Article Text

Abstract
Objectives In patients with aortic stenosis (AS) left ventricular (LV) myocardial growth may exceed individual needs to compensate LV haemodynamic load leading to inappropriately high LV mass (iLVM), a condition at high risk of adverse cardiovascular events. The prognostic impact of iLVM was determined in 218 patients with asymptomatic severe AS.
Methods iLVM was recognised when the measured LV mass exceeded 10% of the expected value predicted from height, sex and stroke work (prognostic cut-off assessed by a specific ROC analysis). For assessment of outcome, the endpoint was defined as death from all causes, aortic valve replacement or hospital admission for non-fatal myocardial infarction and/or congestive heart failure.
Results At the end of follow-up (22+13 months) complete clinical data were available for 209 participants (mean age 75+11 years). A clinical event occurred in 81 of 121 patients (67%) with iLVM and in 26 of 88 patients (30%) with appropriate LV mass (aLVM) (p<0.001). Event-free survival in patients with aLVM and iLVM was 78% vs 56% at 1-year, 68% vs 29% at 3-year and 56% vs 10% at 5-year follow-up, respectively (all p<0.01). Cox analysis identified iLVM as a strong predictor of adverse outcome (Exp β 3.08; CI 1.65 to 5.73) independent of diabetes, transaortic valve peak gradient and extent of valvular calcification. Among patients with LV hypertrophy, those with iLVM had a risk of adverse events 4.5-fold higher than counterparts with aLVM.
Conclusions iLVM is common in patients with asymptomatic severe AS and is associated with an increased rate of cardiovascular events independent of other prognostic covariates.
- Aortic stenosis
- aortic valve disease
- inappropriate left ventricular mass
- left ventricular hypertrophy
- old age
- prognosis
Statistics from Altmetric.com
- Aortic stenosis
- aortic valve disease
- inappropriate left ventricular mass
- left ventricular hypertrophy
- old age
- prognosis
Left ventricular hypertrophy (LVH) is common in patients with severe aortic stenosis (AS) and represents the effort of the cardiovascular system to keep wall stress close to normal values.1 In these patients, severe LVH and concentric left ventricular geometry are associated with an increased risk of postoperative mortality after aortic valve replacement (AVR).2–4 We recently documented that a significant portion of patients with AS has an excessive growth of left ventricular mass (LVM),5 a condition named ‘inappropriately high left ventricular mass’ (iLVM),6 associated with an unfavourable cardiovascular profile and adverse outcomes in patients with arterial hypertension.7–9 Whether iLVM has a prognostic significance in patients with AS is yet unknown.
Accordingly, the present study was designed to examine the prognostic impact of iLVM in patients with asymptomatic severe AS and to assess whether the evaluation of the appropriateness of LVM offers additional predictive value in patients with LVH.
Methods
Study population
Patients older than 18 years with asymptomatic severe AS were selected for this study among individuals consecutively referred to the echocardiography laboratory of ‘Villa Bianca’ Hospital in Trento and ‘Spedali Civili Brescia’ for a cardiac murmur (70%), palpitations (20%) or check-up (10%). AS was assessed as ‘asymptomatic’ in patients in New York Heart Associationi functional class I without angina or syncope. Severe AS was diagnosed as aortic valve thickening accompanied by an aortic valve area (AVA) smaller than 1.0 cm2 or a mean transvalvular gradient greater than 40 mmHg.10 11 Exclusion criteria were a history of coronary artery disease (diagnosed by clinical, electrocardiographic and echocardiographic evaluation at rest and by the results of an exercise/echo-stress test), a clinical indication to coronary angiography, more than mild mitral valve regurgitation or stenosis,10 11 primary hypertrophic or restrictive cardiomyopathy, acute myocarditis, alcohol-induced myocardial injury, renal, hepatic or neoplastic disease. Patients were enrolled into the study between May 2003 and May 2008.
Assessment and follow-up
After completion of clinical history, physical and laboratory examination (haemoglobin, haematocrit, parameters of renal and hepatic function, serum sodium and potassium), eligible subjects underwent echocardiographic examination. Diabetes, arterial hypertension (defined as pharmacologically treated high blood pressure), hypercholesterolaemia (defined as total cholesterol >200 mg/dl or ongoing pharmacological lipid-lowering treatment), atrial fibrillation, smoking habit and obesity (diagnosed if patients had body mass index ≥30 kg/m2) were recorded.
The appearance of symptoms during the follow-up was taken into account for considering AVR.10 11 However, the decision to operate was left to the judgement of the attending physician. Once AVR was planned, coronary angiography was routinely scheduled before surgery. The follow-up information was obtained by interviewing the patients and/or their relatives. For assessment of outcome, the endpoint was defined as death from all causes or AVR or hospital admission for non-fatal myocardial infarction and/or congestive heart failure (CHF). The protocol of the present study was approved by the local institutional review boards, and informed consent was obtained from all recruited subjects.
Echocardiography
Echocardiograms were performed prospectively using Megas Esaote Biomedica (Italy) and Vivid 7 General Electrics (USA) machines equipped with 2.5–3.5 MHz annular array transducers and sonographers were blinded to clinical data. Left ventricular chamber dimensions and wall thicknesses were measured by the American Society of Echocardiography guidelines and LVM was calculated using a necropsy validated formula.12 LVM was normalised for height to the 2.7 power and LVH was defined as LVM of 49.2 g/m2.7 or greater for men and 46.7 g/m2.7 or greater for women.13 The relative wall thickness was calculated as posterior wall thickness/left venticular diastolic radius ratio independently of the presence of LVH and indicated concentric left venticular geometry if 0.43 or greater. Left venticular volumes and ejection fraction were measured by the biplane method of disks.14 Stroke volume derived by Teichholtz's formula was used for calculating the predicted LVM, as the equation for predicting LVM was originally generated using this method.15 Myocardial contractility was assessed by means of stress-corrected midwall shortening16 (considered depressed if <87% in men and <90% in women).17
AVA was measured by the continuity equation and normalised for body surface area. As indexes of aortic valve severity, we also considered in this study the energy loss index,18 the stroke work loss19 and the valvulo-arterial impedance.20 The degree of valve calcification was scored according to the following criteria: 1, no calcification; 2, mildly calcified (isolated, small spots); 3, moderately calcified (multiple bigger spots); 4, heavily calcified (extensive thickening/calcification of all cusps).21
An excess of LVM was assessed as the ratio between the observed and predicted value. LVM was predicted from stroke work, gender and body size (as height (m) to the 2.7 power) by the following equation22:
In which stroke work was estimated from brachial systolic blood pressure (measured at the end of the echo exam) plus continuous wave (CW) Doppler transaortic peak gradient times stroke volume and converted to grammeters by multiplying by 0.0144. Gender was assigned the value of 1 for men and 2 for women.
Statistical analysis
Data are reported as mean values±1 SD. Between-group comparisons of categorical and continuous variables were performed by the χ2 test and analysis of variance (ANOVA), respectively. Receiver operating characteristic (ROC) analysis was used to assess the best cut-off point of measured/predicted LVM ratio for identifying patients with a poorer prognosis. For categorisation, LVM was defined ‘inappropriately high’ when exceeding the prognostic cut-off value identified by the ROC analysis. In a secondary analysis, the cut-off value of observed/predicted LVM greater than 128% was tested. A subanalysis was also performed to investigate the outcome of patients with inadequate LVM defined as a measured/predicted LVM ratio below the 10th percentile of the distribution of the study population. Multiple logistic regression analysis was performed to assess the variables independently associated with iLVM. Log cumulative hazard functions were computed by univariate and multivariate Cox proportional hazards analyses (SPSS version 11.0) and probabilities of event-free survival and survival curves were obtained (differences between the curves were tested for significance by the log-rank test). Variables that were significantly related to iLVM in univariate tests (p<0.05) were included in the multivariate model. The in-model tolerance to evaluate multicollinearity was assessed by regression analysis. Minimal accepted tolerance was 0.80. A two-tailed value of p≤0.05 was used to reject the null hypothesis.
Results
The appropriateness of LVM could be determined in 218 of 224 patients (six technically inadequate echocardiographic evaluations) who were included in this study (97%).The cut-off point value of the measured/predicted LVM ratio with the best specificity and sensitivity in predicting adverse outcome (ROC analysis) was 110% (figure 1). Participants were thus classified in two subgroups defined iLVM and appropriate LVM if the measured/predicted LVM ratio exceeded or was 110% or less, respectively.

Receiver operating characteristic (ROC) curve for left ventricular mass considered as a percentage of predicted (ROC analysis). Area under the curve and CI are shown. The cut-off point identifying the subgroup of patients with an adverse outcome was 110%, (area under the curve 0.70; sensitivity 76%, specificity 61%).
iLVM was found in 129 patients (59%). These subjects were older and had lower blood pressure than their counterparts with appropriate LVM (table 1). Laboratory profiles and medications were similar between the two groups (data not shown). Considering the echocardiographic variables, patients with iLVM had higher relative wall thickness, greater LVM and lower stress-corrected midwall shortening than those with appropriate LVM (table 2). No patient had severe aortic regurgitation, which was mild to moderate in 24% of patients who had iLVM and in 29% of those who did not.
Baseline clinical characteristics of the study population (218 patients) divided according to LVM appropriateness
Baseline echocardiographic characteristics of the study poplation divided according to LVM appropriateness
Multiple logistic regression analysis revealed that iLVM was independently associated with greater LVM (OR 1.11; CI 1.07 to 1.16; p<0.001) and lower stress-corrected midwall fractional shortening (OR 0.84; CI 0.81 to 0.89; p<0.001). No clinical variable or any parameter of aortic valve severity was significantly related to iLVM at multivariate analysis.
Outcome
Follow-up information was available for 209 patients (96%). Nine patients (one with appropriate, eight with iLVM) were lost to follow-up. The survival analysis thus included 88 patients with appropriate and 121 patients with iLVM. At the end of follow-up (mean 22±13 months), 189 patients (90%) were alive. During this period, a clinical event occurred in 107 patients (51% of study population). Events were 20 deaths, 72 AVR (67 replacements by surgery and five catheter-based replacements) and 15 hospitalisations (myocardial infarction in two cases, CHF in 13 patients). Surgery was not decided upon in seven cases because of patient refusal; in other 10 cases the reason not to operate was very high perioperative risk of death (older age and heavy co-morbidities). The cumulative event-free survival in the whole study population was 77% at 1 year, 54% at 2 years, 37% at 3 years, 30% at 4 years and 28% at 5 years.
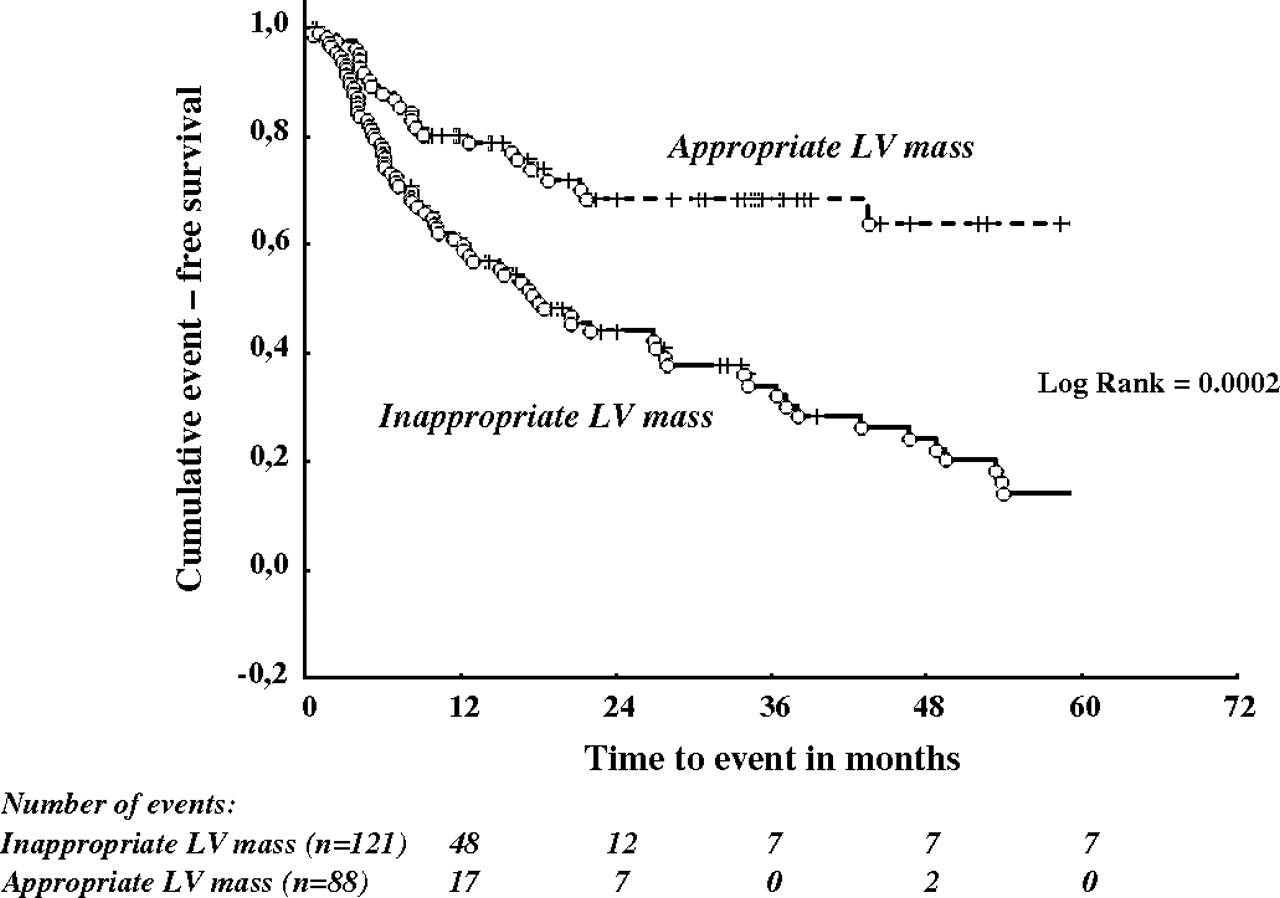
Considering the two study subgroups, a clinical event occurred in 81 patients with iLVM (67%) and 26 patients with appropriate LVM (30%) (p<0.001). Figure 2 shows the event-free survival curves of patients with appropriate and iLVM. Event-free survival in patients with appropriate and iLVM was 78% versus 56% at 1-year, 68% versus 41% at 2-year, 68% versus 29% at 3-year, 63%versus 14% at 4-year and 56% versus 10% at 5-year follow-up, respectively (all p<0.01).

Event-free survival curves in patients with appropriate (dotted line) or inappropriately high (continuous line) left ventricular (LV) mass.
Event-free survival curves were also analysed in tertiles of the measured/predicted LVM ratio; the probability of event-free survival was substantially higher in the lowest (cut-off point 108%) than in the intermediate and highest tertiles, which showed similar rates of events (figure 3).

Event-free survival curves in tertiles of deviation of left ventricular (LV) mass considered as a percentage of the measured/predicted ratio. There were 24 events in the lowest tertile (83 patients, 29%), 40 events in the medium tertile (67 patients, 60%) and 43 events in the highest tertile (59 patients, 73%).
Patients who died, underwent AVR or were hospitalised for non-fatal myocardial infarction or CHF were 16 (13%), 53 (45%), 12 (9%) in the iLVM group and four (4.5%), 19 (22%) and three (3%) in the appropriate LVM group, respectively. Cardiac aetiology could be identified in 16 of 20 deaths with a similar prevalence in the two groups (one sudden death and three deaths for pump failure in the appropriate LVM group; one sudden death and 15 deaths for pump failure in the iLVM group). The reason for the four non-cardiac deaths was pulmonary infection in two patients and remained unknown in two cases. In the 72 patients who underwent AVR, the reason for surgery was the appearance of symptoms in 59 patients, 44 of 53 patients (83%) with iLVM, and 15 of 19 patients (79%) with appropriate LVM (p=ns). Symptoms were described as syncope in four patients, angina in 10 patients and impairment of functional class (ie, dyspnoea during habitual physical activities) in 45 patients. The remaining 13 patients chose AVR despite the asymptomatic phase of the valve disease. All these 72 patients underwent coronary angiography before surgery. Ten of them (14%, five from each group) underwent coronary artery bypass grafting concomitantly to AVR. The mean duration of the follow-up was 19±15 and 26±18 months in patients with and without iLVM, respectively; p=0.03.
Inadequate LVM
Twenty-two patients had a measured/predicted LVM ratio below the 10th percentile and were classified as inadequate LVM. They had a low rate of events (six patients, 27%), which was similar to the group of patients with appropriate LVM.
Predictors of adverse outcome
Several differences at baseline evaluation emerged by univariate analysis between patients who experienced an adverse clinical event and those who did not during the follow-up (table 3). Conversely, haemoglobin, haematocrit, bilirubin, serum sodium and parameters of renal function were similar in the two groups (data not shown). Cox proportional hazard analysis included age, systolic blood pressure, diabetes, transaortic valve peak gradient, AVA, extent of aortic valve calcifications (calcium score), stress-corrected midwall shortening, LVM, LVH and iLVM. Valvulo-arterial impedance was forced in this model. This analysis identified iLVM as a strong predictor of adverse outcome independent of diabetes, higher transaortic peak gradient and greater extent of valve calcification (table 4, model 1). LVM, LVH and valvulo-arterial impedance did not enter into the final model. Identical results were found when the occurrence of symptoms was considered as an endpoint in place of AVR (59 patients of 72 who underwent valve replacement) and when iLVM was defined as observed/predicted LVM greater than 128% (data not shown).
Variables significantly related to adverse outcome: univariate Cox analyses
Cox proportional hazard multivariate analysis for prediction of adverse outcome
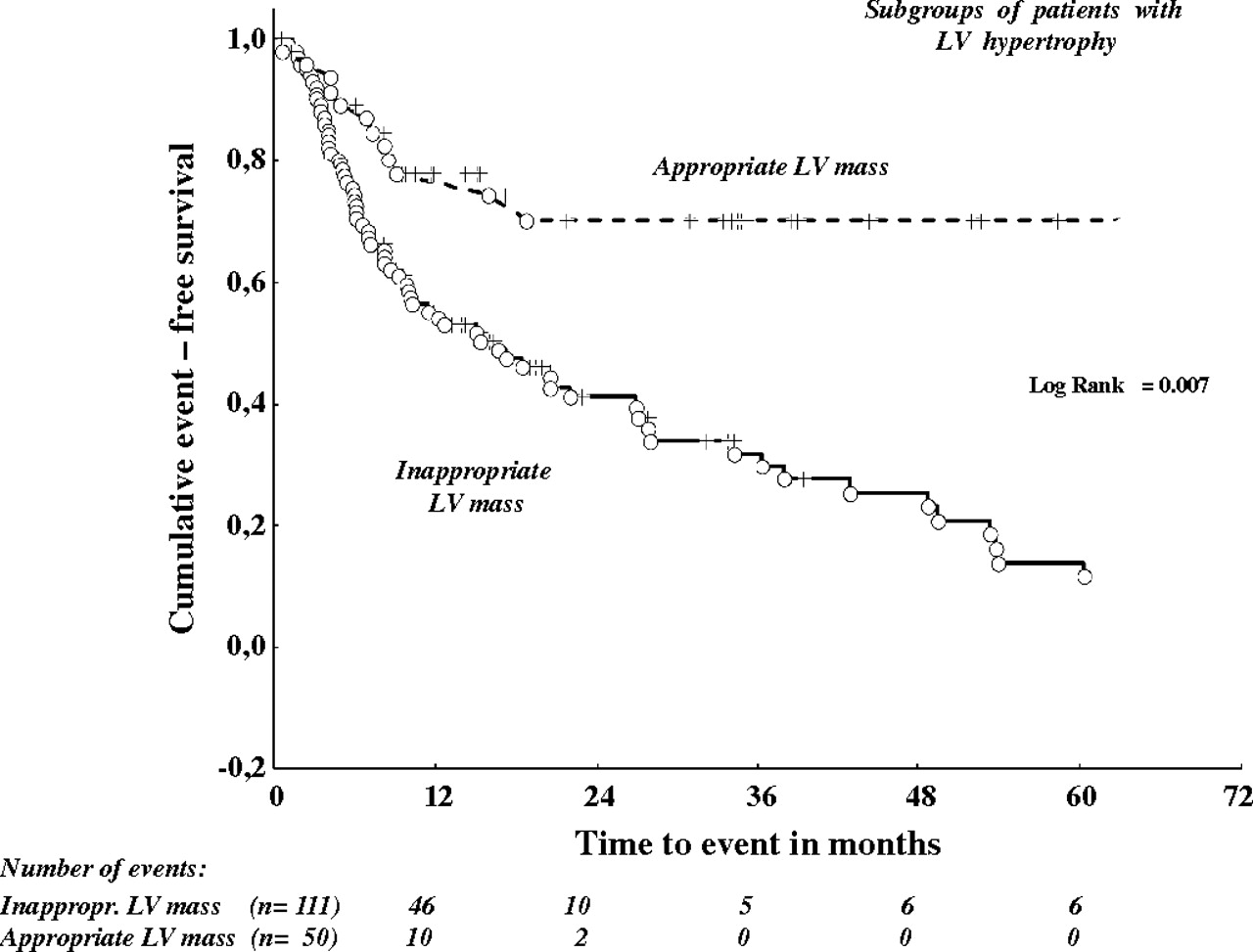
iLVM and LVH
LVH was detected in 163 patients (75% of the whole population). LVH showed a sensitivity and specificity for predicting an adverse event of 79% and 30%, respectively. Event-free survival (evaluated in 161) was significantly different in LVH patients with appropriate (n=50, rate of events 24%) or iLVM (n=113, rate of events 69%, p<0.001) (figure 4). The sensitivity and specificity of iLVM for adverse clinical events in the presence of LVH was significantly higher than traditional LVH (86% and 58%, respectively). The Cox model showed that among patients with LVH, those with iLVM had a 4.5-fold higher risk of adverse events than counterparts with appropriate LVM, independent of diabetes (Exp β 4.7; CI 2.29 to 9.70) and transaortic peak gradient (Exp β 1.02; CI 1.01 to 1.03). On the other hand, considering the subgroup of patients without LVH, the rate of events was similar between subjects with appropriate or iLVM (36% vs 50%, respectively; p=ns).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Event-free survival curves in patients with appropriate (dotted line) or inappropriately high (continuous line) left ventricular (LV) mass: subanalysis in the subgroup of 163 subjects with left ventricular hypertrophy.
Outcome without AVR
AVR is a problematical event as there may be a good deal of subjectivity involved in deciding on surgery, we also analysed outcome excluding AVR from the endpoint. Event-free survival in patients with appropriate and iLVM was 89% versus 90% at 1-year (p=ns), 78% versus 71% at 2-year (p=0.03), 78% versus 60% at 3-year (p<0.001), 78% versus 51% at 4-year and 78% versus 25% at 5-year follow-up (both p<0.001), respectively (log rank 0.04). Cox regression analysis identified iLVM as the strongest predictor of death for all causes or hospital admission for non-fatal myocardial infarction or CHF (table 4, model 2).
Discussion
The adjustment of LVM for left ventricular performance allows us to evaluate the appropriateness of LVM in response to cardiac work, and interpret the nature of compensatory LVH in patients with chronic left ventricular overload. iLVM has been basically investigated in patients with arterial hypertension.6–9 In these patients it is related to an adverse metabolic profile, concentric left ventricular geometry, left ventricular dysfunction and adverse prognosis. More recently, we demonstrated that iLVM was present in a significant portion of patients with AS5 and was associated with concentric left ventricular geometry and reduced left ventricular systolic function.
Excessive LVM and prognosis in AS
The present analysis identifies for the first time iLVM as a predictor of adverse outcomes in patients with AS, independent of diabetes, higher transaortic peak gradient and the extent of valve calcification, which are the well-known clinical and echocardiographic markers of poor outcome in these patients.10 11 20 23 24 Similarly to the MAVI trial,8 which investigated patients with arterial hypertension, the risk of adverse events in asymptomatic patients with severe AS significantly increases for values of measured LVM pretty near to the predicted ones, corresponding in our study to an excess of only 10% above the normal range found in previous studies.22 A survival analysis of patients classified in tertiles of the measured/predicted LVM ratio also confirms that a small growth of LVM, which is not in response to an increase in haemodynamic load, has to be considered pathological and harmful.
As already demonstrated in arterial hypertension,8 iLVM mainly identifies those patients with severe AS in whom greater LVM, concentric left ventricular geometry and impaired left ventricular function coexist. In these patients multiple pathophysiological mechanisms may explain the link between clinical events, left ventricular structural and functional alterations and excessive LVM. In severe AS, in fact, the coronary flow reserve is significantly reduced and preferential coronary flow shifts from endocardium to epicardium leading to subendocardial ischaemia.25 Abnormalities in sarcoplasmic reticulum calcium metabolism and in the cytoskeleton may arise and induce a contractile deficit responsible for the transition from compensated hypertrophy to hypertrophy with failure.26 Furthermore, as hypertrophy progresses, the non-contractile component of myocardium proportionally increases and fibrosis extends, contributing to left ventricular dysfunction.27 Finally, in this condition a simultaneous increase in myocardial oxygen and nutrients develops and may substantially contribute to the extension of ‘demand-side’ ischaemia independent of the presence of structural abnormalities in the proximal territories of the coronary arteries.28 All these mechanisms imply that myocardial ischaemia may often be a transient and reversible condition that could be availed by LVM reduction.10 11 28
Our patients with iLVM were older and had significantly more valve calcification than those without iLVM. These two variables were considered in the statistical analysis. In line with the results from other studies,21 24 age did not predict adverse events, possibly due to the fact that we mostly studied elderly people. In contrast, a higher calcium score was closely related to a poorer outcome. Similar findings were described by Rosenhek et al,21 who examined a younger cohort of patients with asymptomatic severe AS.
Interestingly, no correlation was observed between valvulo-arterial impedance and outcome in our study. This finding contrasts with results reported by Hachicha et al29 demonstrating that valvulo-arterial impedance improves risk stratification and clinical decision-making in patients with AS. The patients considered in our study all had severe AS and were homogeneous for global haemodynamic load, whereas the Hachicha population included both subjects with moderate and severe valve disease who greatly differed for global haemodynamic load. Different inclusion criteria may thus probably explain the different findings in the two studies.
Study limitations
Two main limitations of the present study have to be underlined. First, in patients with severe AS the predicted LVM might be overestimated by the method we used, which was validated in hypertensive individuals without CHF. In these patients left ventricular end-diastolic pressure was likely to be normal (near to zero) and was not considered in the estimation of stroke work. This would not be the case in some individuals with severe AS and concentric LVH. Second, AVR is a problematical outcome because an ample subjectivity (possibly conditioned by echocardiographic data) in managing these patients exists. However, the subanalyses performed in our population in which AVR was excluded or was placed by the occurrence of symptoms as an endpointminimised the possible effect of this limitation.
Conclusions
Although outcome varies largely, indications for surgery are well defined in the practical guidelines for patients with severe AS, and there is a consensus that an intervention has to be considered in the presence of symptoms, whereas it may be postponed in asymptomatic patients with preserved left ventricular systolic function.10 11 21 In these subjects, such a conservative approach is often justified by a high risk of surgery,30 which shifts the balance of the risk/benefit ratio towards waiting for symptom development. This attitude might also be favoured by the lack of information about reliable selection criteria of high-risk subgroups who would particularly benefit from early surgery, and also by the lack of prospective studies assessing specific therapeutic strategies. On the other hand, not infrequently in clinical practice, some physicians refer patients for AVR in the asymptomatic phase of the disease. This empirical behaviour, which also occurred in some patients enrolled in our study, could be induced by the subjective perception that the prognosis of these individual patients is truly worse than assessed.10 11 30 31 The results of the present study support this point of view. The truth of the matter is that, as of today, the management of asymptomatic patients with severe AS remains controversial. Previous studies identified aortic jet velocity and its changes during the time,23 24 functional status,24 the extent of valvular calcifications21 and an abnormal exercise test30 as markers of poor outcome, but no investigation prospectively testing a clinical management based on these parameters has so far been performed.
A more accurate risk stratification in these patients, however, should certainly be taken into account, considering that the development of symptoms represents a strong predictor of operative mortality and an urgent surgical procedure has a worse outcome than an elective one. In this view, it appears clinically relevant to have the use of a new simple variable such as iLVM, which may facilitate the identification of those having the worst outcome and who would benefit from elective surgery among patients with asymptomatic severe AS.