Article Text

Abstract
Background Although recent studies contributed to an improved understanding of the prognosis of patients undergoing tricuspid valve (TV) surgery, the data are limited to certain causes of tricuspid regurgitation (TR) or types of surgery.
Objective This study aimed to identify predictors of clinical outcomes of patients undergoing TV surgery for severe TR of various aetiologies.
Design A retrospective cohort study.
Setting A single tertiary referral centre.
Patients 449 consecutive patients (152 men, aged 56.2±12. 3 years) who underwent TV surgery (397 repairs and 52 replacements) due to severe TR between 1997 and 2010.
Main outcome measures The primary outcome of interest was death from any cause.
Results The early death rate was 4.2% (n=19) and 101 patients died in the late period (median follow-up of 63.3 months; range 0−210.4 months). The 5- and 10-year survival rates were 82.4±1.9% and 71.7±2.8%, respectively. Cox-regression analysis revealed that age (HR=1.03; 95% CI 1.01 to 1.05), male gender (HR=1.96; 95% CI 1.29 to 2.99), New York Heart Association functional class IV (HR=2.08; 95% CI 1.31 to 3.30), presence of liver cirrhosis (HR=2.51; 95% CI 1.11 to 5.68) and preoperative levels of haemoglobin (HR=0.89; 95% CI 0.80 to 0.99), albumin (HR=0.52; 95% CI 0.33 to 0.81) and estimated glomerular filtration rate (HR=0.86; 95% CI 0.78 to 0.95) were independent determinants of mortality. Procedural type (p=0.58) or causes of TR (p=0.97), however, were not predictive of mortality.
Conclusions Long-term survival after TV surgery for severe TR was affected by several preoperative factors including advanced heart failure symptom, comorbidity, end-organ dysfunction and laboratory abnormalities, but not by the type of surgery or causes of TR.
Statistics from Altmetric.com
Introduction
In the management of severe tricuspid regurgitation (TR), there remain many areas of uncertainty with regard to surgical indications and procedural choices. Since many clinical reports had described the prognosis of patients undergoing tricuspid valve (TV) replacement or isolated TV surgery as very poor,1–4 efforts have been made to determine predictors of clinical outcomes, thereby offering appropriate selection criteria for surgery.5–7 Consequently, several clinical variables such as the patient's performance status, parameters of right ventricle (RV) function and laboratory findings were found to be important in determining long-term clinical outcomes following TV replacement or isolated TV surgery.7–10 Furthermore, results from these studies indicated that by adopting relatively early surgery before the onset of worse prognostic indicators, optimal outcomes can be achieved with minimum risks of surgery.
The cited reports, however, had focused only on certain causes of TV disease (primary isolated vs secondary) or types of surgery (replacement vs repair). Consequently, the study results may not be generalisable in describing the prognosis of overall severe TR patients undergoing surgery that we meet in the real clinical practice. In this regard, comprehensive analyses of overall severe TR patients undergoing TV surgery that consider aetiology and types of surgery as potential predictors of outcomes will be important. Therefore, this study aimed to identify predictors of clinical outcomes of patients undergoing TV surgery for severe TR of various aetiologies.
Methods
Patients
We used our institution's database, which prospectively registers baseline patient characteristics, results of cardiac evaluations, detailed information on surgery and perioperative complications of patients undergoing cardiac surgery. We identified 472 patients aged 18 years or older as having undergone TV surgery in the presence of severe TR between January 1997 and September 2010 at the Asan Medical Center, Seoul, Korea. Of the 472 patients, those that were diagnosed with Ebstein anomaly (n=2) and those who underwent previous TV surgery (n=20) were excluded. In addition, we excluded one patient who underwent palliative surgery for advanced cancer, resulting in a final number of 449 patients in this study. This study was approved by the institutional Ethics Committee/Review Board at the Asan Medical Center, which waived the requirement for informed patient consent due to the retrospective nature of the study.
Echocardiography
Two-dimensional echocardiography and Doppler colour-flow imaging were performed using a Hewlett Packard Sonos 2500 or 5500 imaging system equipped with a 2.5 MHz transducer (Hewlett-Packard, Andover, Massachusetts, USA). All patients underwent preoperative echocardiography within 2 months before surgery. The end-systolic and end-diastolic dimensions of the left ventricle (LV) were measured from parasternal M-mode acquisitions, and end-systolic volume, end-diastolic volume and ejection fraction of the LV were calculated using the biplane Simpson method. The distal jet area of TR was measured in mid-systolic phase using the apical four-chamber view and TR severity was assessed by distal jet area on colour Doppler imaging. Severe TR was defined as when the distal jet area was 10 cm2 or more or there was systolic flow reversal in hepatic veins.11 ,12 RV end-diastolic and end-systolic dimensions were measured in the RV outflow tract from the parasternal views.
Surgical procedures
The surgical approach consisted of a median sternotomy (n=388) or a port assisted right mini-thoracotomy (n=61) approach according to the surgeon's preferences. Conventional ascending aorta and bicaval cannulation were used for the sternotomy approach, and the minimally-invasive approach involved peripheral cannulation through the right internal jugular vein, right femoral vein and right femoral artery. TV repair was performed in 397 patients, whereas 52 patients underwent TV replacement using either a bioprosthetic (n=19) or mechanical valve (n=33). The decision to perform TV repair or replacement was affected by the patient's preoperative clinical conditions, echocardiographic parameters and intraoperative findings of TV, but was ultimately at the discretion of the attending surgeon. For instance, TV replacement was preferred over repair in cases with TV leaflet abnormality (ie, rheumatic involvement) or severe degree of tethering/annular dilatation where TV repair failure is expected to be high. In cases of functional TR secondary to left-sided valve diseases, however, TV repair was preferred in expectation of improved RV geometry following the correction of left-side valve lesion and consequent regression of pulmonary hypertension.
Definitions and data collection
The primary outcome of interest was death from any cause. The secondary outcome was defined as a composite of all-cause death, requirements for a TV reoperation or heat transplantation, and readmission due to congestive heart failure. Data were obtained through July 2011 during regular visits to the outpatient clinic or by telephone interviews. For validation of complete follow-up, information regarding mortality, data on vital status, and dates and causes of death was obtained through 31 July 2011 from the Korean National Registry of Vital Statistics. Early mortality was defined as death within 30 days of surgery.
Statistical analysis
Categorical variables, presented as frequencies and percentages, were compared using the χ2 test or Fisher's exact test. Continuous variables, expressed as mean±SD or median with range, were compared using Student's unpaired t test or the Mann–Whitney U test, as appropriate. Kaplan–Meier curves were used to delineate the survival rate or freedom from major adverse events, and log-rank tests were used to compare the between-group differences in the rates. For multivariable analyses, the Cox-proportional hazards models were used to determine the risk factors of death and adverse events. Variables listed in tables 1 and 2 were evaluated in the models, and those with a p value of 0.20 or less in univariable analyses were candidates for the multivariable Cox models. Multivariable analyses involved a backward elimination technique and only variables with a p value of less than 0.10 were used in the final model. Final models were validated in 1000 bootstrap samples. For further verification of the results of Cox-regression analysis in comparison with TV replacement and repair, propensity score analysis was performed. The propensity scores were estimated without regard to outcome variables by multiple logistic regression analysis. A propensity score model was developed that included all the variables shown in tables 1 and 2. The individual propensity score was incorporated into the Cox-regression model as a covariate and type of TV surgery to calculate the propensity-adjusted HR. SPSS software V.14.0 (IBM Inc, Chicago, Illinois, USA) was used for statistical analyses.
Baseline demographic and laboratory profiles
Preoperative echocardiographic parameters and operative procedures
Results
Baseline characteristics
Mean age at surgery was 56.2±12.3 years and 152 patients (33.9%) were male subjects. Overall, 213 (47.4%) were in New York Heart Association (NYHA) functional class III or IV and 13 patients (2.9%) had liver cirrhosis. A total of 60 patients (13.4%) had a previous history of left-sided valve surgery and 359 (80.0%) underwent concomitant left-sided valve surgery. Table 1 summarises baseline demographic and laboratory profiles of the patients. In summary, patients who underwent TV repair had a higher preoperative haemoglobin level, were more likely to have atrial fibrillation and to have a previous history of left-sided valve surgery; these patients were also more likely to undergo a concomitant Maze procedure in the presence of atrial fibrillation than those who underwent a TV replacement.
On preoperative echocardiographic evaluations, TR jet area was larger with patients who underwent TV replacement than those who underwent TV repair. In addition, TV leaflet abnormalities were more commonly seen with TV replacement patients (table 2). Parameters of left heart function such as LV ejection fraction, LV dimension, LV mass and degree of pulmonary hypertension exhibited less favourable findings in TV repair patients because TR was more commonly associated with left-side valvular heart diseases in this patient group (85.9% vs 34.6%, p<0.001).
Early outcomes
Aortic cross clamping (ACC) and cardiopulmonary bypass (CPB) times were 92.9±41.3 and 147.1±68.9 min, respectively. Although ACC and CPB times did not significantly differ between TV repair and replacement (p=0.26 and >0.99, respectively), both durations were significantly longer in patients who underwent combined surgery (n=370) than those who underwent isolated TV surgery (n=79) (ACC time: 98.5±40.3 vs 57.4±28.2 min, p<0.001; CPB time: 156.6±68.7 vs 103.2±50.4 min, p<0.001).
Early death rate was 4.2% (n=19). Causes of early death were low cardiac output syndrome in nine patients, pulmonary complications in five patients, stroke in two patients, surgical site bleeding in two patients and sepsis complicated with multi-organ failure in one patient. Although there were no significant differences in the rates of early mortality between the TV repair and replacement groups, more patients in the TV replacement group experienced early major complications (table 3).
Early operative outcomes
Overall clinical outcomes
Follow-up was completed in 420 patients (93.5%) with a median follow-up duration of 63.3 months (range, 0−210.4 months). During this period, 101 patients died, 15 patients underwent TV reoperation and 26 patients required readmission due to heart failure. The 15 reoperations (at a median of 31.0 months after initial surgery (range 10.4–167.0 months)) involved heart transplantation in two patients, TV rerepair in three and TV replacement in 10. TV repair or replacement was done under arrested heart in nine patients and under beating heart in four patients. Early mortality occurred in one patient who underwent TV rerepair under beating heart at 65.1 months after initial surgery, in whom the cause of death was postoperative cardiac failure. The 5- and 10-year survival rates were 82.4±1.9% and 71.7±2.8% years, respectively.
Major adverse outcomes are summarised in table 4. Figure 1 depicts the unadjusted overall survival, freedom from TV reoperation and major event-free survival in the two groups. There were no significant differences in the rates of death or major adverse events between TV repair and replacement.
Major adverse outcomes during follow-up

Unadjusted Kaplan−Meir curves for overall survival (A), freedom from TV reoperation (B), TV reoperation and CHF-free survival (C) and major event-free survival (D). Major events included all valve-related complications and readmission due to CHF. CHF, congestive heart failure; TV, tricuspid valve.
Predictors of mortality and major adverse outcomes
On multivariate Cox-regression analysis, age, male gender, NYHA functional class IV, presence of liver cirrhosis and preoperative levels of haemoglobin, albumin, and estimated glomerular filtration rate (eGFR) emerged as significant and independent predictors of all-cause mortality (table 5). However, none of the followings were predictive of mortality: the type of procedure (replacement vs repair; HR=1.18; 95% CI 0.66 to 2.11, p=0.58), the cause of TR (primary isolated vs secondary; HR=0.99; 95% CI 0.58 to 1.69, p=0.97) and the presence of leaflet abnormality (HR=0.90; 95% CI 0.54 to 1.51, p=0.69).
Multivariable Cox-regression analysis: predictors of all-cause mortality and secondary outcomes
For secondary outcome (a composite of death, TV reoperation and congestive heart failure), age, male gender, NYHA functional class IV, diabetes mellitus, presence of liver cirrhosis, and preoperative levels of haemoglobin and albumin were significant and independent predictors (table 5). When primary and secondary outcomes of TV replacement were compared with TV repair using propensity score adjustment models, both treatments showed similar rates of death (HR 1.08, 95% CI 0.47 to 2.49, p=0.85) and composite-secondary outcomes (HR 0.97, 95% CI 0.46 to 2.03, p=0.93).
The predictive values of initial laboratory findings for long-term mortality were assessed by using the receiver operating characteristic curve. The curve yielded areas under the curve of 0.642 (95% CI 0.577 to 0.708; p<0.001) for haemoglobin, 0.626 (95% CI 0.554 to 0.698; p<0.001) for albumin and 0.63 (95% CI 0.568 to 0.697; p<0.001) for eGFR. The greatest accuracy for the prediction of mortality was obtained at the cut-off values of 11.65 g/dl for haemoglobin (54.1% sensitivity and 73.1% specificity), 3.65 g/dl for albumin (53.6% sensitivity and 73.5% specificity) and 63.5 ml/min/1.73 m2 for eGFR (52.6% sensitivity and 72.0% specificity). Figure 2 shows distinct survival differences using these cut-off values of laboratory findings as well as according to preoperative NYHA functional class.
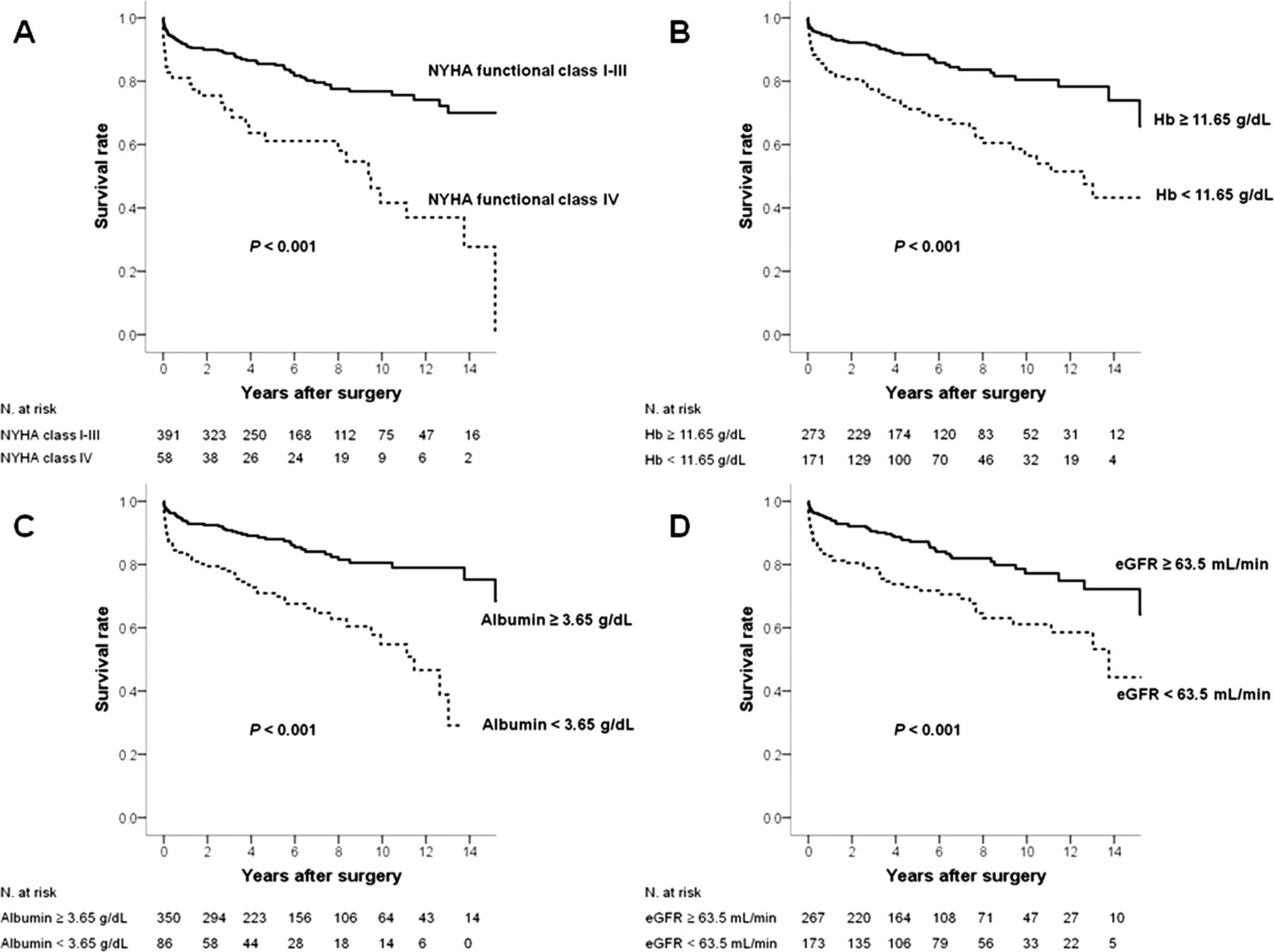
Survival curves according to (A) NYHA functional class and initial levels of (B) haemoglobin, (C) albumin and (D) eGFR. eGFR, estimated glomerular filtration rate; NYHA, New York Heart Association.
Discussion
Surgical results of TV replacement or isolated TV surgery have been documented as poor, with 10%–30% early mortality in most reports.1–3 ,9 ,13 However, several reports suggest that TV replacement itself is not a risk factor for poor outcome, but the patient's conditions that led to TV replacement may be the culprit for poor survival. For instance, a group conducted a propensity score matched comparison between TV replacement and repair for treatment of TR.6 For the matched cohort, early mortality (13% in replacement and 18% in repair, p=0.64) and overall long-term survival rates (p=0.66) were similar. These findings indicate that a patient's preoperative characteristics determine the overall prognosis rather than the type of procedure for a TV surgery. Furthermore, these findings support the idea of performing TV replacement rather than repair in patients for whom there is a reasonable risk of the recurrence of significant TR after repair. For instance, TV tethering is an important and typical risk factor of recurrent or residual TR following TV repair; therefore, in patients with high degree of TV tethering, TV replacement may be a preferred option over TV repair to reduce the late TR.14
High death rates were also observed in patients undergoing TV surgery for severe TR secondary to mitral valve disease.8 ,10 McGrath et al reviewed 530 patients undergoing multi-valvular surgery including TV surgery.10 The early death rate was 15% and the survival rate was only 20% at 15 years. The authors found that survival was negatively affected by male gender, hepatomegaly and lack of postoperative anticoagulation therapy. These findings suggest that the presence of severe TR itself is the indicator of ‘high surgical risk’ in patients with secondary TR and that clinical findings of right heart failure and consequent end-organ damage are poor prognostic markers of long-term survival, even in secondary TR patients.
In this regard, data on comprehensive analysis involving overall severe TR patients undergoing TV surgery are lacking to date. The present study was conducted with the hypotheses that right heart failure, and consequent cardiac cachexia and end-organ damage, are the culprits of poor prognosis following TV surgery. As a result, we found that long-term outcomes were determined primarily by underlying comorbidity and not by aetiology of TR or TV procedural types. The study findings also suggest that unlike ‘less-than-severe’ functional TR, in which excellent outcomes can be achieved with minimum risk of mortality even without concomitant TV repair, ‘severe’ functional TR should be viewed with caution during left-heart valve surgery, because there is a great propensity for high surgical risks.15
Current guidelines indicate that TV surgery can be considered for severe TR only when symptoms of heart failure exist.16 ,17 Paradoxically, evidences are compelling that symptomatic TR patients carry much higher surgical mortality compared with asymptomatic patients or those with milder degree of heart failure symptoms. Therefore, a symptom-guided surgical indication may render overall outcomes even poorer.7 ,9 Contrary to left-sided valve lesions where we no longer wait until patients develop severe heart failure symptoms or overt LV dysfunction before referral for surgery, we have not evolved to that point yet with tricuspid surgery. In this regard, it is of utmost importance to find reliable and reproducible markers to set more appropriate criteria for earlier surgical referral instead of the current ‘symptom-guided’ indication. Unlike LV, functional evaluation of RV is difficult using conventional two-dimensional echocardiographic measurements due to unique three-dimensional structural characteristics.18 Although three-dimensional echocardiography or cardiac magnetic resonance studies are accepted as promising modalities in the assessment of RV functions,19–21 routine uses of such equipment may be limited in real clinical practices. In this situation, laboratory findings of cardiac cachexia and end-organ damage may be useful markers for estimating surgical risks.5
In the present study, we found several laboratory markers (haemoglobin, albumin and GFR) that are commonly used in clinical practice very useful in the prediction of long-term prognosis following TV surgery. Interestingly, cut-off values of those laboratory findings in the differentiation of long-term survival were formed at low limits of the reference values indicating that it is too late to undertake surgery when overt laboratory abnormalities exist. The influences of preoperative hepatic and renal dysfunction on adverse outcomes observed in this study were also reported by previous studies.5 ,7 ,9 ,10 Furthermore, preoperative anaemia is also reported to be a poor prognostic indicator following major cardiac surgery in various clinical settings.13 ,22–25 The aetiology of this anaemia is known as ‘anaemia of chronic disease’ in a significant proportion of patients,26 and is attributable to chronic hepatic/renal dysfunctions and congestive heart failure, all of which are also associated with low serum albumin level. In two large-scale prospective observational studies involving consecutive cardiac surgical patients, 26%–28% of patients were found to have preoperative anaemia (<12–13 mg/dl).23 ,24 The results of these studies were uniform as follows: (1) anaemic patients exhibited high risk features compared with non-anaemic patients such as older age, higher EuroSCORE and greater chances of having major comorbidity, heat failure and renal dysfunction and (2) preoperative anaemia was independently associated with adverse clinical outcomes even after adjustments for significant risk factors. In the present study, the prevalence of anaemia according to WHO definition (haemoglobin level of <13 g/dl for men and <12 g/dl for women) was as common as 42.8% (n=192), which is significantly higher than previous series. With the cut-off value of 11.6 g/dl which showed a distinct survival difference in current study, the prevalence of anaemia was 32.5% (n=146). Regarding improved outcomes that can be achieved before haemoglobin level reaches to this cut-off point, the criteria of anaemia defined by WHO may be a reasonable threshold of early referral for TV surgery.
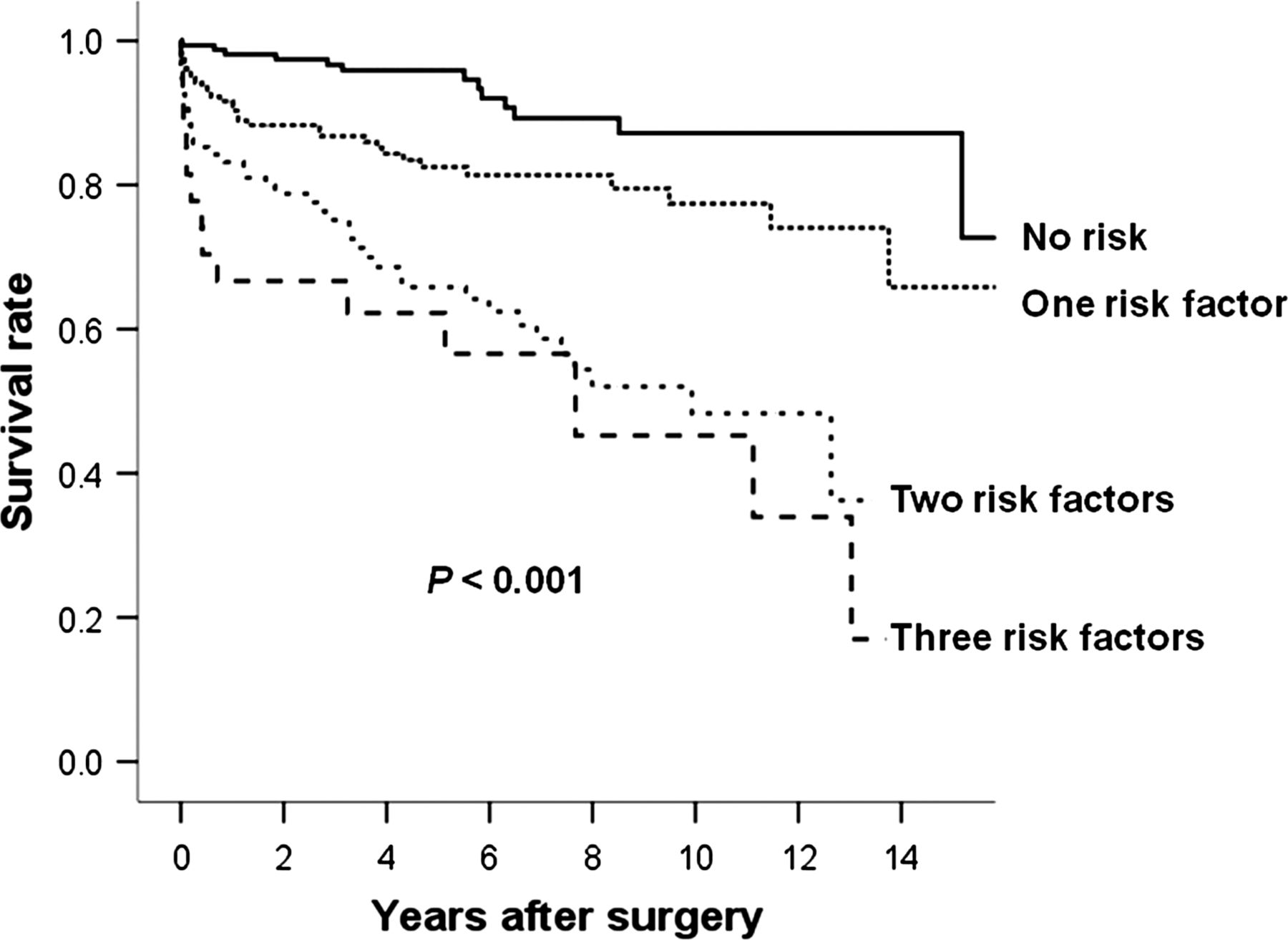
Of note, the influence of preoperative laboratory findings was not confined to the early postoperative period, but extended to the late period, as seen in the survival curves (figure 2), which diverge over time according to the cut-off values, even long after surgery. Early death rates differed according to the number of laboratory risk factors (haemoglobin, albumin and eGFR) that each patient has; for instance, they were 0.6%, 3.3%, 9.2% and 11.1% in patients with no risk factor, one factor, two factors and three factors, respectively (p<0.001). Furthermore, long-term survival rates showed striking differences as shown in figure 3, in that 5-year survival rates were 95.9% in patients with no risk, and 82.5%, 65.8% and 62.2% for those with a single risk factor, two factors and three factors, respectively (p<0.001). These findings strongly implicate that early surgical referral before the onset of overt laboratory abnormality is of utmost importance to improve both short- and long-term outcomes. These objective parameters, with cut-off values suggested in the present study, may play a substantial role for determining the indications of earlier referral to surgical intervention in asymptomatic patients or those with vague symptoms.
{kind=link}
{kind=link}
{kind=link}
Survival curves according to the number of laboratory risk factors. Laboratory risk factors are as follow: (1) haemoglobin <11.65 g/dl, (2) serum albumin <3.65 g/dl and (3) estimated glomerular filtration rate <63.5 ml/min/1.73 m2.
Limitations
This study is subject to the limitations inherent to a retrospective analysis of observational data.
Several echocardiographic parameters are used in the evaluation of TR severity; however, every method has its limitations. In this study, jet area method and hepatic vein systolic reversal were used for defining severe TR. Although the jet area method offers simple and quick screening of TR, it is subject to technical and haemodynamic factors, and may underestimate severity in eccentric jets. Hepatic vein systolic reversal is sensitive for severe TR, but is influenced by right atrial (RA) pressure and atrial fibrillation (AF)12 Sophisticated variables such as tricuspid annular dimension, the degree of TV tethering and quantitative parameters of RV function could not be estimated.
Conclusions
Long-term clinical outcomes following surgery for severe TR were affected by the patient's performance status, comorbidity, liver cirrhosis and laboratory abnormalities including anaemia, hypoalbuminaemia and decreased renal function, but not by the type of surgery (repair vs replacement) or cause of TR. Therefore, earlier TV surgery should be considered, with liberal choice of TV procedure according to individual patient conditions and the surgeon's discretion, before the development of such findings.
References
Footnotes
-
Contributors Each author substantially contributed to the research. In detail: JBK and JWL contributed to the conception and design of the study; JBK contributed to data collection, analysis and interpretation of the results; SJ, SJC, CHC and JWL drafted and revised the manuscript. All authors read and approved the final version of the manuscript.
-
Competing interests None.
-
Ethics approval IRB of Asan Medical Center.
-
Provenance and peer review Not commissioned; externally peer reviewed.