Article Text

Abstract
Objective To explore the relationship between serum phosphate, arterial stiffness and left ventricular mass (LVM) in patients with early-stage chronic kidney disease (CKD).
Design A cross-sectional observational study.
Setting Single centre.
Patients 208 patients with stage 2 to stage 4 non-diabetic CKD.
Interventions Arterial stiffness was determined through measurement of aortic pulse wave velocity (PWV). Cardiac magnetic resonance was used to determine LVM.
Main outcome measure Relationship between serum phosphate, aortic PWV and LVM.
Results Mean age was 54±13 years, mean glomerular filtration rate was 50±15 ml/min/1.73 m2, mean serum phosphate was 1.11±0.21 mmol/l and mean PWV was 8.6±2.1 m/s. When the cohort was divided into quartiles according to serum phosphate, LVM increased across quartiles (p=0.04), with no significant differences in age, kidney function, blood pressure or PWV. Serum phosphate correlated with LVM (r=0.173; p=0.01), but PWV did not (p=0.2). In a regression model containing gender, serum phosphate, office systolic blood pressure, albumin/creatinine ratio and haemoglobin, 30% of the variation in LVM was explained (p<0.0005), with serum phosphate accounting for 5% of the variance.
Conclusion Serum phosphate is independently associated with LVM in patients with CKD. Interventional studies are required to determine whether this association is causative and whether reducing phosphate exposure reduces LVM in this population.
- Aortic stiffness
- cardiac MRI
- cardiovascular risk
- left ventricular mass
- phosphate
- acute coronary syndrome
- aortic disease
- transthoracic
- MRI
- ventricular hypertrophy
- cardiomyopathy
- renal diseases
- cardiovascular disease
- ventricular function
- arterial wall morphology
- echocardiography
- risk factors
- EBM
- endothelium
- imaging and diagnostics
- atrial fibrillation
- pulmonary valve disease
- depression
- tricuspid valve disease
- valve disease
- aortic valve disease
- nuclear cardiology
- tissue Doppler
- echocardiography (transoesophageal)
- acute myocardial infarction
- autonomic regulation
- heart failure
- haemodynamics
- pharmacokinetics/pharmacodynamics
- endothelium
- renin–angiotensin system
Statistics from Altmetric.com
- Aortic stiffness
- cardiac MRI
- cardiovascular risk
- left ventricular mass
- phosphate
- acute coronary syndrome
- aortic disease
- transthoracic
- MRI
- ventricular hypertrophy
- cardiomyopathy
- renal diseases
- cardiovascular disease
- ventricular function
- arterial wall morphology
- echocardiography
- risk factors
- EBM
- endothelium
- imaging and diagnostics
- atrial fibrillation
- pulmonary valve disease
- depression
- tricuspid valve disease
- valve disease
- aortic valve disease
- nuclear cardiology
- tissue Doppler
- echocardiography (transoesophageal)
- acute myocardial infarction
- autonomic regulation
- heart failure
- haemodynamics
- pharmacokinetics/pharmacodynamics
- endothelium
- renin–angiotensin system
Introduction
Phosphate has recently emerged as a novel cardiovascular risk factor.1 Serum phosphate levels, while still within the reference range, are associated with increased cardiovascular morbidity and mortality in the general population, as well as in patients with cardiovascular disease, early chronic kidney disease (CKD) and end-stage kidney disease (ESKD).1 2 The mechanism of this association is currently unknown. It has been postulated that phosphate might affect cardiac structure and function indirectly through promotion of vascular calcification and an increase in arterial stiffness,1 2 but direct effects on the myocardium, such as cardiac fibrosis and ventricular hypertrophy, have also been demonstrated.3 4 Left ventricular hypertrophy (LVH) is an established predictor of cardiovascular mortality and all-cause mortality in a number of different patient populations, including CKD.5 There is also emerging evidence that left ventricular mass (LVM), assessed as a continuous variable, has prognostic value in predicting cardiovascular disease.6 Reductions in LVM have been associated with reduced mortality in a variety of groups at high cardiovascular risk.7
CKD is present in 13% of the adult population in Western societies and is the commonest condition associated with disordered phosphate regulation.8 Patients with CKD have an increased cardiovascular risk at estimated glomerular filtration rates (eGFRs) below 60 ml/min/1.73 m2—and possibly below 90 ml/min/1.73 m2—that cannot be fully explained by 'traditional' risk factors.2 These individuals are more likely to die from cardiovascular disease than from progress to ESKD.2 The majority of cardiovascular deaths in late-stage CKD are attributable to sudden cardiac death, arrhythmia or congestive heart failure, with occlusive vascular disease being accountable for only a small proportion of deaths.2 Structural heart disease, such as LVH, acts as a substrate for the development of congestive heart failure and sudden cardiac death, and is the leading cause of cardiovascular mortality in both ESKD and early-stage CKD. The relationship between serum phosphate, arterial stiffness and LVM in patients with CKD is unclear. We hypothesise that phosphate is linked to increased LVM in CKD and that this association is mediated through an increase in arterial stiffness.
Methods
Study design, setting and participants
We recruited adult patients with CKD from renal clinics at the Queen Elizabeth Hospital Birmingham (Birmingham, UK) for a cross-sectional cohort study. Patients were included if they were aged 18–80 years; had stage 2 (glomerular filtration rate (GFR) 60–89 ml/min/1.73 m2 and evidence of kidney damage for ≥3 months), stage 3 (GFR 30–59 ml/min/1.73 m2) or stage 4 (GFR 15–29 ml/min/1.73 m2) CKD9; and had no change in medication in the preceding 3 months. Patients with diabetes mellitus, uncontrolled blood pressure (mean daytime ambulatory blood pressure >130/85 mm Hg), atrial fibrillation, known left ventricular dysfunction, valvular disease, signs and symptoms of congestive heart failure, and a history of cardiovascular disease were excluded. The presence of cardiovascular disease was defined as a history of myocardial infarction, treatment for angina, angiographically proven coronary artery disease, coronary artery bypass graft, percutaneous coronary intervention, haemorrhagic stroke, ischaemic stroke, transient ischaemic attack, carotid artery revascularisation, intermittent claudication, angiographically proven peripheral artery disease, aortic aneurysm, angiographically proven renal artery stenosis or renal artery revascularisation. Patients receiving treatment with a phosphate binder or vitamin D analogue were also excluded. The study was approved by the West Midlands Research ethics committee, and all participants gave written informed consent.
All subjects underwent baseline investigations, including measurement of height and weight and collection of serum and plasma. GFR was estimated by the four-variable Modification of Diet in Renal Disease formula, with serum creatinine recalibrated to be traceable by an isotope-derived mass spectroscopy method.10 Serum calcium levels were corrected for serum albumin. Albuminuria was measured using spot albumin/creatinine ratio (ACR). Office blood pressure was measured with a validated oscillometric sphygmomanometer (Dinamap Procare; GE Healthcare, Hatfield, UK) as per British Hypertension Society guidelines.11 All subjects underwent 24 h ambulatory blood pressure measurement (Meditech ABPM-04; PMS Instruments, Maidenhead, UK). Arterial stiffness was assessed using the gold-standard measurement of carotid–femoral pulse wave velocity (PWV) (SphygmoCor; AtCor Medical, Sydney, Australia) as previously described using a high-fidelity micromanometer (SPC-301; Millar Instruments, Texas, USA) to sequentially record electrocardiographically gated carotid and femoral waveforms following 15 min of supine rest.12
Cardiac MRI
Cardiovascular MRI was performed on a 1.5 T scanner (Sonata; Siemens, Erlangen, Germany). Serial contiguous short-axis cines were piloted from the vertical long axis and the horizontal long axis of the left ventricle (electrocardiographically gated steady-state free precession imaging (True-FISP); temporal resolution 40–50 ms, repetition time 3.2 ms, echo time 1.6 ms, flip angle 60°, slice thickness 7 mm) in accordance with previously validated methodologies.13 For measurements of left ventricular function, volume and LVM, analysis was performed offline (Argus Software; Siemens).13 LVM was indexed (left ventricular mass index (LVMI)) to body surface area (Mosteller formula: BSA (m2)= √((weight (kg)×height (cm))/3600). LVH was defined as an LVMI greater than age-corrected and gender-corrected limits.13
Statistical analysis
Statistical analysis was performed using SPSS V.16.0. Data distribution was tested using the Kolmogorov–Smirnov test. Non-normally distributed data were log-transformed before analysis and, if still not normally distributed, analysed with non-parametric tests. Continuous data were compared by Student t test or analysis of variance, and categorical data were compared by Pearson's χ2 test. Data are expressed as mean±SD or as median (IQR). Parametric correlations were calculated using Pearson's correlation, and non-parametric correlations were calculated using Spearman's test. Linear regression was used to assess the relationship between continuous variables. Colinearity between explanatory variables was assessed by examining the variance inflation factor, with a variance inflation factor >5 suggesting relevant colinearity. Reproducibility of LVMI was determined using intraclass correlation coefficient and a two-way random-effects model. A type I error rate below 5% (p<0.05) was considered statistically significant.
Results
Demographics
Of 3349 patients screened, 736 patients met the study entry criteria. Five hundred and twenty-eight patients declined the study; therefore, 208 subjects were recruited. Renal diagnoses and the prescribed medications of the entire cohort are shown in table 1. The patients were taking 1.8±1.2 (mean) anti-hypertensive agents, with 89% of the patients either on an ACE inhibitor or an angiotensin receptor blocker. No patients were taking erythropoietin-stimulating agents. Among the patients, 57% were male, 86% were Caucasian, 10% were South Asian and 4% were Afro-Caribbean, with a mean age of 54±13 years. Seventeen per cent were current smokers. The biochemical and haematological characteristics of the cohort are shown in table 2. The mean eGFR was 50±15 ml/min/1.73 m2 with a mean phosphate of 1.11±0.21 mmol/l. The frequency of CKD stage was as follows: stage 2, 22%; stage 3a, 39%; stage 3b, 34%; stage 4, 6%. Fifty-nine per cent of patients had renal disease confirmed by biopsy, with a further 23% diagnosed using ultrasonography.
Renal diagnoses and medications of the study population
Demographic, haematological and biochemical characteristics of the entire cohort according to quartiles of increasing serum phosphate
Imaging, blood pressure and PWV parameters are shown in table 3. LVMI was higher in men than in women (62.5 vs 49.9 g/m2; p<0.0001). Five patients (2%) had LVH, of which three were male. The mean PWV was 8.6±2.1 m/s, with no differences between men and women.
Cardiac magnetic resonance parameters, blood pressure and PWV for the entire cohort according to quartiles of increasing serum phosphate (as in table 2)
Relationships with serum phosphate
Sixty-two (30%) patients had a serum phosphate level higher than the recommended treatment threshold of 1.2 mmol/l, as defined in the Kidney Disease: Improving Global Outcomes guidelines.14 Patients with serum phosphate >1.2 mmol/l had a greater LVMI than those with serum phosphate <1.2 mmol/l (61 vs 55 g/m2; p=0.03), with no differences in eGFR (52±16 vs 49±15 ml/min/1.73 m2; p=0.3), age (54±12 vs 54±13 years; p=0.8), or office blood pressure (systolic blood pressure 130±18 vs 129±17 mm Hg; p=0.6) and 24 h ambulatory blood pressure (daytime average systolic blood pressure 122±12 vs 121±11 mm Hg; p=0.4). This association was also present when gender-specific LVMI was assessed with serum phosphate (men: 70 vs 60 g/m2; p=0.001; women: 53 vs 48 g/m2; p=0.03), with no differences in eGFR, body mass index, age, PWV, or office and 24 h ambulatory blood pressures between phosphate groups.
When the cohort was divided into quartiles according to serum phosphate concentrations, LVMI increased across phosphate quartiles (p=0.04; table 3). There were no differences in age, office or 24 h ambulatory blood pressure, PWV, eGFR, calcium, parathyroid hormone (PTH), haemoglobin, albuminuria or cholesterol across the quartiles (table 2). The relationship between serum phosphate quartiles and LVMI persisted when analysed separately for men (p=0.002) and women (p=0.04; figure 1). There was no observed difference in absolute LVM across quartiles (p=0.1), but more women were in the higher serum phosphate quartiles than in the lower quartiles (table 2; p=0.03). When men and women were analysed separately, absolute LVM increased across phosphate quartiles (p=0.002 and p=0.04, respectively).

Left ventricular mass index (LVMI) in women (A) and men (B) according to serum phosphate quartile. One-way analysis of variance: women (p=0.04) and men (p=0.002).
Correlations with LVMI
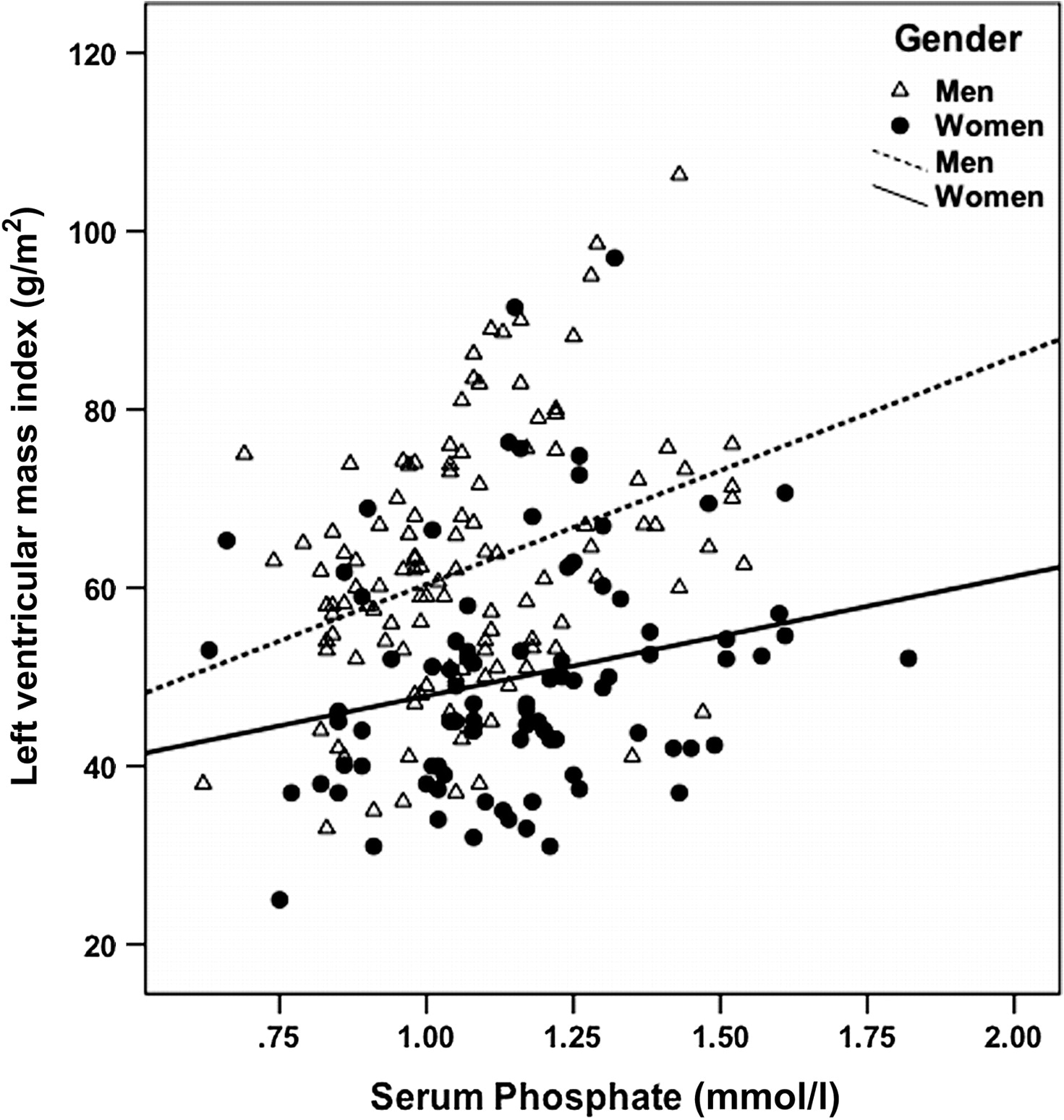
Log ACR (r=0.184; p=0.009), haemoglobin (r=0.162; p=0.02), serum phosphate (r=0.173; p=0.01; figure 2), office systolic blood pressure (r=0.323; p<0.0001), office diastolic blood pressure (r=0.260; p<0.0001) and pulse pressure (r=0.191; p=0.008) all correlated with LVMI. There was no correlation between PWV and LVMI (p=0.2). Age, eGFR, calcium, log PTH, total cholesterol and high-density lipoprotein cholesterol did not correlate with LVMI.

{kind=link}
{kind=link}
Scatter plot of left ventricular mass index (LVMI) versus serum phosphate labelled by gender. Pearson's correlation: whole cohort (r=0.17; p=0.01), women (r=0.23; p=0.03) and men (r=0.34; p<0.0001).
Determinants of LVM
All variables that significantly correlated with LVMI (including gender) were entered into an ‘enter’ linear regression model using LVMI as a continuous variable, with office systolic blood pressure used as the most highly correlated measure for blood pressure (table 4). Log ACR and haemoglobin were not significantly associated with LVMI in this model. The model explained 30% of the variation in LVMI (p<0.0005). The importance of serum phosphate and systolic blood pressure in explaining the variance in LVMI was confirmed, with serum phosphate accounting for 5% of the variance and with systolic blood pressure accounting for 6% of the variance. Substitution of central blood pressure for peripheral blood pressure in the model made no appreciable difference in the results. When analysis was repeated with absolute LVM as the outcome variable and with BMI as an additional covariate, the model remained significant, with 37% of the variation in absolute LVM being explained (p<0.0005). Serum phosphate, systolic blood pressure and gender were the only significant independent predictors of absolute LVM, with serum phosphate and systolic blood pressure accounting for 5% and 4% of the variance, respectively.
Enter linear regression: predictors of LVMI
Reproducibility
The overall reliability of the intraobserver measurements of LVMI was high, with an intraclass correlation coefficient of 0.992 (95% CI 0.981 to 0.997).
Discussion
In this study, we have shown that serum phosphate is associated with LVM in both men and women with early-stage CKD. The association is maintained after adjusting for multiple confounders and is independent of blood pressure, age and renal function. We were unable to demonstrate a relationship between serum phosphate and arterial stiffness. In this cohort of patients with well-controlled blood pressure, the variance in LVM explained by serum phosphate is of a very similar magnitude to that explained by systolic blood pressure. These findings raise the possibility that lowering serum phosphate might be a novel way of reducing LVM, thus providing an alternative means of improving cardiovascular outcome in this group of patients.
Although the higher cardiovascular risk conferred by the presence of LVH as a categorical variable is well accepted, it is increasingly recognised that there is no biological dichotomy; LVM is a continuous variable with a graded relationship with cardiovascular risk.6 7 The reasons for this association are unclear; LVM may merely reflect the cumulative burden of exposure to high blood pressure or may directly influence cardiovascular risk through factors such as increased myocardial oxygen consumption, reduced coronary flow reserve, and ventricular scarring and fibrosis, causing an increased risk of arrhythmia.6 In patients with CKD, increased LVM is just one manifestation of ‘uraemic cardiomyopathy’.2 In favour of a causative relationship is the finding that in patients with hypertension and LVH, a reduction in LVM during anti-hypertensive treatment is associated with improved cardiovascular outcome, in addition to the benefit gained from lower blood pressure.7 Furthermore, reduction of blood pressure within the normal range is associated with further reductions in LVM.12 15 However, there may be limits to how low blood pressure can be reduced without increasing cardiovascular events and mortality. Although chronic pressure overload is generally accepted as a major determinant of LVH, the contribution of other biological variables is now acknowledged.16
Two studies have demonstrated a similar association between serum phosphate and LVM in patients with ESKD.17 18 Strozecki et al17 used echocardiography to demonstrate a correlation between serum phosphate and LVM in 22 normotensive patients undergoing haemodialysis. These results were verified in a more recent study of 246 patients undergoing haemodialysis in which serum calcium phosphate product was a major determinant of LVM measured using CMR.18 Our study extends these findings to the early-stage CKD population, indicating that phosphate has an influence on cardiovascular structure in the early stages of CKD when the majority of patients have a serum phosphate level that lies below the treatment threshold recommended by the Kidney Disease: Improving Global Outcomes guidelines.14 Improved control of hyperphosphataemia through the use of a daily dialysis regimen has been shown to be independently associated with a reduction in LVM over 12 months compared to conventional haemodialysis in patients with ESKD.19 Whether similar reductions in serum phosphate are associated with decreased LVM in patients with predialysis CKD requires further investigation.
In an observational study of 978 patients with stable coronary artery disease and normal renal function, serum phosphate was associated with LVM in men but not in women.20 In our cohort, the strength of association between phosphate and LVM was weaker in women than in men. It is possible that hormonal factors may explain this difference in the strength of association, but this is an area that requires further study.
Phosphate may play a causative role in the development of LVH and myocardial fibrosis through a number of possible actions. The most widely accepted mechanism is by an increase in arterial stiffness and, therefore, left ventricular afterload. In vitro experiments have shown that high levels of intracellular phosphate actively promote the osteogenic transformation of vascular smooth muscle cells, resulting in vascular calcification.2 Deposition of calcium phosphate mineral in the vasculature is highly prevalent in patients undergoing dialysis, and the extent of calcification correlates with the severity of arterial stiffness and is a predictor of all-cause mortality and cardiovascular mortality in ESKD.21 An association between vascular calcification, arterial stiffness and LVM has been demonstrated in small numbers of patients with ESKD22 23; in larger studies of non-CKD populations, serum phosphate has been associated with surrogate measures of arterial stiffness.24 25 Our cohort of patients with early-stage CKD with a mean age of 54±13 years had excellent blood pressure control and only marginally elevated PWV (mean 8.6±2.1 m/s), which may account for the absence of any demonstrable relationship with serum phosphate or LVM. Our study thus provides no support for this hypothesis but—being observational in nature—does not exclude such a mechanism. Alternatively, animal studies suggest that phosphate might exert direct actions on the myocardium, inducing fibrosis and LVH, although the mechanism by which this occurs requires further study.3 4 Given concerns regarding the use of gadolinium-based contrast agents in patients with renal dysfunction, this was not studied in our population.
An alternative explanation for the relationship between serum phosphate and LVM is the existence of a common factor present in CKD that influences both of these variables. Hyperphosphataemia is associated with increased levels of the phosphaturic hormone fibroblast growth factor 23 (FGF-23), increased PTH and decreased vitamin D levels. FGF-23 regulates calcium phosphate metabolism and was associated with LVM independently of serum phosphate levels in a study of 220 patients with predialysis CKD.26 The authors did not demonstrate a relationship between serum phosphate and LVM in their cohort. Approximately half of their cohort was diabetic, however, and comprised a large proportion of Afro-Caribbean subjects. They also included patients with coronary artery disease and congestive heart failure. Furthermore, 15% of subjects with the lowest eGFR were receiving phosphate binders, and 25% were receiving activated vitamin D. All of these factors could have significantly affected the relationship between serum phosphate and LVM in their cohort. Levels of FGF-23 and serum phosphate are intricately linked,27 and activation of FGF-23 receptors has been shown to induce myocyte hypertrophy in vitro.28 It remains unclear whether FGF-23 directly promotes LVH or increases arterial stiffness in CKD. The effects of FGF-23 are mediated by the renal coreceptor Klotho, the expression of which is reduced in early-stage CKD. It has been suggested that Klotho is the initiator of renal mineral bone disorder and abnormal phosphate handling in CKD, although its relationships with arterial stiffness and LVM are currently unknown.29 PTH has been implicated in the development of cardiac fibrosis in animal models,30 and a small study of normotensive patients undergoing haemodialysis has demonstrated an association between PTH and echocardiographically derived LVM.17 A larger study of patients undergoing haemodialysis using CMR-derived LVM was unable to replicate this finding.18 We were also unable to demonstrate an association. Vitamin D receptor gene polymorphisms have been linked to LVH in patients with ESKD,31 and treatment with vitamin D analogues has been associated with reductions in LVM in animal models32 and with regression of LVH in patients undergoing haemodialysis.33 It remains unclear whether these observations are due to the direct cardiovascular effects of vitamin D or depend on whether other mediators are involved.
Phosphate plays a key role in multiple aspects of myocyte metabolism, including regulation of cardiac energetics.34 There is some evidence that reduced phosphate is associated with impaired myocardial performance.35 Abnormal cardiac energetics have been demonstrated in patients with increased LVM and may play a role in the progression of structural heart disease and in the development of heart failure.36 Impaired cardiac energetics have also been demonstrated in animal models of CKD.37 The relationship between cardiac energetics and a high phosphate state is unknown but represents an area worthy of future study.
There are limitations to our study. All subjects recruited into this study were under regular review by nephrologists, and most had primary renal disease, potentially limiting the applicability of our results to patients with CKD who are treated solely in the community. We did not collect data on serum vitamin D or FGF-23 concentrations, which would have provided greater insights into potential aetiological mechanisms. Unlike these tests, however, serum phosphate is an easily measured variable that is widely available and regularly used in routine clinical practice. We did not perform gadolinium-enhanced CMR, which may have provided useful insights into the effects of phosphate on myocardial fibrosis. Our study was observational and cross-sectional in design and thus subject to potential confounding from missing variables; therefore, we are able only to describe associations and not to infer causality. Nevertheless, this is the first study to report a clear association between serum phosphate and LVM, a prognostically important cardiovascular variable, in patients with early-stage CKD. Further longitudinal and interventional studies with hard end points are required to determine whether the association between phosphate and LVM is causative and whether phosphate lowering is effective at reducing LVM and, therefore, cardiovascular risk in this group of patients.
References
Footnotes
Funding This study was supported by a grant from the British Heart Foundation and by an unrestricted educational grant from Genzyme Corporation.
Competing interests CJF has received lecture and advisory board fees from Genzyme Corporation. All authors are recipients of an unrestricted educational grant from Genzyme Corporation.
Patient consent Obtained.
Ethics approval Ethics approval was provided by the West Midlands Research ethics committee.
Provenance and peer review Not commissioned; externally peer reviewed.