Article Text

Abstract
Objective Implantable cardioverter defibrillators (ICDs) are routinely used to prevent sudden cardiac death (SCD) in selected hypertrophic cardiomyopathy (HCM) patients, but the determinants of device-related complications, therapies and long-term cardiovascular mortality in ICD recipients are not known.
Design Retrospective observational cohort study.
Setting Single-centre tertiary referral cardiomyopathy clinic.
Patients 334 consecutively evaluated HCM patients (median age 40 years, 62% male, 92% primary prevention) at risk of SCD treated with ICD. Thirty-six patients (11%) received concurrent cardiac resynchronisation therapy for heart failure symptoms.
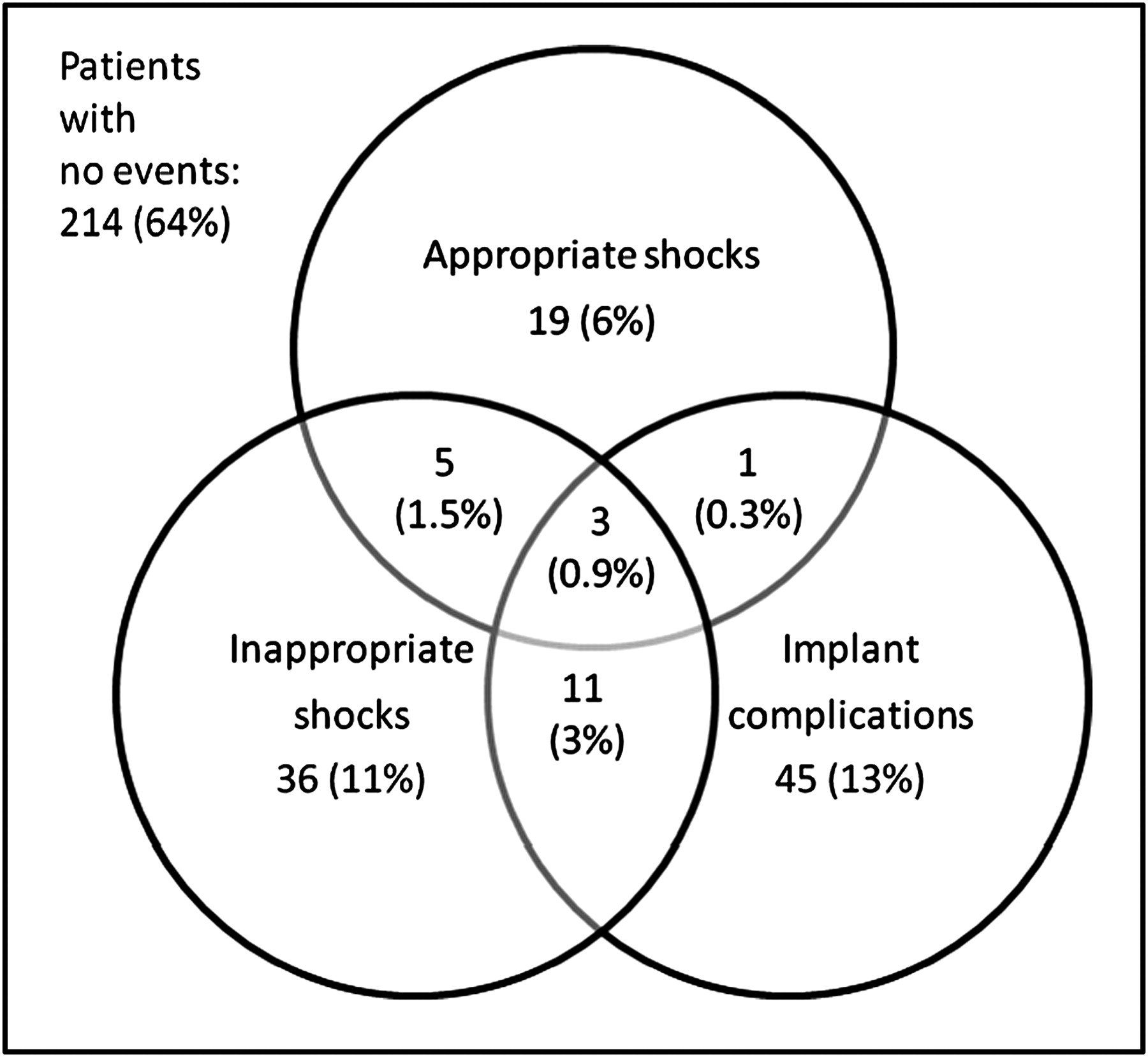
Results During the 1286 patient-years of follow-up, cardiovascular mortality (including transplantation) occurred in 22 (7%) patients (1.7%/year) and was associated with New York Heart Association (NYHA) class III/IV (adjusted HR=9.38, 95% CI 3.31 to 26.55, p≤0.001), percentage fractional shortening (HR=0.92, 95% CI 0.87 to 0.96, p=0.001) and implantation for secondary prevention (HR=0.07, 95% CI 0.01 to 0.86, p=0.04). There were no SCD. Twenty-eight (8%) patients received appropriate shocks (2.3%/year), which were predicted by baseline fractional shortening (HR=0.96, 95% CI 0.92 to 0.99, p=0.04). Fifty-five (16%) patients received inappropriate shocks (4.6%/year). Sixty (18%) patients experienced implant-related complications (5.1%/year), including two deaths. Adverse ICD-related events (inappropriate shocks and/or implant complications) were seen in 101 (30%) patients (8.6%/year). Patients with cardiac resynchronisation therapy were more likely to develop implant complications than those with single-chamber ICDs (HR=4.39, 95% CI 1.44 to 13.35, p=0.009) and had a higher 5-year cardiovascular mortality than did the rest of the cohort (21% vs 6%, p<0.001).
Conclusions HCM patients with an ICD have a significant cardiovascular mortality and are exposed to frequent inappropriate shocks and implant complications. These data suggest that new strategies are required to improve patient selection for ICDs and to prevent disease progression in those that receive a device.
- Implantable cardioverter defibrillators
- hypertrophic cardiomyopathy
- sudden cardiac death
- ventricular arrhythmias
- implant complications
- implantable cardioverter defibrillator (ICD)
- ventricular fibrillation
- ventricular tachycardia
- cardiomyopathy hypertrophic
Statistics from Altmetric.com
- Implantable cardioverter defibrillators
- hypertrophic cardiomyopathy
- sudden cardiac death
- ventricular arrhythmias
- implant complications
- implantable cardioverter defibrillator (ICD)
- ventricular fibrillation
- ventricular tachycardia
- cardiomyopathy hypertrophic
Introduction
Hypertrophic cardiomyopathy (HCM) is an inherited myocardial disease affecting 1 in 500 adults that, in a minority of patients, causes premature sudden death from ventricular arrhythmia.1 In patients with ischaemic heart disease and congestive cardiac failure, randomised controlled clinical trials have shown that implantable cardioverter defibrillators (ICDs) improve survival in particular subgroups.2 Similar data are lacking in patients with HCM, but based on the findings of observational studies,3 current guidelines recommend implantation of ICDs in HCM patients with a history of sustained ventricular arrhythmia or with clinical features associated with increased risk of sudden cardiac death (SCD).1 Data published to date indicate that patients treated in this way receive device therapies that successfully terminate potentially life-threatening ventricular arrhythmias.4–13 However, it is possible that the potential survival benefit afforded by appropriate ICD therapies might, in some patients, be offset by the consequences of a progressive decline in cardiac function14 and the lifetime risk of serious device-related complications.15
The aims of this study were to examine the long-term survival of HCM patients with ICD and to assess the risks and benefits of ICD therapy by determining the incidence and determinants of appropriate shocks, inappropriate shocks and implant-related complications.
Methods
Study design
A single-centre, observational, retrospective cohort design was used. The study conforms to the principles of the Helsinki Declaration. All patients gave written informed consent for ICD implantation. All authors have read and agreed to the manuscript as written.
Study population
The study cohort consisted of all consecutively evaluated HCM patients with an ICD who were attending a dedicated cardiomyopathy clinic. The unit was based at St Georges Hospital, London, UK, until 2003. The clinical service and patient care were subsequently transferred to The Heart Hospital, London, UK, from 2003 onwards. HCM was defined as unexplained hypertrophy (maximum left ventricular wall thickness (MLVWT) ≥15 mm) or in accordance with the criteria for the diagnosis of familial disease in patients with at least one first-degree relative with an unequivocal diagnosis.16 17 Only patients aged ≥16 years at the time of device implantation were included. Patients with Friedreich's ataxia, Noonan's syndrome and metabolic disorders were excluded.
Patient assessment, risk stratification and ICD implantation
Patients were evaluated throughout their follow-up using electrocardiography (rest and ambulatory), echocardiography and exercise testing as previously described.18 19 ICDs were implanted for primary prevention of SCD in the presence of one or more of the following major risk factors: family history of SCD attributed to HCM in one or more first-degree relatives, history of unexplained syncope, MLVWT ≥30 mm, non-sustained ventricular tachycardia on Holter monitoring and abnormal blood pressure response to exercise.1 18 A minority of patients were also considered at high risk in the presence of risk factors other than those specified by the current guidelines.1 Survivors of SCD and patients with sustained ventricular tachyarrhythmia received an ICD for secondary prevention.1
ICD implantation and defibrillation threshold testing were performed using conventional methods. All leads were intravenous, unless there was a contraindication. Treatment zones, antitachycardia and antibradycardia pacing were programmed on an individual patient basis.
Surveillance for ICD therapies and complications
ICD interrogation was performed every 6 months or earlier if there was a clinical event. All devices had the capacity to store intracardiac electrograms, and therapies were independently classified by two of the authors (CO and PL). Therapy was considered appropriate if the treated tachyarrhythmia was ventricular in origin. Ventricular fibrillation was defined as a ventricular arrhythmia with an irregular polarity, amplitude and morphology, with a mean cycle length of ≤240 ms. Ventricular tachycardia was defined as a ventricular arrhythmia with a regular or irregular polarity, amplitude and morphology, with a mean cycle length of >240 ms.7 All other therapies, including those triggered by self-terminating ventricular arrhythmias, were considered inappropriate. Atrial fibrillation was defined as irregular tachycardia with >60 ms variation between consecutive complexes with an identical electrographic morphology and polarity as sinus rhythm. Atrial flutter was defined as regular tachycardia with an identical electrographic morphology and polarity as sinus rhythm and a ventricular cycle length of 350 to 450 ms. Sinus tachycardia was defined as a gradual-onset regular tachycardia with an identical electrographic morphology and polarity as sinus rhythm and a mean ventricular rate above the programmed cut-off rate.7 Disagreement in interpretation was resolved using the above criteria.
The following device-implant-related complications were recorded: device-related infective endocarditis; pocket infection; superficial wound infection; device erosion; haematoma requiring intervention; device repositioning for cosmetic reasons, device migration or discomfort; lead failure secondary to fracture or insulation defects; lead displacement; device malfunction secondary to integral component, hardware or firmware failure of the generator; pericarditis; tamponade; pneumothorax/haemothorax; arterial embolisation; upper extremity venous thrombosis; pulmonary embolisation secondary to intravascular lead-related thrombus and severe tricuspid regurgitation. Complications were considered major if they caused death, required hospitalisation or required an additional procedure to revise the ICD.
End points
Five separate end points were independently considered: first appropriate ICD shock, first inappropriate ICD shock, first implant-related complication, first adverse ICD-related event (a combination of first inappropriate ICD shock therapy and first implant-related complication) and cardiovascular mortality. Cardiovascular mortality included SCDs (witnessed SCD with or without documented ventricular fibrillation or death within 1 h of new symptoms or nocturnal deaths with no antecedent history of worsening symptoms), heart failure deaths (death preceded by signs and/or symptoms of heart failure, including cardiogenic shock), heart transplantation for end-stage heart failure, stroke, pulmonary or peripheral arterial embolisation, death related to ICD implantation or another cardiac procedure and myocardial infarction. Deaths of unknown cause were classified as non-cardiovascular deaths.
Statistical analysis
SPSS (v17.0) and STATA (v10) were used for all statistical analyses. Normally distributed continuous data are expressed as mean±SD and as median and IQR for non-normally distributed data. The percentage of categorical data is shown in parentheses. Differences between means were compared using the Student t test and the Mann–Whitney U test for normally distributed and non-normally distributed continuous data, respectively.
For time-to-event analysis, the follow-up period was calculated from the date of device implantation to the end point of interest. In patients without an event, the follow-up period extended to the most recent ICD evaluation or censoring event up to 14th January 2010. The annual event rate was calculated by dividing the number of patients reaching an end point by the total follow-up period for that end point. The cumulative probability for the occurrence of an outcome was estimated using the Kaplan–Meier method. The relation of outcomes to baseline clinical characteristics (predictor variables) was assessed using the Cox proportional hazards model. The predictor variables were prespecified on the basis of previously published studies, to minimise the likelihood of noise variables from being included in the final models.20 A univariable preselection process was used to identify predictor variables for subsequent multivariable analyses. To prevent weak predictors from being excluded from the multivariable models, the univariable preselection process was based on a high significance level of 50%. Interactions between the final predictors were sought, and the linearity assumption for continuous variables was tested using models with quadratic polynomial terms.21
The influence of the following predictor variables on cardiovascular mortality was considered initially with univariable and then multivariable analysis: age at the time of device implantation, male sex, ICD indication (primary or secondary), New York Heart Association (NYHA) functional class, fractional shortening (FS) (%), left atrial diameter (mm), left ventricular outflow tract gradient (LVOTG) ≥50 mm Hg and history of atrial fibrillation. The relation between age at the time of device implantation, male sex, ICD indication, MLVWT (mm), FS (%), LVOTG ≥50 mm Hg, amiodarone treatment and appropriate ICD therapy was examined in a similar fashion. The predictor variables used in the analysis of inappropriate ICD therapies were as follows: age at the time of device implantation, male sex, atrial fibrillation, left atrial diameter (mm), amiodarone treatment and the type of device (single- vs dual-chamber ICD). Finally, the contribution of age at the time of device implantation, male sex, warfarin treatment and the complexity of the device (dual-chamber and biventricular devices vs single-chamber ICDs) to implant-related complications was investigated.
HRs, 95% CIs and p values are presented. A two-sided p value <0.05 was considered significant.
Results
Three hundred and seventy HCM patients with an ICD were identified, but 36 were excluded from the study because their ICD follow-up was carried out at other centers, and access to complete medical records was not possible. The final study cohort consisted of 334 patients: 307 patients (92%) received a device for primary prevention of SCD and 27 patients (8%) for secondary prevention. The baseline clinical characteristics tabulated according to implant indication and survival status are shown in table 1. Three hundred and twenty-two patients (96%) fulfilled the conventional diagnostic criteria for HCM, and 12 patients (4%) fulfilled familial criteria.17
Baseline clinical characteristics and clinical outcomes
The devices were implanted between 4th April 1992 and 1st June 2009: 10 devices were implanted between 1992 and 1996 (6/10 (60%) for secondary prevention), 29 were implanted between 1996 and 2000 (6/29 (21%) for secondary prevention), 124 were implanted between 2000 and 2005 (13/124 (10%) for secondary prevention) and 171 were implanted between 2005 and 2009 (2/171 (1%) for secondary prevention). Forty-eight patients (14%) received an ICD prior to their first evaluation at our unit. All ICD interrogation records were available for assessment. An atrial lead was implanted in 86% of patients. In addition to an ICD, 19 patients (6%) who had heart failure symptoms at the time of ICD implantation received cardiac resynchronisation therapy (CRT): 9 (47%) of 19 with impaired systolic function (ejection fraction <50%) and 10 (53%) of 19 with preserved systolic function. During follow-up, 17 patients (5%) with single- or dual-chamber ICD implanted for the prevention of SCD developed heart failure symptoms, and their devices were upgraded to CRT–ICD: 9 (53%) of 17 with impaired systolic function and 8 (47%) of 17 with preserved systolic function.
Cardiovascular mortality
During a follow-up period of 1286 patient-years (median 3.6 years, IQR 1.8 to 5.2 years, range 6 days to 17.6 years), 22 patients (7%) reached the cardiovascular mortality end point (1.7%/year, 95% CI 1.0 to 2.4; 5-year cumulative incidence 8%, 95% CI 4 to 12). The cardiovascular mortality end point included 11 cardiac transplants for end-stage heart failure (mean±SD age 49±10 years, 8/11 (73%) with impaired systolic function), 6 heart failure deaths (mean±SD age 53±17 years, 5/6 (83%) with impaired systolic function), 1 death (age 40 years) due to pulmonary embolisation following surgery, 1 death that occurred after peripheral arterial embolisation in a 54-year-old patient and 1 death that resulted from stroke in a patient aged 70 years. Two primary prevention patients died of ICD-related complications: a 24 year old from cardiac tamponade 6 days following device implantation and a 25 year old from intrathoracic bleeding during an intravascular lead extraction for device-related infective endocarditis, 3.6 years post-device implant. In the 22 patients who reached the cardiovascular mortality end point, the median time from device implantation to reaching the end point was 1.7 years (IQR 1.1 to 3.9 years, range 6 days to 15.1 years). Only 1 of the 27 secondary prevention patients reached the cardiovascular death end point after 15.1 years of follow-up (heart transplant). The cause of death in one secondary and two primary prevention patients could not be determined because of lack of information. Two patients died from non-cardiac causes (malignancy and complications of alcohol consumption).
Multivariable analysis identified three independent predictors of reaching the cardiovascular mortality end point: NYHA functional class, FS and device indication (table 2). FS at the time of ICD implantation was inversely related to the risk of cardiovascular death/transplant, with a 10% decrease in FS associated with a 57% (95% CI 34 to 75) increase in risk. The linearity assumption for FS was not violated (p=0.38). The interaction effect of implant indication with FS and NYHA III/IV was not significant (p=0.80 and p=0.99, respectively). The mean FS was similar in NYHA I/II and NYHA III/IV patients (38%±9% and 37%±13%, respectively; p=0.69). The Kaplan–Meier curve for primary and secondary prevention patients is shown in figure 1A. In the subgroup of patients with normal systolic function at baseline (n=301), FS (HR=0.92, 95% CI 0.85 to 0.99, p=0.03) and NYHA III/IV (HR=5.4, 95% CI 1.63 to 18.33, p=0.006) remained independent predictors of reaching the cardiovascular mortality end point.
Univariable and multivariable regression models

Kaplan–Meier curves for survival free from cardiovascular mortality end point (A) stratified according to device implantation for primary or secondary prevention, appropriate shocks (B) stratified according to impaired systolic function, inappropriate shocks (C), implant complications (D) stratified according to device complexity, implant complications in patients with single- or dual-chamber ICDs (cardiac resynchronisation therapy patients excluded) (E), implantable cardioverter defibrillator-related adverse events (inappropriate shocks or implant complications) for the whole cohort (F).
Appropriate ICD shocks
The rate of appropriate ICD shocks was 2.3%/year (95% CI 1.4 to 3.1), with a 13% 5-year cumulative incidence (95% CI 7 to 19). Appropriate ICD shocks were delivered to 21 (7%) primary and 7 (26%) secondary prevention patients, with an appropriate shock rate of 2.0%/year (95% CI 1.1 to 2.8) and 4.3%/year (95% CI 1.2 to 7.4), respectively. The 5-year cumulative incidence of appropriate ICD shocks was 12% (95% CI 6 to 18) for primary prevention and 20% (95% CI 4 to 36) for secondary prevention patients. Of the patients who received appropriate ICD shocks, 12 (42%) had additional appropriate shocks during follow-up. Ventricular fibrillation was the cause of appropriate ICD shocks in 52% of cases. The median time from implantation to the first appropriate shock was 2.1 years (IQR 0.7 to 3.9 years, range 35 days to 6.8 years). Of the 22 patients who reached the cardiovascular end point, 2 (9%) received an appropriate shock. Of the 12 patients diagnosed as having HCM based on familial criteria,17 1 (8%) received an appropriate shock.
In the multivariable analysis (table 2), FS was the only independent predictor for receiving an appropriate ICD shock. A 10% decrease in FS was associated with a 34% (95% CI 10 to 57) increase in risk when adjusted for other factors. The linearity assumption for FS was not violated (p=0.56). The Kaplan–Meier curve showing the appropriate ICD shock-free survival for patients with reduced FS is shown in figure 1B.
The relation between clinical risk factor profile in the 307 primary prevention patients (table 3) and appropriate ICD shocks was also examined. There was no relation between the number of risk factors and appropriate shock rate (HR=0.97, 95% CI 0.45 to 2.11, p=0.94, for patients with two to three risk factors; HR=0.0, 95% CI 0.0 to ∞, p=0.98, for patients with four or more risk factors, compared to those with no or one major risk factor). Of the 11 patients with no major risk factors, 1 (9%) had an appropriate shock.
The risk factors for SCD in 307 primary prevention patients
Inappropriate ICD shocks
Inappropriate shocks were delivered to 55 patients (16%), with a discharge rate of 4.6%/year (95% CI 3.4 to 5.8) and a 21% 5-year cumulative incidence (95% CI 15 to 27). Seventeen of the patients receiving an inappropriate ICD shock (31%) had recurrent inappropriate therapies during their follow-up. The median time from implantation to the first inappropriate shock was 1.1 years (IQR 0.5 to 2.7 years, range <1 day to 5.6 years).
Inappropriate shocks were triggered by atrial fibrillation/flutter (51%), sinus tachycardia (24%), supraventricular tachycardia (11%), lead failure or displacement (8%), self-terminating ventricular tachycardia (4%) and T-wave oversensing (2%). Multivariable analysis did not identify independent predictors for inappropriate ICD shocks (table 2); patients with single-chamber devices were not more likely to receive an inappropriate shock than those with an atrial lead. The Kaplan–Meier curve showing survival free from inappropriate ICD shocks is shown in figure 1C. Compared with patients implanted during the most recent implant quartile (2005–2009), patients with earlier ICD implants did not have a higher inappropriate shock rate (2000–2005 implants: HR=0.59, 95% CI 0.32 to 1.07, p=0.08; 1996–2000 implants: HR=0.87, 95% CI 0.37 to 2.03, p=0.75; 1992–1996 implants: HR=0.00, 95% CI 0.0 to ∞, p=0.96).
Implant-related complications
Sixty patients (18%) experienced an ICD implant-related complication at a rate of 5.1%/year (95% CI 3.8 to 6.3), with a 21% 5-year cumulative incidence (95% CI 15 to 27). A total of 73 implant-related complications were observed (table 4). Lead failure was the most common implant-related complication with a 5-year cumulative incidence of 6% (95% CI 2 to 10). Forty-eight patients (14%) were affected by 54 complications that were classified as major. There were no deaths related to failed defibrillation threshold testing. Compared with those patients undergoing ICD implantation during the most recent implant quartile (2005–2009), patients with early ICD implants did not have a higher implant complication rate (2000–2005 implants: HR=0.62, 95% CI 0.35 to 1.08, p=0.09; 1996–2000 implants: HR=0.19, 95% CI 0.05 to 0.70, p=0.01; 1992–1996 implants: HR=0.00, 95% CI 0.0 to ∞, p=0.96). Patients who had a device implanted at another institution (n=48) prior to their assessment in our unit did not have a higher complication rate (HR=1.11, 95% CI 0.57 to 2.13, p=0.76). Compared to patients with single-chamber ICDs, those with CRT–ICD were more likely to experience implant-related complications when adjusted for other predictor variables (table 2). Implant-related complication-free survival according to device complexity is shown in figure 1D. Of the 298 patients without CRT, 47 (16%) had an implant complication with an annual rate of 4.4% (95% CI 3.2 to 5.6) and a 19% 5-year cumulative incidence (95% CI 13.2 to 24.9). The Kaplan–Meier curve is shown in figure 1E.
Implant-related complications
Adverse ICD events
One hundred and one patients (30%) experienced either an inappropriate ICD therapy or an implant-related complication with an annual rate of 8.6% (95% CI 7.0 to 10.2) and a 34% 5-year cumulative incidence (95% CI 28 to 40). The Kaplan–Meier curve showing survival free from device adverse events for the whole cohort is shown in figure 1F; figure 2 summarises the outcomes. Of the 298 patients without CRT, 86 (29%) had either an inappropriate ICD therapy or an implant-related complication with an annual rate of 8.1% (95% CI 6.5 to 9.7) and a 34% 5-year cumulative incidence (95% CI 28 to 40).
The experience of hypertrophic cardiomyopathy patients treated with implantable cardioverter defibrillators.
Implant complications and adverse ICD events in CRT recipients
In the 36 patients with CRT–ICD, 13 (50%) experienced an implant complication with an annual rate of 11% (95% CI 5.5 to 17.2) and a 36% 5-year cumulative incidence (95% CI 18.4 to 53.6). Lead failure and displacement were responsible for 60% of implant complications in this subgroup. Fifteen patients (42%) had either an inappropriate ICD therapy and/or an implant-related complication with an annual rate of 13.0% (95% CI 6.9 to 19.3) and a 39% 5-year cumulative incidence (95% CI 21.4 to 56.6). Of the 15 patients with adverse ICD events, 5 (30%) had an appropriate ICD shock. The main outcomes of the study stratified according to device type are summarised in table 5. Patients with CRT–ICD had a higher cardiovascular mortality and appropriate ICD shock rate but with similar rate of inappropriate shocks compared to ICD-only patients.
The main outcomes of the study stratified according to device type
Discussion
This study is the first to explore the determinants of long-term survival in HCM patients treated with ICDs for the prevention of SCD. The major finding is that ICD recipients are at high risk of heart failure-related mortality, as well as morbidity from inappropriate shocks and implant-related complications. Survivors of SCD that received ICDs for secondary prevention had a better long-term outcome than those implanted for primary prevention. Complex devices were associated with a higher rate of implant-related adverse events, and the use of atrial leads did not reduce inappropriate shock rates.
Even though SCD has previously been reported in HCM-ICD recipients,8 10 13 22 this was not observed in our study, providing further support for the effectiveness of ICD in terminating potentially lethal ventricular arrhythmias. However, as a consequence of this success, heart failure with or without systolic impairment has emerged as the leading cause of cardiovascular mortality in this population. Most data suggest that HCM is characterised by progressive loss of myocardial performance over many decades.23–26 Even when symptoms of heart failure develop, the time to diagnosis of severe systolic impairment is still about 10–15 years.24 25 This decline in systolic function is often overlooked because the majority of patients are asymptomatic in the early stages, and conventional indices of cardiac performance remain within the normal range.27 In addition, a significant portion of HCM patients develop heart failure with preserved systolic function.25 The findings in this study indicate that ICD recipients are at high risk of heart failure death or transplantation and illustrate the need for new strategies to prevent disease progression, for example, by reducing ischaemia28 or modulating fibrotic pathways activated by sarcomere protein mutations.29
With a limited supply of heart transplant donors, the use of CRT in HCM patients with refractory heart failure symptoms is likely to increase. In a small observational study, we have previously shown that CRT improves symptoms and ejection fraction in 40% of HCM patients with impaired systolic function.30 In this study, all patients had an ICD implant because they were thought to be at high risk of SCD, but in addition, some patients with concurrent heart failure symptoms received CRT for conventional indications2 or as part of a randomised trial (http://clinicaltrials.gov identifier: NCT00504647). As this study shows, this is an important subgroup of patients who have a high risk of SCD and high cardiovascular mortality. In common with a recent registry study, implantation of complex devices was also associated with a higher implant complication rate.31 This is likely to relate to the more technically demanding nature of CRT–ICD implantation leading to an excess of lead-related complications.
The appropriate ICD shock rate in our cohort is lower than that reported in other studies (table 6, figure 3).4–13 This might be explained by differences in patient characteristics, in particular, baseline ventricular function, but a comparative analysis of this variable could not be performed as previous studies did not uniformly report on indices of systolic function. The exclusion of paediatric patients in this study may also play a role. For example, Begley et al4 reported a higher rate of appropriate ICD shocks in those aged <21 and >40 years. A similar association with age was reported in an earlier study by Maron et al,7 but in a subsequent analysis of a larger cohort by the same authors, there was no relation between age at implantation and risk of appropriate discharge in primary prevention patients.8 In the current analysis, there was no association between age at implant and the risk of appropriate ICD shocks. Finally, the incidence of appropriate therapies could reflect differences in medical therapy, particularly antiarrhythmic medication and ICD programming.32
Summary of previously published studies

{kind=link}
{kind=link}
{kind=link}
Forest plot of random effect meta-analysis with adjusted weight ratios of previously reported appropriate shock rates. The size of the box depends on the weight estimated for each study by the random effect model (Der Simonian and Laird). The CIs of each study are also shown. The overall appropriate shock rate is 4.6%/year (95% CI 3.1 to 6.1). Maron et al 20078 include 150 previously reported patients in Maron et al 20007 and Jayatilleke et al.5 The studies by Primo et al9 and Begley et al4 were not included as the annual appropriate shock rate was not available.
Published studies of ICDs in HCM patients (table 6), although diverse in design, have uniformly reported a higher incidence of appropriate ICD shocks in patients with devices implanted for secondary rather than primary prevention.4–13 The same was true of our univariable analysis, but when adjusted for other potential modulators of the arrhythmogenic substrate, ICD implantation for secondary prevention was no longer a predictor. Instead, fractional shortening emerged as the only independent predictor for appropriate shocks and, along with NYHA functional class at the time of ICD implantation, also predicted cardiovascular mortality. Even though FS does not reflect global systolic function accurately, these observations suggest that it is the severity of the underlying myocardial disease at the time of ICD implant rather than the indication for the ICD which is the major determinant of long-term outcomes.
Despite advances in ICD technology, inappropriate shocks remain a problem in a substantial number of patients (table 6). Young age and a history of atrial fibrillation have been associated with a higher risk for inappropriate ICD shocks,6 10 but we could not confirm this observation. In keeping with previous reports in HCM patients,6 13 the use of atrial leads did not reduce inappropriate shocks, and their use has been associated with more implant-related complications in other cardiac conditions.31 This indicates that in the absence of a specific indication for atrial pacing or the need for sequential atrioventricular pacing for left ventricular outflow tract symptoms,33 34 single-lead systems should be implanted preferentially.
Although the aggregation of risk factors in an individual patient is thought to reflect the severity of disease and ultimately the risk of SCD,1 the rate of appropriate ICD shocks in this and previous studies8 13 was unrelated to the risk factor profile. This seems counterintuitive, given the fact that there is strong and consistent evidence that accumulating risk factors equate with higher risk of SCD.18 35–37 There are various possible explanations for this discrepancy. The most obvious is that the end point of our analysis was an appropriate ICD shock and not SCD per se, and the assumption that all appropriate ICD discharges are equivalent to SCD is likely to be flawed.32 38 Another more subtle explanation is the failure to seek additional risk factors when there are already sufficient reasons to implant an ICD; for example, once two risk factors are detected, doctors are less likely to search for the three other remaining risk factors as this does not alter decision making. In addition, the existing approach to risk estimation was developed to distinguish high- from low-risk patients rather than stratifying risk further within the high-risk group (ie, in those with an ICD).
Finally, this is not a validation study of the existing algorithm since it does not consider SCD in patients who were judged to be at low risk and did not receive an ICD or in high-risk patients who declined ICD implantation. Nevertheless, we acknowledge that there is a need for a new, validated clinical risk prediction model that provides patients and doctors with individualised absolute risk estimates for disease outcomes. This approach has already been used for outcomes in cardiothoracic surgery (European System for Cardiac Operative Risk Evaluation).39 In addition to routinely used clinical parameters, novel genetic,40 electrophysiological41 and imaging parameters42 may improve prognostic accuracy.
Study limitations
Retrospective data collection restricted the selection of predictor variables to those that were routinely collected at the time of the first implant. The effects of some predictor variables at baseline are difficult to assess. For example, our cohort was not systematically screened for latent LVOTG using stress echocardiography.43 Amiodarone treatment initiated or discontinued after implantation was not considered in the analysis. Information on training and experience of the implanter was sought but was not available. Psychological complications such as depression and anxiety were not included in our analysis.44
While all patients in this study received an ICD because they were deemed to be at increased risk of SCD by their treating cardiologist, a subgroup also received CRT therapy. A lack of randomized control trial data in this setting means that HCM is not specifically considered in the current guidelines for CRT.2 Because of a concern that their inclusion could have skewed the overall data set, we performed a subanalysis in patients not receiving CRT (table 5). While patients with CRT–ICD had a higher cardiovascular mortality, appropriate shocks and implant complications, outcomes in the ICD-only subgroup were similar to those observed in the overall cohort, and the inclusion of CRT–ICD patients does alter the conclusions and clinical implications of this study.
Conclusions
The high incidence of heart failure death and cardiac transplant in ICD recipients emphasises the need for new strategies to prevent disease progression. Careful consideration should be given to the complexity of the device prescribed and meticulous care at all stages of management from patient selection, implantation and follow-up (ICD programming and medical therapy) to minimise inappropriate therapies and long-term complications.
Acknowledgments
We are indebted to Dr Alison Muir, Dr Caroline Coats, Dr Juan Gimeno, Dr Antonios Pantazis, Dr Maite Tome-Esteban and Ms Shaughan Dickie for their support.
References
Footnotes
See Editorial, p 97
Funding This research was supported by grants from the Spanish Society of Cardiology (to Dr Cardona), European Society of Cardiology (to Dr Calcagnino and Dr Quarta) and Hellenic Society of Cardiology (to Dr Tsovolas). This work was undertaken at The Heart Hospital (University College London Hospitals NHS trust)/University College London, which received a proportion of funding from the Department of Health's National Institute for Health Research (NIHR) London Biomedical Research Centres funding scheme.
Competing interests Dr Lambiase received support from St Jude, and Dr Elliott received fees from Medtronic. All other authors have no potential conflicts of interest to declare.
Ethics approval Ethics approval not required under NHS research governance arrangements.
Provenance and peer review Not commissioned; externally peer reviewed.