Article Text

Abstract
Objectives To identify the determinants and the impact on outcome of brain natriuretic peptide (BNP) in asymptomatic patients with degenerative mitral regurgitation (MR).
Method Comprehensive transthoracic echocardiography including two-dimensional speckle tracking quantification was performed in 135 consecutive asymptomatic patients (60±14 years, 56% men) with moderate to severe degenerative MR and preserved left ventricular (LV) function. Blood samples were collected at the time of the echocardiography and plasma BNP levels were measured.
Main outcome measures BNP level and cardiac events.
Results BNP was correlated with age, indexed LV end-systolic diameter, indexed left atrium (LA) volume, estimated LV filling pressure with E/Ea ratio, systolic pulmonary arterial pressure and global longitudinal strain (GLS). In multiple regression analysis, indexed LA volume (p=0.008), mitral deceleration time (p=0.003) and GLS (p<0.0001) were independently associated with BNP. During follow-up (mean=23±19 months), 54 events occurred resulting in 4-year event-free survival of 50±6%. There was a graded relationship between the increase in BNP (ie, according to quartile) and reduced event-free survival (p<0.0001). In Cox multivariable analysis, indexed LA volume (HR=1.04, p=0.003), GLS (HR=1.14, p=0.007) and 3rd and 4th quartiles of BNP (HR=8.5, p=0.002 and HR=8.8, p=0.002) were independent determinants of event-free survival.
Conclusion In asymptomatic degenerative MR, LV longitudinal function and LA volume are the main determinants of BNP release. BNP is a powerful independent predictor of cardiac events. Measurement of plasma BNP may help to improve risk stratification and management of asymptomatic patients with degenerative MR.
- Valve
- mitral regurgitation
- echocardiography
- brain natriuretic peptide
- speckle tracking
- aortic valve disease
- exercise echocardiography
- dobutamine echocardiography
- valvular heart disease
- valve disease
- EBM
- aortic stenosis
- prosthetic heart valves
- cardiomyopathy restrictive
- diastolic function
- congestive heart failure
- heart failure
- stress echocardiography
- echocardiography
Statistics from Altmetric.com
- Valve
- mitral regurgitation
- echocardiography
- brain natriuretic peptide
- speckle tracking
- aortic valve disease
- exercise echocardiography
- dobutamine echocardiography
- valvular heart disease
- valve disease
- EBM
- aortic stenosis
- prosthetic heart valves
- cardiomyopathy restrictive
- diastolic function
- congestive heart failure
- heart failure
- stress echocardiography
- echocardiography
Introduction
The management and timing of surgery of patients with asymptomatic degenerative mitral regurgitation (MR) remain controversial. In severe MR, both the current European Society of Cardiology (ESC)1 and American College of Cardiology/American Heart Association (ACC/AHA)2 guidelines recommend mitral valve surgery when symptoms, left ventricular (LV) dysfunction, atrial fibrillation or pulmonary arterial hypertension occur (class I and IIa). In the absence of such criteria, patients with chronic severe MR may undergo surgery only when the likelihood of successful repair is high (>90%). However, surgeons may be reluctant to operate on patients without symptoms, even in the absence of comorbidities. Indeed, although operative mortality of mitral valve repair may be very low in selected series and centres, it is still significant and these excellent operative results are not necessarily generalisable to all centres. Furthermore, despite the improvement in the awareness and technical skills of the surgeons for this procedure, a substantial proportion of the valves that are potentially repairable are ultimately replaced by a prosthesis. In this regard, some authors recommend referring patients for prophylactic mitral surgery only to high-volume and experienced surgical centres.3 4 Nevertheless, this strategy is not always feasible for various reasons including availability, local context, patient preference and insurance restrictions.5 Consequently, the selection of appropriate asymptomatic patients with severe MR (ie, in whom the benefit/risk ratio (RR) of early surgery may be expected to be optimal), is the cornerstone of the management of these patients.
Brain natriuretic peptide (BNP) and its inactive amino terminal portion are neurohormones released by the ventricles in response to increased LV wall stress. A recent study reported that assessment of BNP levels and quantification of MR may provide complementary prognostic information in acute coronary syndromes.6 In patients with organic MR, BNP is known to be related not to MR itself but rather to the consequences of MR, mainly on LV, left atrium (LA)7 and systolic pulmonary arterial pressure (SPAP).8 Accordingly, a few studies have suggested that BNP level measurement may be useful for risk stratification of asymptomatic severe MR.9 10
Recent echocardiographic advances have introduced the use of two-dimensional speckle-tracking (2DST) analysis to quantify longitudinal LV myocardial function and detect subtle and subclinical LV dysfunction. Because LV ejection fraction is well recognised as a poor echocardiographic parameter to assess LV systolic function in ≥ moderate organic MR,11 12 the evaluation of LV longitudinal function may help to detect early LV dysfunction. However, the relationship between LV longitudinal function and BNP is, to the best of our knowledge, unknown in this population.
The aim of this study was to identify the determinants and the impact on outcome of BNP in asymptomatic patients with degenerative MR.
Methods
Study population
A total of 135 consecutive asymptomatic patients with at least moderate degenerative MR (defined as an effective regurgitant orifice (ERO) area ≥20 mm2 and/or a regurgitant volume (RV) ≥30 ml) were prospectively included in two centres (University of Liège, CHU Sart Tilman, Liège, Belgium, n=106; Quebec Heart and Lung Institute, Quebec, Canada, n=29). Patients with one of the following criteria were excluded: (1) LV end-systolic diameter >45 mm; (2) LV ejection fraction <60%; (3) atrial fibrillation; and (4) concomitant >mild valvular stenosis or regurgitation.
The present protocol was approved by the relevant institutional review boards and all patients gave written informed consent.
Demographic and clinical data
Demographic and clinical data included age, gender, height, weight, history of smoking, documented diagnosis of hypertension (patients receiving antihypertensive medications or having untreated hypertension (blood pressure ≥140/90 mm Hg)), hypercholesterolaemia (patients on cholesterol-lowering medication or, in the absence of such medication, low-density lipoprotein cholesterol level >160 mg/dl) and diabetes (patients currently receiving oral hypoglycaemic medication or insulin).
Echocardiographic measurements
Echocardiographic examinations were performed with a Vivid 7 or 9 imaging device (GE Healthcare, Little Chalfont, UK). All echocardiographic and Doppler data were obtained in digital format and stored on a workstation for offline analysis (EchoPAC, GE Vingmed Ultrasound AS, Horten, Norway). All measurements were averaged over three cardiac cycles. MR was quantified as previously described13 and recommended.14 The RV and the ERO area were reported as the average of the proximal isovelocity surface area and of Doppler volumetric methods. The LV diameters were obtained from the parasternal long-axis view by two-dimensional guided M-mode using the leading edge methodology at end diastole and end systole. The LV end-systolic and end-diastolic volumes as well as the LV ejection fraction were obtained using the modified biplane Simpson's method. The LV stroke volume was calculated by multiplying the LV outflow tract area by the LV outflow tract velocity–time integral measured by pulsed-wave Doppler. The LA volume was obtained using the area-length method. Mitral E- and A-wave velocities were measured with pulsed-wave Doppler, and Ea-wave velocity by tissue Doppler imaging in the septal position of the mitral annulus. The LV filling pressure was estimated using the E/Ea ratio. SPAP was derived from the regurgitant jet of tricuspid regurgitation using systolic transtricuspid pressure gradient calculated by the modified Bernoulli equation and the addition of 10 mm Hg for right atrial pressure as previously performed15 and validated.13 16
In order to comprehensively assess LV myocardial function, the global longitudinal strain (GLS) was quantified using 2DST analysis. From standard bidimensional grayscale recordings (frame rate >60/s), the endocardial borders were traced at the end-systolic frame, and an automated tracking algorithm outlined the myocardium in successive frames throughout the cardiac cycle. The tracking quality was verified for each segment (with subsequent manual adjustment of the region of interest if necessary), and myocardial motion was analysed by speckle tracking within the region of interest bound by endocardial and epicardial borders. Inadequate tracked segments were automatically excluded from analysis. In this situation, local strain in each segment was calculated.17 18 GLS was obtained by averaging all segment strain values from the apical 4-, 3- and 2-chamber views.
The reproducibility of MR quantification and GLS have been previously reported.16 19
Plasma BNP level measurement
Venous blood samples for baseline BNP measurement were drawn before echocardiography, after 20 min of supine rest. Chilled ethylenediamine tetra-acetic acid tubes were centrifuged immediately at 4000 rpm (4°C) for 15 min. Separated plasma samples were processed by immunofluorescence assay (Biosite, Beckman Coulter, San Diego, California, USA). The inter- and intra-assay variations were 5% and 4%, respectively. The assay detection limit was 1 pg/ml.
Cardiac event-free survival
Patient follow-up was performed according to current guidelines. Follow-up information was obtained from interviews with the patients, physicians or eventually next of kin every 6–12 months. Cardiac event was defined as the occurrence of cardiovascular-related death, mitral valve surgery (indicated only by the development of symptoms or LV dysfunction, according to current guidelines) and hospitalisation for acute pulmonary oedema or congestive heart failure. Surgery performed on the basis of the presence of pulmonary hypertension was not considered as an event. At the end of this study, patients with a last follow-up of >6 months were re-evaluated by telephone calls from physicians or next of kin.
To ensure blinding and avoid bias in clinical decision-making, the results of BNP levels were not transmitted to the treating physician or surgeon.
Statistical analysis
The results are expressed as mean±SD or percentage unless otherwise specified. Patients were studied in two groups according to the median of BNP level. Differences between groups were analysed for statistical significance with the Student t test, Mann–Whitney U test, χ2 test or Fisher exact test as appropriate. Correlations between echocardiographic data and BNP level were assessed with linear regressions. Independent predictors of BNP level or BNP >median were obtained with the use of stepwise multiple linear regressions or logistic regression, respectively. Probabilities of cardiac event-free survival were obtained by Kaplan–Meier estimates and then compared with a two-sided log-rank test. Cox proportional hazards models were used both in individual and multivariable analyses to identify the independent predictors of cardiac event-free survival. The impact of BNP level on outcome was assessed according to quartile. Variables with a univariate value of p<0.10 were incorporated into the multivariable models. Gender was forced into the multivariate models regardless of the p value on univariate analysis because it has been show to influence plasma BNP levels.20
Values of p<0.05 were considered significant. All statistical analyses were performed with STATISTICA version 6 (StatSoft, Tulsa, Oklahoma, USA).
Results
Among the 135 included patients (60±14 years, 56% men), 82 (61%) had severe MR with RV >60 ml. The BNP varied widely (figure 1) from 5 pg/ml to 439 pg/ml (median 40 pg/ml, mean 61±70 pg/ml) resulting in a normality test failure (p<0.0001). After log transformation the BNP distribution was normal (p=0.35). According to the median BNP level (40 pg/ml), patients with high BNP were significantly older (p=0.02) and there was no other significant difference between the two groups regarding demographic and clinical data and risk factors, medication and mitral valve prolapse localisation (table 1).

Distribution of brain natriuretic peptide level in the whole cohort.
Demographic and clinical data
In severe MR, patients with high BNP also tended to be older (p=0.08).
Echocardiographic data in patients with high versus low BNP
There was no significant difference between low and high BNP level groups regarding LV dimensions and systolic function (table 2). Patients with a high BNP level had a significantly higher E/Ea ratio (p=0.049) and longer deceleration time (p=0.0045). The LA volume and LA volume indexed for body surface area were significantly higher in patients with a BNP level >40 pg/ml (both p=0.0001). Of note, there was no significant difference in ERO and RV between the two groups (p=0.58 and p=0.64, respectively). Patients with severe MR had a statistically similar BNP level to those with moderate MR (69±84 vs 56±58 pg/ml, p=0.28). The SPAP was significantly higher in the high BNP group (table 2, p=0.03) and patients with pulmonary hypertension (ie, SPAP >50 mm Hg) had a significantly higher BNP level (122±129 vs 53±54 pg/ml, p=0.0002). LV longitudinal myocardial function, as assessed using the GLS, was significantly impaired in patients with BNP level >40 pg/ml (−17.7±3 vs −22.3±3, p<0.0001). In addition, there was a direct relationship between increased BNP level and increased GLS (ie, impaired LV longitudinal function) (p<0.0001, figure 2).
Echocardiographic data

Relationship between brain natriuretic peptide (BNP) level and global longitudinal strain. (A) Global longitudinal strain in the whole cohort and according to the quartiles of BNP level (Q1: 0–19 pg/ml, Q2: 20–40 pg/ml, Q3: 41–70 pg/ml, Q4: 71–439 pg/ml; *p=0.051 vs Q1, †p<0.0001 vs Q1, ‡p<0.01 vs Q2, §p=0.06 vs Q3). (B) Correlation between the log transformation of BNP and global longitudinal strain.
In patients with severe MR a high BNP was associated with higher indexed LV end-systolic volume, indexed LA volume, SPAP and GLS (all p<0.03).
Determinants of BNP level
The log transformation of BNP was significantly correlated with age, indexed LVES diameter, E/Ea ratio, deceleration time, LA and indexed LA volume, and with SPAP (table 3). The best correlation with log BNP was found with the GLS (r=0.64, p<0.0001; figure 2B). In multiple linear regression, mitral deceleration time, indexed LA volume and GLS were independent determinants of log BNP (table 4).
Correlation with BNP
Multivariable analysis to identify the determinants of BNP
A multiple logistic regression model was then built (table 4) in order to identify the independent determinants of elevated BNP level (>40 pg/ml). In this model, long deceleration time and high indexed LA volume were independently associated with high BNP level. GLS was identified as the strongest determinant of BNP level >40 pg/ml (p=0.001), with a 33% increased risk of having elevated BNP for each increase of 1% (ie, impairment of LV longitudinal myocardial function) of GLS (OR=1.33, 95% of CI 1.12 to 1.59).
Impact of BNP on cardiac event-free survival
During follow-up (mean 23±19 months, median 17 months), 54 patients (40%) had a predefined cardiac event. Mitral valve surgery (70% of mitral valve repair) was motivated by the occurrence of symptoms in 18 patients, the presence of LV dysfunction or dilation in 5 patients or by the combination of both in 20 patients. Among the 11 remaining patients in whom a cardiac event other than surgery occurred, 10 were hospitalised due to syncope, congestive heart failure or acute pulmonary oedema and one died. Cardiac event-free survival was 77±4% and 59±5% at 1 and 2 years, respectively.
According to the median BNP level (40 pg/ml), patients with low BNP had significantly higher cardiac event-free survival (1 year: 92±3 vs 61±6%; 2 years: 81±5 vs 35±7%; p<0.0001). Using receiver operative characteristics curve analysis, a BNP level >40 pg/ml yielded the best results for predicting outcome (sensitivity 74%, specificity 65%, positive predictive value 59%, negative predictive value 79%). Compared with quartile 1 of BNP level, the 2-year event-free survival was significantly reduced in quartile 3 and 4 (Q1: 83±7% vs Q3: 35±11% and Q4: 35±10%, respectively, p<0.0001, figure 3).
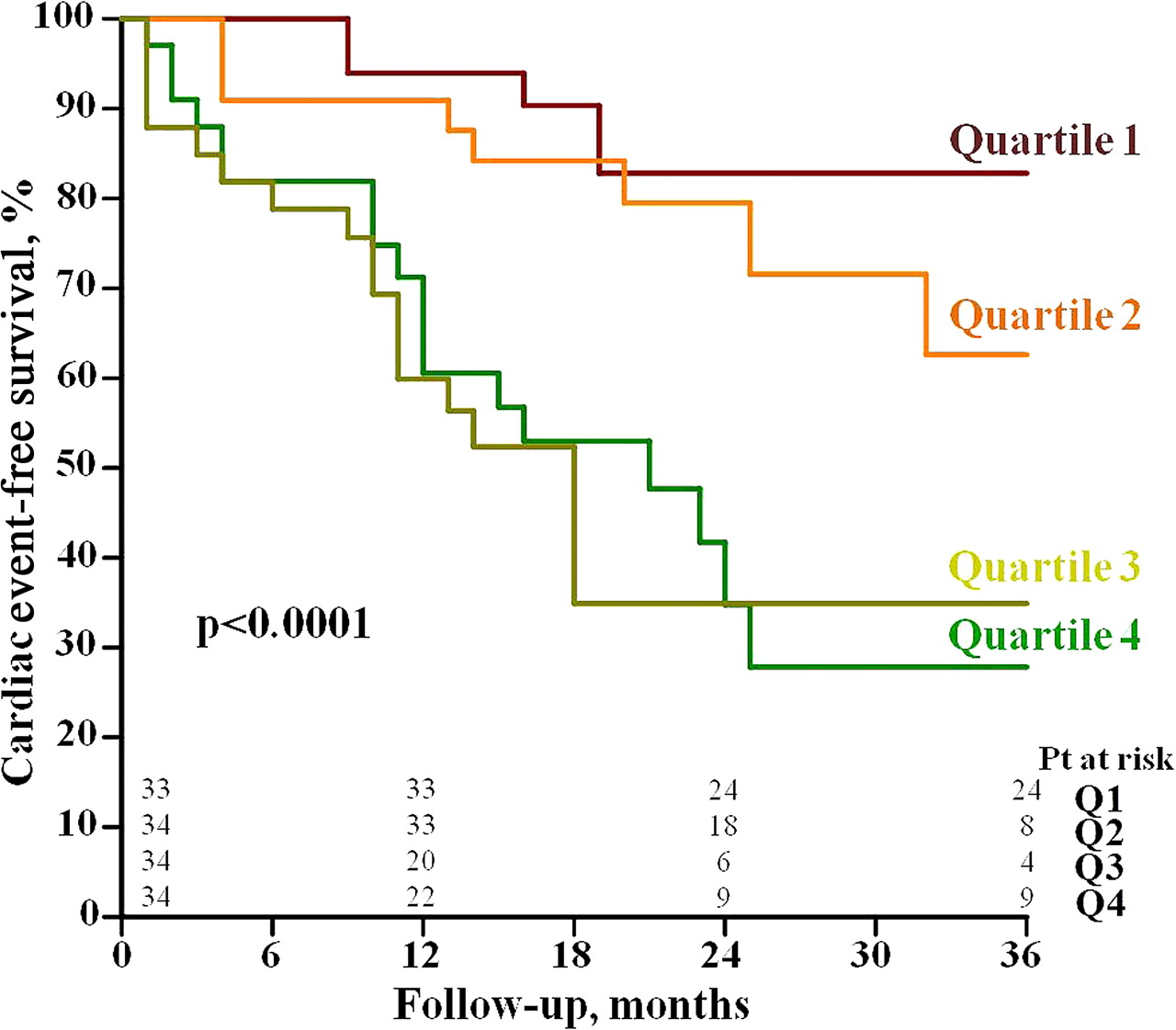
Cardiac event-free survival stratified according to the quartiles of brain natriuretic peptide level.
In patients with severe MR, the high BNP group had significantly lower cardiac event-free survival (1 year: 54±8% vs 87±5%; 2 years: 37±9% vs 78±7%, p<0.0001).
In the univariate Cox proportional hazard model (table 5) a high BNP level (>40 pg/ml) was associated with an increased risk of cardiac event (HR=5.01, 95% CI 2.7 to 9.4, p<0.0001). Compared with the lowest BNP level quartile (quartile 1: 5–19 pg/ml; quartile 2: 20–40 pg/ml; quartile 3: 41–70 pg/ml; quartile 4: 71–439 pg/ml), quartile 3 and quartile 4 were significantly associated with a higher risk of cardiac events (HR=8.9, 95% CI 2.9 to 26.3, p<0.0001 and HR=10.3, 95% CI 3.4 to 30.8, p<0.0001, respectively; figure 4A). There was a trend for a significantly higher risk in quartile 2 compared with quartile 1 (HR=3.05, 95% CI 0.95 to 9.8, p=0.06). In the Cox proportional hazard model, multivariable analysis showed that the BNP level was an independent predictor of cardiac event-free survival (table 5). Independently of age, sex, MR severity, LV dimension and function, LA volume and LV filling pressure estimation, patients with a high BNP level (>40 pg/ml) had a fourfold increase in the risk of having a cardiac event during follow-up. Similarly, quartiles 3 and 4 of BNP were independently associated with significantly worse cardiac event-free survival (figure 4B) compared with quartile 1. In this multivariable model there was also a trend for quartile 2 to be at higher risk than quartile 1 (HR=3.5, 95% CI 0.9 to 14.1, p=0.075).
Cox proportional hazards analysis for the prediction of cardiac event-free survival according to median brain natriuretic peptide (BNP) level

Cox proportional hazard model for the prediction of cardiac event-free survival according to brain natriuretic peptide quartiles (quartile 1 as referent) in (A) univariable and (B) multivariable analysis. The multivariate adjustment was performed as in table 5 (model 2).
Other predictors of cardiac-event free survival
Indexed LA volume >40 ml/m2 was associated with significantly reduced cardiac event-free survival (2 years: 57±7% vs 66±7%, p=0.037, figure 5A). Patients with GLS <−20% (ie, median value) had significantly better 2-year event-free survival (73±6% vs 44±7%, p=0.0004, figure 5B). In the multivariate analysis reported in table 5 (Model 2), indexed LA volume (HR=1.04, 95% CI 1.01 to 1.07, p=0.003) and GLS (HR=1.14, 95% CI 1.04 to 1.26, p=0.007) were the other factors besides BNP level identified as independent predictors of cardiac event-free survival.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Cardiac event-free survival stratified according to (A) indexed left atrial (iLA) volume >40 ml/m2 and (B) median (−20%) global longitudinal strain (GLS).
Discussion
The results of the present study show that BNP level may vary considerably in asymptomatic patients with moderate to severe degenerative MR and preserved LV function. The main independent predictors of BNP level are mitral deceleration time, LA volume and LV longitudinal myocardial deformation. A high BNP level is independently associated with reduced cardiac-related event-free survival. Furthermore, LA volume and LV longitudinal myocardial deformation are also independent predictors of cardiac events.
Determinants of BNP
In a previous study including a wide range of MR severity, symptomatic status and LV function, Detaint et al7 underlined the relationship between BNP activation and LV volume overload. The presence of MR leads to LV and LA enlargement in response to volume overload and, consequently, to BNP activation and release independently of MR severity. Moreover, LA dilation contributes to the development of atrial fibrillation which is associated with an increased level of BNP.
Our results extend those of previous studies7 10 and indicate that LV end-systolic and LA dimensions are associated with elevated BNP levels. However, after further multivariate adjustment, only indexed LA volume remains independently associated with BNP. In addition, we identified LV longitudinal myocardial deformation (ie, a marker of subclinical myocardial dysfunction) as the main determinant of BNP. In degenerative MR, favourable loading conditions may mask a subtle degree of LV dysfunction.21 Subclinical LV dysfunction relates to the structure-function relationship and characterises a preclinical stage of myocardial damage that can be detected by a decrease in longitudinal myocardial function. The alteration of LV longitudinal kinetics is related to the vulnerability of subendocardial fibres and occurs before the development of dilation or abnormality observed with conventional measures of LV such as LV end-systolic diameter and ejection fraction.19 22 We found that, in the absence of LV dilation or reduced LV ejection fraction, GLS may be significantly reduced in asymptomatic degenerative MR and is well correlated with BNP level. In fact, GLS may be considered as a highly sensitive marker of both LV volume overload and LV wall stress which are, in turn, associated with BNP release.
Interestingly, we also found that a longer deceleration time is independently associated with BNP level. This suggests that prolonged LV relaxation indicates subclinical LV diastolic dysfunction, subtly increasing LV wall stress and thus participating in BNP activation. The results of our study show that, even in the absence of symptoms and reduced LV ejection fraction, patients with moderate to severe MR may have both subclinical LV systolic and diastolic impairment that is expressed by a rise in BNP level.
BNP release was reported as age- and gender-related in the general population20 and in patients with primary MR.7 The mechanisms whereby age influences BNP are unclear. Previous studies have reported that levels of natriuretic peptides are higher in elderly subjects, but these studies included patients with altered cardiac structure or function, not allowing differentiation of the impact of age and its consequences on the ventricle.23 24 Nevertheless, these investigators suggested that age-related changes in diastolic dysfunction or in renal function influence BNP. On the other hand, Redfield et al20 found that the relationship between age, gender and BNP was independent of clinical factors, renal function and cardiac structure parameters.
In our cohort the identification of the independent determinants of BNP in multivariable analysis (table 4) was performed with an age and gender adjustment. Whereas age was univariately associated with BNP level (r=0.32, p<0.0001, table 3), there was no significant difference between men and women with regard to BNP levels (p=0.13). Furthermore, neither age nor gender was an independent predictor of BNP in multivariable analysis.
BNP as a predictor of outcome
Several previous studies have found that BNP level is associated with outcome in patients with primary MR.7 9 10 Detaint et al7 showed that a median BNP level of ≥31 pg/ml was associated with reduced survival in a population including approximately one-third of patients with symptoms. Recently, Klaar et al10 reported that a BNP level of 44 pg/ml provides an almost 100% (99.5%) negative predictive value in predicting the occurrence of symptoms or LV dysfunction during follow-up. Pizarro et al9 validated a cut-off value of 105 pg/ml, corresponding approximately to the fourth quartile of BNP in their asymptomatic population, as a strong independent predictor of cardiac events in asymptomatic patients. However, the studied population included a significant proportion of patients with LV dilation.
In the present study we found that, in asymptomatic patients with moderate or severe degenerative MR, normal LV ejection fraction (>60%) and no LV dilation or atrial fibrillation, BNP level measurement represents a strong independent predictor of cardiac-related events. A BNP level >40 pg/ml was associated with an independent fourfold increase in the risk of cardiac event at 3 years. This association between BNP level and outcome is most likely the consequence of the close relationship between BNP activation and early and subclinical LV dysfunction and LA enlargement. Indeed, LA dilation is now well established as a good marker of poor outcome in patients with primary MR.25 26
Interestingly, we also found that reduced LV longitudinal myocardial function is an important predictor of cardiac events. The increased risk associated with BNP was unaffected by adjustment for other clinical and echocardiographic parameters, which included LV dimensions (as is generally done in previous studies7 9) and also LA size and GLS. This finding suggests that BNP activation is probably a surrogate for the consequences or degree of MR and is also additional to other descriptors of MR severity and predictors of outcome, which lends support to the clinical usefulness of this biomarker.
LV longitudinal function as a predictor of outcome
To the best of our knowledge, this study is the first to report that LV longitudinal function, as assessed by 2DST imaging, is an independent predictor of poor outcome in asymptomatic degenerative MR without LV dysfunction or dilation. Each 1% decrease in GLS (ie, impaired LV longitudinal function) is associated with a 14% increase in the risk of a cardiac event. Both GLS and BNP are therefore of high clinical value to enhance risk stratification and management in patients with asymptomatic MR. By improving the individual risk stratification and identifying LV dysfunction at an earlier stage, these parameters could be helpful for tailor-made therapeutic decision-making. Of note, LV longitudinal function has previously been identified as an accurate marker of postoperative LV dysfunction19 and recovery of functional capacity.27 Given that LV ejection fraction is known to remain normal or supranormal for long in the presence of moderate to severe MR11 12 and that LV dilation often occurs after the onset of symptoms,28 GLS—which is a rapid, simple and reproducible echocardiographic measure—should be integrated in the routine evaluation of patients with MR.
Clinical implications
The management of asymptomatic severe degenerative MR remains controversial.3 5 A ‘watchful-waiting’ strategy was previously reported as safe,28 with good perioperative and postoperative outcome. On the other hand, several authors have suggested that early intervention (ie, before the occurrence of a guidelines-recommended trigger for surgery), by increasing the rate of repairability, decreasing the operative mortality or complications and improving the postoperative LV function and outcome, should be recommended in the presence of severe MR.29–35 Nevertheless, early surgery is not without risk, and some surgeons may be reluctant to operate on asymptomatic patients only on the basis of the echocardiography-quantified severe MR. Consequently, risk stratification of these patients should be improved in order to optimise the benefit/RR of surgery. Recent studies from our group emphasised the usefulness of exercise stress echocardiography16 and the measurement of exercise pulmonary arterial hypertension13 to identify a subset of patients at high risk of more frequently and more rapidly developing symptoms. Unfortunately, stress echocardiography is not always available and feasible, underlining the profound need for new markers of risk. In this regard, BNP level is a low cost, simple, easily and rapidly measurable biomarker that may provide important incremental prognostic value and take a central role in the clinical armamentarium offered for the management of asymptomatic MR.
A high BNP level was associated with a more than eightfold increase in the risk of cardiac events compared with a very low BNP level (<19 pg/ml), suggesting that early intervention could be beneficial in such patients. In contrast, patients with a low BNP level had a reasonable 3-year cardiac event-free survival rate of 75±6%. These patients could therefore be closely followed up or, when possible, referred for exercise echocardiography in order to investigate LV contractile reserve19 36 and exercise-induced changes in MR16 and SPAP.13
Interestingly, in patients with moderate MR a high BNP level (greater than median) was also significantly associated with reduced cardiac event-free survival. As current guidelines do not recommend surgery in patients with moderate MR, our data therefore favour a closer clinical and echocardiographic follow-up of this subgroup of patients in order to identify promptly changes in clinical status, LV dimensions or function, pulmonary pressure and heart rhythm.
Limitations of the study
Our population consisted of relatively young patients with pure degenerative MR (ie, due to mitral valve prolapse or flail leaflet). The findings cannot therefore be extrapolated to all patients with MR. In particular, BNP level measurement should be used cautiously in patients with concomitant aortic stenosis or myocardial disease, atrial fibrillation, hypertension, renal failure or other known causes of increased neurohormones. In addition, the relatively young age of our patients may have influenced the outcome analyses.
The BNP measurement was performed only at baseline inclusion. Serial measurements of BNP and analysis of the progression of consequences of MR could be of interest. Further studies in larger cohorts are needed to address this point.
A substantial proportion of the cardiac events reported were mitral valve operations which are in part driven by the occurrence of symptoms for which the evaluation remains subjective. However, the symptomatic status is a class I indication for surgery in both the ACC/AHA and ESC guidelines.
Conclusion
In asymptomatic patients with degenerative MR, normal LV ejection fraction and no LV dilation, the BNP level may vary considerably among subjects. The main determinants of BNP in this population are the consequences of MR on LA size and on LV longitudinal myocardial function. The BNP level is a powerful independent predictor of reduced cardiac event-free survival. Measurement of the BNP plasma level may thus be useful to enhance risk stratification and better define the optimal timing of surgery in asymptomatic patients with degenerative MR.
Acknowledgments
We thank M Carmine Celentano for excellent technical assistance.
References
Footnotes
Funding JM is research associate from the FRS-FNRS, Brussels, Belgium and received grants from the Fonds Léon Fredericq, Liège, Belgium and from the Fond pour la Chirurgie Cardiaque, Belgium. This study was also supported by a grant (MOP #102 737) from the Canadian Institutes of Health Research, Ottawa, Ontario, Canada. PP holds the Canada Research Chair in Valvular Heart Diseases, Canadian Institutes of Health Research, Ottawa, Ontario, Canada.
Competing interests None.
Patient consent Obtained.
Ethics approval Committee/Institutional Review Board of CHU Sart Tilman, Belgium and of Laval Hospital, Quebec, QC, Canada.
Provenance and peer review Not commissioned; externally peer reviewed.