Article Text

Abstract
Objective To assess the relationship between elevated levels of B-type natriuretic peptide (BNP) and outcome in patients with Eisenmenger syndrome.
Design Retrospective study.
Setting Tertiary centre for adult congenital heart disease.
Patients All patients with Eisenmenger syndrome (n=181, age 36.9±12.1 years, 31% with Down syndrome) in whom BNP concentrations were measured as part of routine clinical care were included.
Main outcome measures The study end point was all cause mortality.
Results During a median follow-up period of 3.3 years, 20 patients (7 with Down syndrome) died. Higher BNP concentrations were predictive of all cause mortality on univariate analysis in patients with or without Down syndrome. On multivariable Cox proportional hazard analysis, BNP predicted survival independently of renal function, Down syndrome, or 6 min walk test distance (p=0.004). Temporal increases in BNP concentration were also found to predict mortality. Treatment with disease targeting therapies was associated with a significant reduction in BNP concentrations.
Conclusions BNP concentrations predict outcome in contemporary Eisenmenger patients. Increases in BNP concentrations over time are also of prognostic significance. In addition, disease targeting therapies may help to reduce BNP concentrations in this population, while treatment-naïve patients have static or rising BNP concentrations.
- Brain natriuretic peptide
- pulmonary arterial hypertension
- Eisenmenger syndrome
- prognosis
- mortality
- congenital heart disease
- exercise tolerance
- adult congenital heart disease
- exercise physiology
- exercise testing
- heart failure
- echocardiography
- heart rate variability
- pulmonary vascular disease
- pulmonary hypertension
- paediatric cardiology
- endocrinology
- metabolic medicine
- cardiac function
- paediatric echocardiology
- interventional catheteris
- paediatric cardiology
- paediatric interventional cardiology
- congenital - adult
- congenital - paediatric
Statistics from Altmetric.com
- Brain natriuretic peptide
- pulmonary arterial hypertension
- Eisenmenger syndrome
- prognosis
- mortality
- congenital heart disease
- exercise tolerance
- adult congenital heart disease
- exercise physiology
- exercise testing
- heart failure
- echocardiography
- heart rate variability
- pulmonary vascular disease
- pulmonary hypertension
- paediatric cardiology
- endocrinology
- metabolic medicine
- cardiac function
- paediatric echocardiology
- interventional catheteris
- paediatric cardiology
- paediatric interventional cardiology
- congenital - adult
- congenital - paediatric
Introduction
Adults with congenital heart disease (ACHD) represent an expanding patient population requiring life long tertiary medical care. Approximately 5–10% of patients develop pulmonary arterial hypertension (PAH) of variable severity.1 Eisenmenger syndrome—that is, pulmonary hypertension with reversed central shunt and cyanosis—represents the extreme manifestation of PAH in the setting of ACHD. Nowadays Eisenmenger syndrome can be prevented in the majority of paediatric patients. Nevertheless, approximately 4% of contemporary ACHD patients under follow-up at tertiary centres in Europe and North America have Eisenmenger syndrome.2 Morbidity and mortality remains considerable in this population.3 With the availability of oral disease targeting therapies, such as endothelin receptor antagonists and phosphodiesterase inhibitors, improving symptoms and survival,4–6 risk stratification is increasingly required in this patient group. B-type natriuretic peptide (BNP) is released by cardiomyocytes in response to ventricular stretch of the right and the left ventricle,7 and is an established marker of ventricular dysfunction.8–11 In adult patients with idiopathic PAH, BNP correlates with haemodynamic parameters8 and has been shown to be predictive of survival.12 In contrast, no data on the prognostic value of BNP is available in adults with Eisenmenger syndrome. This study aimed to establish the utility of BNP in predicting prognosis in patients with Eisenmenger syndrome and its response to treatment in this population.
Patients and methods
This was a retrospective study. All patients with Eisenmenger syndrome (Eisenmenger patients) attending the Royal Brompton Pulmonary Hypertension Service in whom plasma BNP concentrations were measured as part of routine clinical assessment between 2003 and 2010 were identified from biochemistry laboratory records. Their medical records were reviewed and demographic and clinical data were recorded. Six minute walk testing (6MWT) data were available in 99 patients within 6 months from BNP measurement, and WHO functional class was ascertained in all patients at the time of BNP analysis. The study end point was all-cause mortality. Survival status was assessed through the National Health Service computer system, which is linked to a national database of patient survival held by the UK's Office for National Statistics. Approval by the local research ethics committee was obtained.
Venous blood samples were collected into tubes containing potassium EDTA. The BNP concentrations were quantified using the commercial Beckman Access 2, Triage BNP assay (Biosite Diagnostics Inc, San Diego, California, USA). The upper limit of the reference range for this assay is <4 pmol/l (≈13.9 pg/ml). To convert these measurements to BNP measured in pg/ml, the value in pmol/l should be multiplied by 3.472.13
Statistical analysis
Values are presented as mean±SD or median and interquartile range (IQR, 25th and 75th centile) depending on variable distribution. Possible correlations between demographic, clinical or exercise variables and outcome were investigated using uni- and multivariable Cox proportional hazard analysis and hazard ratios (HRs) with two-sided 95% CIs are provided. Kaplan–Meier curves were generated to illustrate outcome based on quartiles of BNP concentrations. The results of the Cox regression were further validated by the use of a non-parametric random survival forest analysis (RSF) based on a log rank splitting rule.14 This ensemble tree method for the analysis of right censored survival data is based on a two step randomisation process. First, each tree is grown on a bootstrap sample of the data. Then, a random subset of variables is selected at each tree node and used to to split the tree using these candidate variables.15 Variable importance is assessed by calculating the change in prediction error, after the addition of artificial noise. Larger, positive values of variable importance indicate that a variable has a higher predictive value, while small or negative values are associated with less informative variables. In addition, importance of a predictor was assessed based on the minimal depth of a maximal subtree as described in detail previously.15 16 The smaller the minimal distance (the closer the maximal subtree is to the tree root), the greater the parameter's impact on prediction. The resulting RSF was also used to estimate predicted mortality for different BNP concentrations. Receiver operating curve (ROC) analyses were performed to assess the prognostic value of BNP concentration. Furthermore, multivariable ROC analysis/c-statistic was calculated for parameters significantly predicting survival on Cox analysis using a logistic regression model. In addition, time dependent ROC curves from censored survival data using the Kaplan–Meier method of Heagerty et al17 were employed to investigate further the prognostic value of BNP at 1, 2, and 3 years into follow-up. Statistical analysis was performed with R version 2.12.1.18 For all analyses a two-tailed probability value <0.05 was used as the criterion for statistical significance.
Results
Baseline characteristics
Overall, 181 Eisenmenger patients in whom BNP measurements were performed were included. The mean age was 36.9±12.1 years, 65 patients were male, and 56 patients had Down syndrome. Additional demographic information is presented in table 1. Based on the upper limit of normal of 4 pmol/l (≈13.9 pg/ml) for this assay, 153 patients (84%) had abnormal BNP concentrations. The distribution of BNP concentrations in Eisenmenger patients with and without Down syndrome is illustrated in figure 1. BNP concentrations increased with patient age (r=0.48, p=0.0001). Although patients in higher WHO functional classes tended to have higher BNP concentrations, this did not reach statistical significance (r=0.12, p=0.16). Similarly, there was no direct association between 6MWT distance and BNP concentrations (r=−0.06, p=0.61). Not unexpectedly, 6MWT distance and WHO functional class were found to be moderately correlated (r=−0.28, p=0.02). No significant difference in baseline BNP was found between patients with simple and complex underlying cardiac diagnosis (23.4±20.3 vs 27.2±44.5 pmol/l, p=0.53).
Patients baseline characteristics
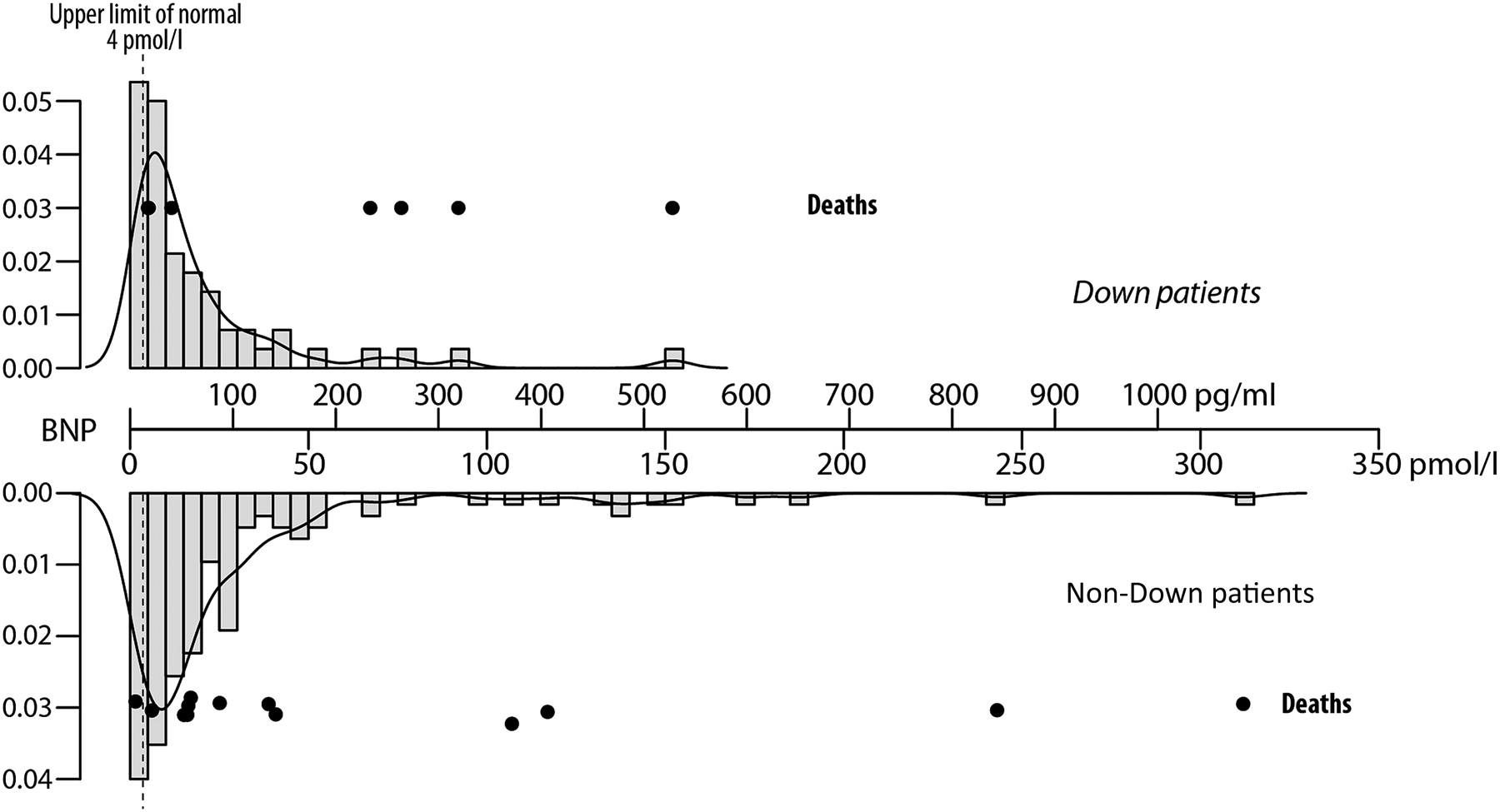
Histogram illustrating the distribution of B-type natriuretic peptide (BNP) concentrations in Eisenmenger patients with and without Down syndrome. BNP concentrations are presented in pg/ml and pmol/l. The black dots represent patients who died during follow-up.
Outcome
Over a median follow-up period of 3.3 years (IQR 2.2–4.4 years), 20 patients died (seven with Down syndrome) and 97 patients required hospital admission. Causes of death were as follows: progressive heart failure (n=8), sudden out-of-hospital collapse/circulatory arrest without evidence of haemoptysis (n=8), perioperative death following heart and lung transplantation (n=1), uncontrollable haemoptysis (n=1), and malignancy (n=1). For one patient the cause of death could not be established.
Predictive value of baseline BNP concentrations
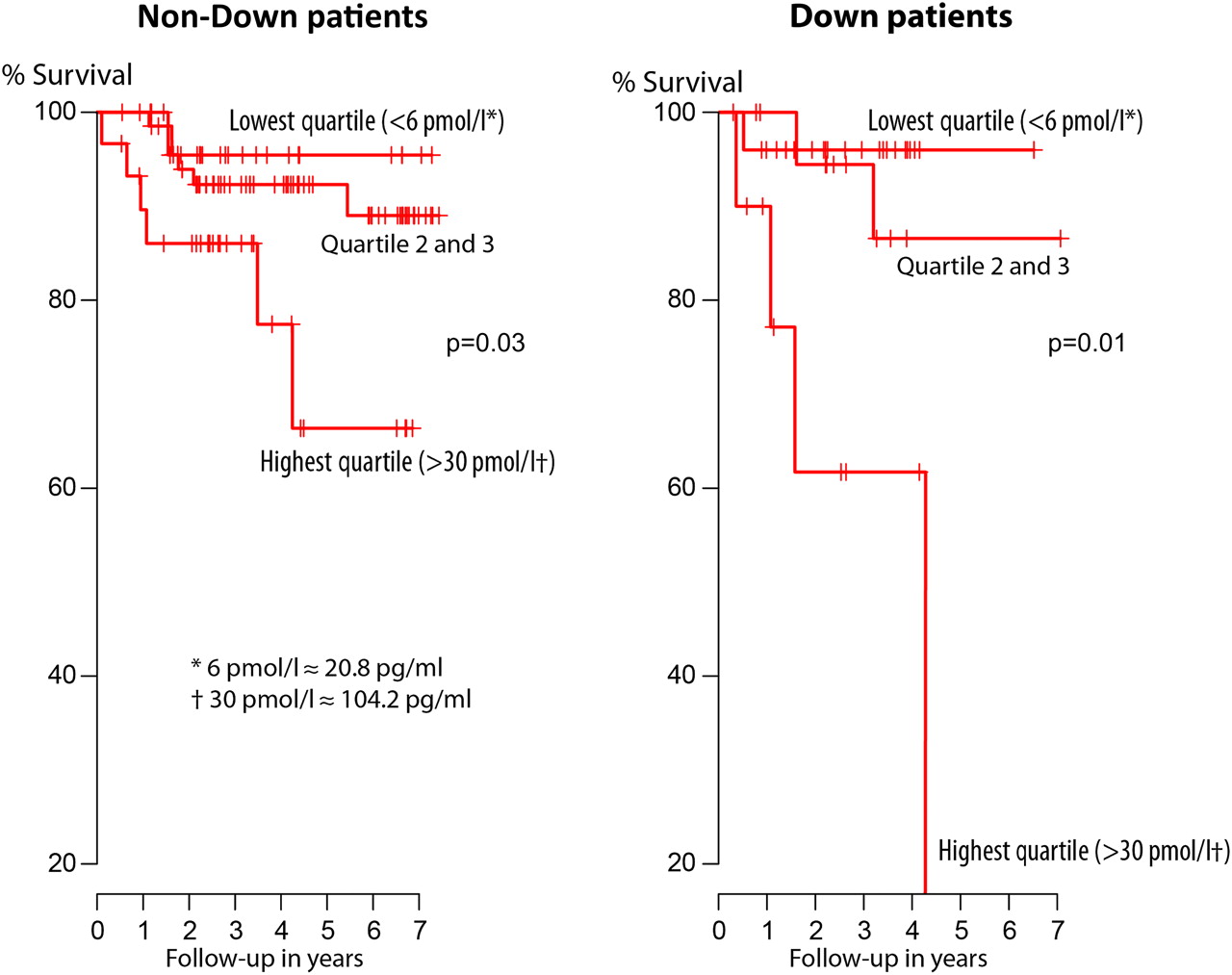
Baseline BNP concentrations were significantly related to all cause mortality on univariate Cox proportional hazard analysis, as shown in table 2. Other significant univariate predictors of survival included 6MWT distance, creatinine values, and resting oxygen saturations (table 2). Kaplan–Meier survival curves were constructed to illustrate the association between BNP values and all cause mortality based on the quartiles of the studied population (figure 2). We chose to construct Kaplan–Meier curves illustrating the association between BNP and survival based on the quartiles of the studied population (lowest quartile <6.0 pmol/l (≈17.4 pg/ml), middle quartiles 6–30 pmol/l, and highest quartile >30 pmol/l (≈104.2 pg/ml)). This showed that the risk of death rises with increasing plasma concentrations of BNP, both in the non-Down and Down syndrome population, and revealed an especially poor prognosis in patients with BNP concentrations >30 pmol/l (≈104.2 pg/ml). Values above this cut-off were associated with a 4.6-fold (95% CI 1.9 to 11.1) increase in the risk of death overall, and 7.8-fold increase (95% CI 1.7 to 36.6) in the Down syndrome population.
Significant univariable predictors of mortality on Cox proportional hazard analysis

Kaplan–Meier plots according to quartiles of B-type natriuretic peptide (BNP) for patients with and without Down syndrome. p Values refer to Log rank statistics. This figure is produced in colour in the online journal; please visit the website to view the colour figure.
On multivariable survival analysis BNP was confirmed as a significant predictor of survival in our study (table 3). As illustrated in figure 3A, BNP was shown to be the most informative predictor, based both on variable importance and assessment of lowest minimal distance of maximal subtrees on RSF analysis. In addition, the results of the RSF were used to illustrate predicted survival for various baseline BNP concentrations (figure 3B). Predicted survival is estimated over the follow-up period of the study (median 3.3 years).
Multivariable predictors of mortality on Cox proportional hazards analysis

(A) Results of the random survival forest analysis, illustrating parameter impact on prediction based on variable importance and minimal depth of a maximal subtree, confirming the results of the multivariable Cox proportional hazard analysis. (B) Results of the random survival forest analysis. Expected mortality over the study period (median 3.3 years) for various concentrations of B-type natriuretic peptide (BNP) based on the results of the random survival forrest analysis. The grey (red online only) and dotted lines represent cubic splines with 95% CIs. This figure is produced in colour in the online journal; please visit the website to view the colour figure.
ROC characteristics analyses
ROC characteristics analyses confirmed the predictive value of BNP, both in Down and non-Down syndrome patients (area under curve (AUC) 0.73 and 0.67, respectively). Based on the significant parameters on univariate Cox analysis, a multivariate c-statistic/ROC area analysis was performed to assess the incremental value of BNP in predicting all cause mortality in addition to 6MWT, creatinine, and presence of Down syndrome (=baseline model). The c-statistic increased from 0.81 for the baseline model to 0.86 with the addition of BNP for the entire follow-up period. Time dependent ROC analyses were also performed to assess the relative prognostic value of BNP at 1, 2, and 3 years of follow-up and to investigate the best timing for BNP measurements. These analyses showed the highest prognostic value of BNP at 1 year of follow-up (AUC 0.81 vs 0.68 and 0.65 at 2 and 3 years of follow-up, respectively).
Prognostic value of repeated BNP measurements
Overall, 73 patients had repeated BNP measurements within 1 year of the first BNP assessment. There were no significant differences between the patients with repeated BNP measurements and the remainder of the cohort in terms of age, gender distribution, complexity of lesions, prevalence of Down syndrome, functional class or resting oxygen saturation, reflecting cyanosis (p>0.05 for all). Concentrations of BNP increased in 45 patients, decreased in 26, and remained unchanged in two patients. Change in BNP concentrations were found to be significantly related to the risk of death on Cox proportional hazard analysis (HR 1.18 per 100 pg/ml BNP, 95% CI 1.07 to 1.30; p=0.0007). Moreover, the relative increase in BNP concentration was also found to be related to survival (HR 1.023 per 10% change, 95% CI 1.002 to 1.045; p=0.028). Interestingly, all four patients with an increase in BNP concentration above approximately 350 pg/ml (≈100 pmol/l) died during follow-up.
Effect of disease targeting therapies on BNP values
To investigate the effect of disease targeting therapies on BNP concentrations, patients were stratified into those who were commenced on disease targeting therapies during follow-up (n=46, 23 on bosentan, one on ambrisentan, and 22 on sildenafil) and those who remained treatment-naïve. Many patients with near normal BNP concentrations at baseline exhibited only minimal changes in BNP concentrations during follow-up. In patients with a baseline BNP concentration above 104.2 pg/ml (≈30 pmol/l; corresponding to the highest quartile of BNP), a significant reduction in BNP concentrations was seen during the first year of treatment (300±140 vs 184±102 pg/ml, p=0.03) with disease targeting therapies, supporting the notion that disease targeting therapies are associated with reductions in plasma BNP concentrations.
In contrast, as illustrated in figure 4, the four treatment-naïve patients with the most pronounced 1 year increase in BNP concentrations died during follow-up.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Change in B-type natriuretic peptide (BNP) concentrations within 1 year of start of disease targeting therapies or 1 year from the first available measurement in treatment-naïve patients. The figure shows that dramatic increases in BNP concentrations occurred in the treatment-naïve group only. Grey (red online only) dots/lines represent patients who died during follow-up. Black crosses indicate mean values. This figure is produced in colour in the online journal; please visit the website to view the colour figure.
Discussion
Employing a large contemporary cohort of Eisenmenger patients under follow-up at a tertiary centre for congenital heart disease and pulmonary hypertension, the current study demonstrates that plasma BNP concentrations are elevated in patients with Eisenmenger syndrome and relate to higher risk of death. Increases in BNP concentrations over time were also found to be of prognostic significance. In addition, this study provides evidence that disease targeting therapies may help to reduce BNP concentrations in this population, while treatment-naïve patients have static or rising BNP concentrations.
Despite being a multisystem disorder, Somerville et al reported that right ventricular failure and sudden cardiac death are the leading causes of mortality in Eisenmenger patients.19 BNP is released from myocytes in response to ventricular wall stress and myocardial ischaemia.20 In patients with acquired heart disease it represents a strong predictor of future cardiovascular events and death independent of ventricular dimensions and systolic dysfunction.21 This makes it especially attractive in the setting of complex congenital heart disease and Eisenmenger syndrome where objective echocardiographic quantification of biventricular function is inherently difficult due to complex anatomy, ventriculo-ventricular interaction, and dependence on loading conditions.22 23
The results of the current study suggest that Eisenmenger patients with elevated BNP concentrations have a high risk of death and, thus, require special medical attention. This is true for patients with and without Down syndrome, with high BNP concentrations being potentially even more concerning in the latter. Therefore, BNP concentrations should be periodically assessed in Eisenmenger patients. Time dependent ROC analysis showed that BNP concentrations bear prognostic information up to at least 3 years of assessment. However, the prognostic value was found to be strongest within 1 year of measurement, suggesting that at least annual assessment may be desirable. In addition, temporal increases in BNP concentrations were also found to relate to poor outcome in the current study. The fact that BNP concentrations were not found to be directly correlated with 6MWT distance or functional class suggests that exercise capacity in Eisenmenger patients is largely determined by extracardiac factors, such as oxygen carrying capacity of blood and the degree of desaturation during exercise, rather than directly by cardiac function. Interestingly, no direct association was found between complexity of underlying cardiac defect and BNP levels in the current study.
Our results raise the question of whether BNP concentrations could be used to guide therapy in Eisenmenger patients, in a similar fashion to the way BNP guided therapy has been advocated in heart failure. In the setting of heart failure it has been demonstrated that BNP guided therapy reduces mortality compared to conventional clinical care.24 Similarly, Squire et al demonstrated that plasma N-terminal pro-BNP (NT-proBNP) has the potential to guide therapy with ACE inhibitors in patients with acute coronary syndrome.25 Recently, goal orientated approaches have received cosiderable interest in patients with idiopathic PAH, and therapeutic strategies based on goal oriented algorithms have been associated with improved survival.26 27 Because choosing appropriate treatment goals requires identification of parameters that are strongly related to outcome,28 the results of this study suggest that BNP could represent such a parameter in Eisenmenger patients. Eisenmenger patients with a BNP value of approximately 100 pg/ml (≈30 pmol/l) had a particularly poor prognosis in the current study; therefore, this would represent an obvious cut-off value to consider initiation or escalation of therapy. Although not the focus of this study, 6MWT emerged as another predictor of survival independently of BNP and could be a useful adjunct in guiding therapy. In contrast, no clinically relevant prognostic value of WHO functional class could be established in this study. This highlights the limitation of subjective parameters of exercise capacity in patients with complex congenital heart disease. It is likely that these patients have made lifelong adaptations to their cardiovascular disease and cyanosis due to its slow progression, so that subjective symptoms do not fully reflect the true extent of exercise intolerance.29
Few data are available on the impact of disease targeting therapies on BNP concentrations.30 31 Our results support the notion that treatment is associated with a reduction in BNP concentrations. This finding is reminiscent of the effect of afterload reduction in patients with acquired heart failure and left ventricular dysfunction. In this setting angiotensin receptor blockers were found to cause a sustained reduction in BNP concentrations, and temporal changes in BNP concentrations were identified as important predictors of outcome. In theory, this reduction in BNP concentration could be due to a selection bias. Results from a previous study from our institution suggest that Eisenmenger patients commenced on disease targeted therapies are more symptomatic and have more advanced disease.4 Yet, this would only support the notion that disease targeted therapies reduce BNP values in this setting, despite being potentially applied to sicker patients. Ultimately, however, the impact of disease targeting therapies on BNP concentrations needs to be addressed as part of prospective studies with appropriate randomisation to avoid bias.
Study limitations
This was a retrospective study and we cannot exclude the possibility that patients included represent a biased sample favouring those with more symptoms and more complex disease. The patients included in the current study represent approximately 80% of all Eisenmenger patients under regular follow-up at our centre and should, therefore, be fairly representative of our population of patients with Eisenmenger syndrome.
Conclusion
Plasma BNP concentrations are elevated in patients with Eisenmenger syndrome and relate to higher risk of death, with plasma BNP concentrations above 100 pg/ml (≈30 pmol/l) being associated with a 4.6-fold increase in mortality. In addition, temporal changes in BNP concentrations were also found to be of prognostic significance and PAH specific treatment was associated with a reduction in BNP concentrations. BNP measurements may thus be useful in predicting mortality and guiding disease targeting therapies in patients with Eisenmenger syndrome.
Key messages
B-type natriuretic peptide (BNP) concentrations predict outcome in contemporary Eisenmenger patients.
Increases in BNP concentrations over time are also of prognostic significance.
Disease targeting therapies may help to reduce BNP concentrations in this population, while treatment-naïve patients have static or rising BNP concentrations.
References
Footnotes
See Editorial, p 681
Competing interests Dr Diller has received unrestricted educational grants from Actelion, UK and has served on the advisory board of Actelion, Germany. Professor Gatzoulis has served on the advisory board of Actelion, Pfizer, and GlaxoSmithKline and has received unrestricted educational grants from Actelion and Pfizer, UK. Dr SJ Wort has received educational grants from Actelion and has served on the advisory boards of Pfizer, Bayer and Eli-Lilly.
Ethics approval Ethics approval was provided by Royal Brompton Ethics Commitee.
Provenance and peer review Not commissioned; externally peer reviewed.