Article Text

Abstract
Objectives To compare magnetic resonance myocardial perfusion imaging (MRI) with anatomical assessment by multislice computed tomography (MSCT) coronary angiography and conventional coronary angiography.
Design and patients In this prospective study, 53 patients (60% male, average age 57±9 years, 83% intermediate pre-test likelihood) underwent 1.5 T MRI, 64-slice MSCT and conventional coronary angiography.
Main outcome measures The presence of significant stenosis (≥50% luminal narrowing) was determined on MSCT and conventional coronary angiography. Ischaemia on MRI was defined as a stress perfusion abnormality in the absence of delayed contrast enhancement.
Results A significant stenosis was seen on MSCT in 15 (28%) patients, while ischaemia on MRI was seen in 19 (36%). In the 38 patients without significant stenosis on MSCT, normal perfusion was seen in 29 (76%). In patients with a significant stenosis on MSCT, ischaemia was seen in 10 (67%). In all patients without significant stenosis on MSCT and normal perfusion on MRI (n=29), significant stenosis was absent on conventional coronary angiography. All patients with both MSCT and MRI abnormal (n=10) had significant stenoses on conventional coronary angiography.
Conclusion The anatomical and functional data obtained with MSCT and MRI are complementary for the assessment of coronary artery disease. These findings support the sequential or combined assessment of anatomy and function.
- MSCT
- MRI
- atherosclerosis
- myocardial perfusion
- coronary artery disease(CAD)
- MRI
- magnetic resonance imaging
- MSCT
- multislice computed tomography
Statistics from Altmetric.com
Introduction
Coronary artery disease (CAD) remains one of the leading causes of morbidity and mortality in the Western world. In this regard, non-invasive imaging modalities have an increasingly important role. Following the recent development of non-invasive anatomical imaging using multislice computed tomography coronary angiography (MSCT), non-invasive imaging of atherosclerosis has received particular interest. With this technique, fast evaluation of coronary anatomy has become possible, enabling stenosis detection with a high diagnostic accuracy compared with conventional coronary angiography.1 2 Notably, subclinical atherosclerosis, possibly warranting more targeted anti-atherosclerotic therapy, can also be easily identified with this technique.
However, non-invasive anatomical imaging (MSCT angiography) cannot predict ischaemia, which is needed to guide decisions about potential revascularisation. Several studies comparing the relationship between MSCT and functional imaging of myocardial perfusion using single photon emission computed tomography (SPECT) and positron emission tomography (PET) have indeed shown a discrepancy between non-invasive anatomical and functional imaging, suggesting that these techniques may provide complementary information about the presence, extent and severity of CAD.3 4
In addition to the currently available nuclear imaging techniques, myocardial perfusion abnormalities reflecting ischaemia may also be appreciated using MRI.5 6 Myocardial perfusion imaging using stress MRI has a good diagnostic accuracy compared with non-invasive functional imaging using SPECT and PET, and invasive imaging using fractional flow reserve.7–9 Because of its high spatial resolution and lack of ionising radiation, MRI may possibly be used as an alternative to SPECT and PET for combined anatomical and functional imaging in combination with MSCT. Currently, the potential complementary relation between MSCT and MRI perfusion imaging has not been investigated. Therefore the purpose of this study was to compare myocardial perfusion imaging by MRI with anatomical assessment by MSCT and conventional coronary angiography.
Patients and methods
Patient population and study protocol
In this prospective cohort study, 53 consecutive patients referred for conventional diagnostic coronary angiography because of suspected CAD underwent additional evaluation with MSCT and cardiovascular MRI within a period of 14 days. Patients were excluded from the study if they met one of the following exclusion criteria for MSCT: cardiac arrhythmias, renal insufficiency (serum creatinine >120 mmol/l), known hypersensitivity to iodine contrast media and pregnancy. Further exclusion criteria for MRI were cardiac pacemakers or intracranial aneurysm clips and claustrophobia. Finally, patients were excluded if a cardiac event (worsening angina, revascularisation, or myocardial infarction) occurred in the period between the three examinations.
Baseline characteristics of the patients were recorded, and their pre-test likelihood of CAD was determined using the Diamond and Forrester method, with a risk threshold of <13.4% for low risk, >87.2% for high risk and between 13.4% and 87.2% for intermediate risk, as previously described.10 The study was approved by the local medical ethics committee (Medical Centre Haaglanden, The Hague, The Netherlands) and all patients gave written informed consent.
Quantitative coronary angiography
Conventional coronary angiography was performed according to standard techniques. Quantitative coronary angiography (QCA) analysis of the most severe lesion was performed for each coronary artery by an observer blinded to the MSCT and MRI results using an offline software program (QCA-CMS, version 6.0, Medis, Leiden, The Netherlands). Coronary arteries were divided into 17 segments according to the modified American Heart Association classification and QCA was performed in lesions exceeding 30% luminal narrowing on visual assessment.11 A significant stenosis was defined on a patient and vessel level as ≥50% luminal narrowing on QCA.
Multislice computed tomography
All examinations were performed using a 64-slice MSCT scanner (Lightspeed VR 64, General Electrics, Milwaukee, Michigan, USA). A patient's heart rate and blood pressure were monitored before each scan. In the absence of contraindications, patients with a heart rate exceeding the threshold of 65 beats/min were administered β-blocking drugs (50–100 mg metoprolol, orally or 5–10 mg metoprolol, intravenously).
Before the helical scan, a non-enhanced electrocardiographically (ECG)-gated scan, prospectively triggered at 75% of the R–R interval, was performed to measure the coronary calcium score (CS). The retrospectively ECG-gated helical scan was performed using the following scan parameters: collimation 64×0.625 mm; rotation time 0.35 s; tube voltage 120 kV and tube current 600 mA (with tube modulation to reduce the radiation dose). A bolus of 80 ml iomeprol (Iomeron 400, Bracco, Milan, Italy) was injected at 5 ml/s followed by 40 ml saline flush. Datasets were reconstructed from the retrospectively gated raw data with an effective slice thickness of 0.625 mm.
Post-processing of the MSCT calcium scans and coronary angiograms was performed on a dedicated workstation (Advantage, GE Healthcare, Waukesha, Wisconsin, USA). The total CS was calculated using the Agatston method. Coronary anatomy was evaluated using the contrast-enhanced helical examinations. Coronary arteries were divided into 17 segments according to the modified American Heart Association classification.11 All studies were interpreted by two experienced observers blinded to the results of coronary angiography and MRI with an intention-to-diagnose strategy. Discrepancies in interpretation were resolved by consensus. MSCT results were classified on a patient and vessel level as normal (no identifiable plaque or wall irregularities), non-significant, non-obstructive CAD (<50% luminal narrowing) or significant, obstructive CAD (≥50% luminal narrowing).
Magnetic resonance imaging
MRI was performed with a 1.5 T scanner (Symphony, Siemens, Erlangen, Germany), using a multichannel surface coil array. A first-pass MRI perfusion scan was performed during adenosine stress to determine the presence of hypo-enhancement indicative of a perfusion defect during stress. After first-pass perfusion imaging delayed contrast-enhanced MRI was performed to determine the presence of areas with hyper-enhancement indicating scar tissue. The integration of the two datasets provides differentiation between ischaemia and scar tissue.12 13 Studies were analysed for each patient and for each vascular territory. To assess MRI results for each vascular territory, the myocardium was divided into segments using a modified 17-segment model described elsewhere, without the apex.14 Segments 1, 2, 7, 8, 13 and 14 were allocated to the left anterior descending artery, segments 3, 4, 9, 10 and 15 to the right coronary artery and finally, segments 5, 6, 11, 12 and 16 were allocated to the left circumflex artery.
First-pass stress perfusion MRI
During the examination, pharmacological stress was applied using adenosine infusion. In order to obtain maximum vasodilatory effect, patients were instructed to abstain from smoking, tea and coffee and were asked to stop anti-anginal drugs and β blockers for 24 h before the examination.
The first pass of 0.1 mmol/kg gadolinium-DOTA (Dotarem, Guerbet, Gorinchem, the Netherlands) injected at a rate of 3 ml/s was assessed after 6 min of adenosine infusion (140 μg/kg/min) in three short-axis slices at the basal, mid- and apical level of the left ventricle. Using the following parameters: TrueFISP with a notched saturation pulse, inversion time 230 ms, repetition time/echo time 427 ms/ 1.53 ms, flip angle 8°, matrix 256 by 122, field of view 341 by 420 mm, slice thickness of 8 mm with a slice gap of 8 mm.
The images were evaluated by two experienced observers blinded to the MSCT and QCA results using dedicated software (MASS, version 5.1, Medis, Leiden, The Netherlands). Using the short-axis acquisitions, first-pass stress perfusion MRI scans were visually scored using the proposed modified 17-segment model, without the apex.14 Each segment was graded on a five-point scale (0=no hypo-enhancement, 1=hypo-enhancement 1–25% of left ventricular (LV) wall thickness, 2=hypo-enhancement 26–50% of LV wall thickness, 3=hypo-enhancement 51–75% of LV wall thickness and 4=hypo-enhancement 76–100% of LV wall thickness.15
Delayed contrast-enhanced MRI
Delayed contrast-enhanced MRI was obtained 15 min after infusion of gadolinium in three short-axis slices at the basal, mid- and apical level of the left ventricle, using inversion recovery Turbo-Flash technique (repetition time/echo time 705 ms/4.30 ms, flip angle 25°, matrix 256 by 166, field of view 341 by 420 mm and a slice thickness of 6 mm). The inversion time was adjusted to null normal myocardium.
The images were evaluated by two experienced observers blinded to the MSCT and QCA results using dedicated software (MASS, version 5.1, Medis, Leiden, The Netherlands). Hyper-enhancement on the delayed contrast-enhanced MR images was scored according to the same segment model used for the analysis of first-pass stress perfusion MRI.14 Each segment was graded on a five-point scale (0=no hyper-enhancement, 1=hyper-enhancement 1–25% of LV wall thickness, 2=hyper-enhancement 26–50% of LV wall thickness, 3=hyper-enhancement 51–75% of LV wall thickness and 4=hyper-enhancement 76–100% of LV wall thickness.15
Differentiation between ischaemia and scar
Ischaemia was defined as the presence of hypo-enhancement during first-pass stress perfusion in the absence of hyper-enhancement on the delayed contrast-enhanced MRI. In segments with scar the degree of hyper-enhancement (1% through 100% of LV wall thickness) was subtracted from the degree of hypo-enhancement during the first-pass perfusion to differentiate between partially reversible defects and total irreversibility. Segments with partial reversibility were subsequently graded as ischaemic.
Data analysis
Continuous variables were expressed as mean with standard deviation and proportions were expressed in percentages. First, MSCT observations were compared with QCA to evaluate the ability of MSCT to detect significant stenosis (≥50% luminal narrowing). Second, MSCT was compared with MRI to determine the relation between anatomical assessment with MSCT and ischaemia on MRI. Finally, flow charts were created to determine the relationship between MSCT, MRI and QCA. Comparisons were performed on a patient and vascular territory level.
Results
Patients were clinically referred for invasive coronary angiography because of chest pain suspected to be CAD. All characteristics of the study population are listed in table 1. Briefly, the average age was 57±9 years and the population consisted of 60% male patients. The majority of patients (83%) presented with an intermediate pre-test likelihood of CAD.
Patient characteristics (n=53)
Multislice computed tomography
The heart rate exceeded 65 beats/min in 35 patients (66%) and in these patients additional β-blocking drugs were administered. As a result, the average heart rate during MSCT was 59±8 beats/min. The average CS of the population was 251±487. Calcifications were present in 37 patients (70%) and a CS >400 was found in 10 patients (19%).
On a patient level, the MSCT angiogram was classified as normal in 14 (26%) patients, non-significant, non-obstructive CAD (<50% luminal narrowing) in 24 (45%) and significant, obstructive CAD (≥50% luminal narrowing) was observed in the remaining 15 (28%) patients. On a vessel level, normal coronary anatomy was present in 83 (52%) vessels, non-significant disease (<50% luminal narrowing) in 51 (32%) and significant disease (≥50% luminal narrowing) in 25 (16%) vessels.
Magnetic resonance imaging
First-pass perfusion MRI during adenosine stress disclosed normal myocardial perfusion in 34 patients (64%). A perfusion defect was observed in the remaining 19 patients (36%). During the delayed contrast-enhanced scan hyper-enhancement was seen in three patients (6%). In these patients the first-pass perfusion defects were only partially attributable to scar. Thus on a patient level ischaemia was absent in 34 (64%) patients, while a perfusion abnormality indicative of ischaemia was seen in the remaining 19 (36%) patients. On a vascular level, 126 (79%) territories showed no hypo-enhancement during first-pass perfusion MRI. Thus, hypo-enhancement was found in the remaining 33 (21%) vascular territories. During delayed contrast-enhanced MRI hyper-enhancement was found in four of the territories showing first-pass perfusion abnormalities. In one territory partial reversibility was seen while in the remaining three territories the abnormalities seen during first-pass perfusion were entirely attributable to scar tissue. Accordingly, on a vascular territory level, perfusion abnormalities indicative of ischaemia were present in 30 (19%) vascular territories.
Relation between anatomical and functional imaging
Relation between MSCT and QCA
The agreement between MSCT and QCA for the detection of significant CAD is shown in table 2. MSCT correctly identified 13/15 (87%) significant, obstructive lesions on QCA (≥50%) and accurately ruled out the presence of significant disease in 36/38 (95%) patients without significant lesions on QCA.
Agreement between MSCT and QCA
In table 2 the relationship between MSCT and QCA is illustrated on a vessel level. MSCT correctly identified 20/25 (80%) significant, obstructive stenoses and correctly ruled out a significant lesion in 129/134 (96%) vessels without significant lesions on QCA.
Relation between MSCT and MRI
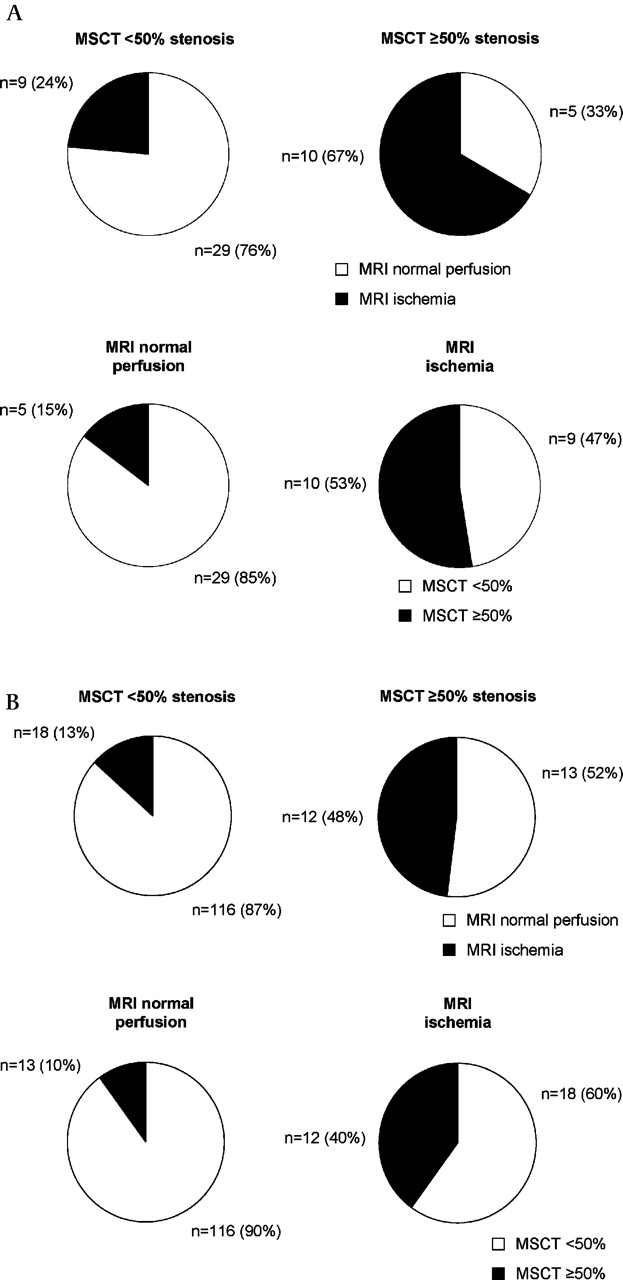
Figure 1A illustrates the complementary value of MSCT and MRI. Only 67% of patients with a significant, obstructive lesion (≥50% luminal narrowing) on MSCT showed ischaemia on MRI. Vice versa, a significant, obstructive stenosis was observed in 15% of patients with normal perfusion on MRI. A similar complementary value between MSCT and MRI was observed when assessing the relation between MSCT and MRI on a vascular territory level (figure 1B).
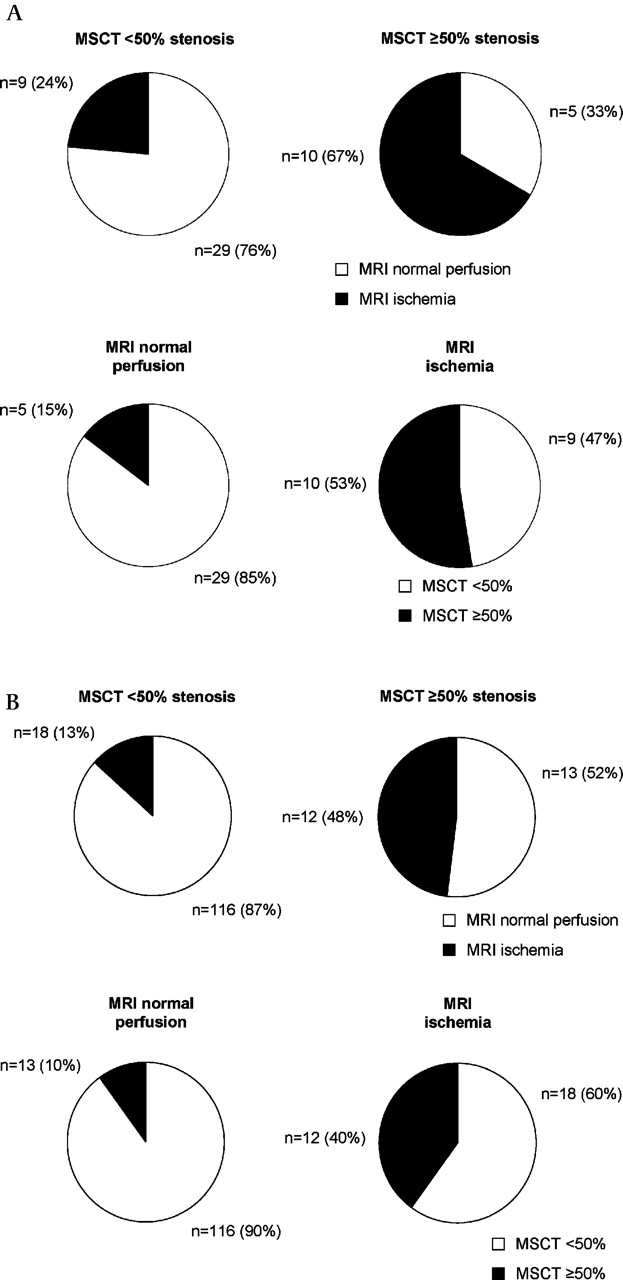
Pie charts depicting the relationship between the anatomical information obtained by multislice computed tomography (MSCT) and the functional information from MRI on a patient level (A) and on a vascular territory level (B).
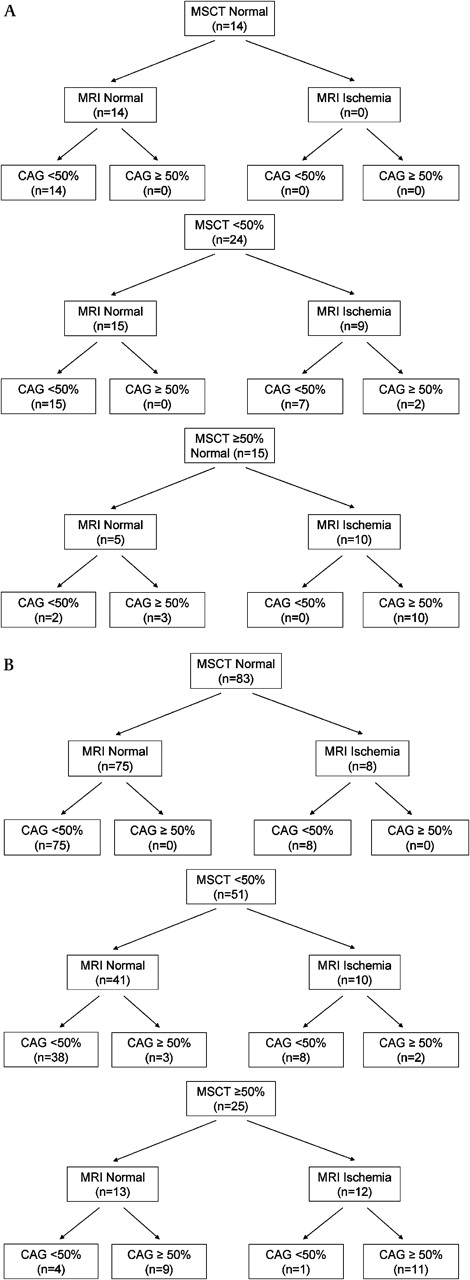
Figure 2 further illustrates the complementary value of MRI and MSCT. In this figure, the results of MRI and QCA are presented in patients with a normal MSCT, non-significant, non-obstructive CAD (MSCT <50% luminal narrowing) and in patients with significant, obstructive CAD (MSCT ≥50% luminal narrowing). Importantly, MRI was normal in all patients with a normal MSCT (n=14, 100%). Furthermore, no significant stenoses were observed on QCA in these patients. In the 24 patients with non-significant, non-obstructive CAD (<50% luminal narrowing) on MSCT, MRI was normal in 15 (63%) while ischaemia was observed in nine (37%). Thus, approximately one out of three people with non-significant, non-obstructive CAD (<50% narrowing) had ischaemia on perfusion MRI. In two patients classified as having non-significant CAD on MSCT a significant stenosis was observed on QCA. Importantly, ischaemia was observed on MRI in both of these patients. Nevertheless, in all patients without significant stenosis on MSCT and normal perfusion on MRI, absence of a significant stenosis was confirmed on QCA.

Flow charts describing the relationship between multislice computed tomography (MSCT), MRI and quantitative coronary angiography (CAG) on a patient level (A) and on a vascular territory level (B). These flow charts illustrate the complementary value of MRI in patients with non-significant and significant stenosis on MSCT.
Finally, in the 15 patients with a significant stenosis on MSCT (≥50% luminal narrowing), MRI was normal in five (33%) and ischaemia was observed in 10 (67%). In other words, one out of three patients with a significant stenosis on MSCT had normal perfusion on MRI. Two patients were classified as having a significant stenosis on MSCT while QCA was non-significant. Ischaemia on MRI was absent in both of these patients. Importantly, however, in all patients with both a significant stenosis on MSCT and ischaemia on MRI the presence of a significant stenosis was confirmed on QCA. Similar findings were observed on a vascular territory level. An example of a patient with a perfusion defect on MRI, a significant stenosis on MSCT and a significant stenosis on QCA is presented in figure 3.

{kind=link}
{kind=link}
{kind=link}
Case example of a patient with a large perfusion defect in the inferior wall on MRI during first-pass perfusion (A) and a small area showing delayed enhancement (B), suggesting the presence of predominantly ischaemia in addition to a small region of scar tissue. On MSCT a corresponding high-grade stenosis was identified in the right coronary artery (C). On coronary angiography the right coronary angiography was occluded with collaterals originating from the right ventricular branch (D).
Discussion
The main finding of this study is that MSCT coronary angiography and MRI perfusion imaging may provide complementary information about the presence, extent and severity of CAD.
Complementary value of MSCT and MRI
In patients with a significant stenosis on MSCT, normal perfusion on MRI was observed in 33%, suggesting that still a large proportion of significant stenoses on MSCT have no effect on myocardial perfusion (not associated with stress-inducible ischaemia). Simultaneously, these findings indicate that normal perfusion on MRI cannot rule out the presence of significant atherosclerosis. Indeed a significant stenosis was still observed in approximately one out of six of patients without evidence of ischaemia on MRI. Although currently no comparison has been available between MSCT and MRI perfusion imaging, several previous studies have assessed the relationship between conventional coronary angiography and MRI.13 16–18 In a meta-analysis by Nandalur et al significant stenosis on conventional coronary angiography was associated with abnormal perfusion on MRI in 58–97% of patients.18 Initially, this correlation seems higher than that seen in our study when comparing MSCT with MRI. However, differences in methodology such as the use of different cut-off points (50%, 70% and 75% luminal narrowing) for significant stenosis as well as a differences in disease prevalence (on average ≈60% in the meta-analysis by Nandalur et al compared with ≈30% in our study) may have exerted a major influence on individual observations.19
In patient populations more comparable to those of our current study in patients with an intermediate pre-test likelihood, the relationship between coronary anatomy and myocardial perfusion has been studied by comparing MSCT with SPECT or PET imaging.3 4 In the study by Schuijf et al, only 50% of patients with a significant (≥50%) lesion on MSCT had an abnormal perfusion on SPECT.4 Conversely, normal perfusion on SPECT was unable to rule out the presence of significant CAD or atherosclerosis in general. In a more recent study by Gaemperli et al the MSCT observations were corroborated by invasive coronary angiography.20 The predictive value of obstructive CAD on MSCT was 58% for the prediction of a reversible perfusion defect on SPECT. Importantly, the accuracy of MSCT to identify abnormal perfusion on SPECT was similar to that of QCA. These observations support the notion that the low predictive value of MSCT for reversible perfusion defects is not caused by inaccuracies in stenosis detection with MSCT but merely reflects inherent differences of the techniques. The results of our study comparing MSCT with MRI perfusion imaging are in line with those observed when comparing MSCT with nuclear perfusion imaging and further support the suggestion that MSCT and MRI may provide complementary information for the identification of the presence, extent and severity of CAD.
Combined anatomical and functional imaging
The combined assessment of coronary anatomy and myocardial perfusion may not only provide complementary information for different aspects of CAD, but may also result in a higher diagnostic accuracy for the detection of haemodynamically significant coronary artery lesions, as has been suggested in preliminary work by Rispler et al.21 In a study population of 56 patients, hybrid imaging using a SPECT MSCT scanner resulted in improved specificity and positive predictive value for the identification of haemodynamically significant coronary lesions. In line with these results the addition of MRI to MSCT improved identification of significant stenosis on QCA in this study; all patients with both a significant stenosis on MSCT and ischaemia on MRI were associated with a significant stenosis on QCA. Conversely, in all patients without significant stenosis on MSCT and normal perfusion on MRI, absence of a significant stenosis was confirmed by QCA.
Possibly, diagnostic accuracy may improve even further on a vessel basis by fusing both MSCT and MRI perfusion datasets into a single, three-dimensional anatomical representation of the heart with overlying coronary anatomy. This approach may enable accurate allocation of perfusion defects to the corresponding stenosis. Gaemperli et al assessed the accuracy of cardiac image fusion by combining MSCT and SPECT.22 The authors concluded that in almost one-third of patients, fusion of MSCT and SPECT resulted in increased diagnostic performance, especially in functionally relevant lesions in distal segments and diagonal branches and in vessels with extensive disease or calcifications. Fusion of MSCT and MRI perfusion datasets may potentially provide similar information in the future.
Clinical implications
The combination of anatomical imaging for identification of atherosclerosis and functional imaging for assessment of myocardial perfusion may improve risk stratification and have important implications for patient management.23 Recently, a flow chart incorporating anatomical and functional imaging has been suggested which separates patients into three groups for management: the first group with normal coronary anatomy who can be safely discharged, a second group with non-flow-limiting stenosis requiring medical treatment and aggressive risk factor modification and a final group of patients with a flow-limiting stenosis requiring further evaluation with conventional coronary angiography with potentially revascularisation.24
Such diagnostic strategies initially proposed the use of SPECT imaging for assessment of ischaemia in combination with anatomical assessment using MSCT. Indeed, SPECT imaging remains the most robust and extensively used modality for assessment of ischaemia. However, the combination of SPECT and MSCT, although having the potential to improve patient management, is associated with an increased radiation burden.25 Because of the lack of ionising radiation, MRI may be considered a promising alternative to SPECT for combined anatomical and functional assessment with MSCT, although the limited availability of MRI perfusion imaging and the associated costs currently inhibit the widespread use of this technique. Therefore the use of MRI in this setting will remain largely dependent on local availability.
Study limitations
Both MSCT and MRI have some general limitations. Even though the diagnostic accuracy of MSCT is high, images are of poor quality in still a small percentage of patients. This percentage is expected to continue to decrease with newer-generation scanners. Another limitation of MSCT is the considerable radiation dose associated with the currently used 64-slice system. Radiation burden can, however, be decreased using newer-generation scanners and protocols.26 27
A general limitation of MRI includes the relatively longer examination times which can be uncomfortable for some patients. Furthermore, a limitation of the clinical applicability of MRI perfusion imaging is the wide variation in scan protocols, scanners and data analysis methodologies that currently exist. In our study a qualitative approach was used similar to previously published studies.9 13 28 29 Other studies have used quantitative methodologies, which have the advantage of decreased interobserver variability. However, their disadvantages include a time-consuming quantification and lack of a definition of optimal and standardised approaches.
Conclusion
The anatomical and functional data obtained with MSCT and MRI provide complementary information for the assessment of CAD. These findings support the sequential or combined assessment of anatomy and function in patients presenting with suspected CAD.
References
Footnotes
Linked articles 183731.
Funding JMvW is financially supported by a research grant from the Netherlands Society of Cardiology (Utrecht, The Netherlands). JJB has research grants from Medtronic (Tolochenaz, Switzerland), Boston Scientific (Maastricht, The Netherlands), BMS medical imaging (N Billerica, Massachusetts, USA), Biotronik (Berlin, Germany), St Jude Medical (Veenendaal, The Netherlands), GE Healthcare (St Giles, UK), and Edwards Lifesciences (Saint-Prex, Switzerland).
Competing interests None.
Ethics approval This study was conducted with the approval of the Medical Centre Haaglanden.
Provenance and peer review Not commissioned; externally peer reviewed.