease clopidogrel-mediated platelet inhibition. As these are in vitro data, large prospective clinical trials are warranted to clarify the impact of concomitant CCB therapy on the long-term outcome after angioplasty and stenting in patients treated with clopidogrel.
Limitations
There were baseline differences between patients without and with CCB therapy which represent potential confounding factors, although a multivariate regression analysis including these variables revealed CCBs to be an independent predictor of reduced clopidogrel-mediated platelet inhibition in both assays. Additional study limitations are its design as an observational study instead of an interventional study of CCBs, and the lack of clinical outcome data.
Acknowledgments
The authors would like to thank Beate Eichelberger and Daniela Koren for their excellent technical assistance.
References
Footnotes
See Editorial, page 179
Competing interests None.
Ethics approval This study was conducted with the approval of the ethics committee of the Medical University of Vienna.
Provenance and peer review Not commissioned; externally peer reviewed.