Article Text

Abstract
Aims Sudden cardiac death (SCD) is a common mode of death in hypertrophic cardiomyopathy (HCM), but identification of patients who are at a high risk of SCD is challenging as current risk stratification guidelines have never been formally validated. The objective of this study was to assess the power of the 2003 American College of Cardiology (ACC)/European Society of Cardiology (ESC) and 2011 ACC Foundation (ACCF)/American Heart Association (AHA) SCD risk stratification algorithms to distinguish high risk patients who might be eligible for an implantable cardioverter defibrillator (ICD) from low risk individuals.
Methods and results We studied 1606 consecutively evaluated HCM patients in an observational, retrospective cohort study. Five risk factors (RF) for SCD were assessed: non-sustained ventricular tachycardia, severe left ventricular hypertrophy, family history of SCD, unexplained syncope and abnormal blood pressure response to exercise. During a follow-up period of 11 712 patient years (median 6.6 years), SCD/appropriate ICD shock occurred in 20 (3%) of 660 patients without RF (annual rate 0.45%), 31 (4.8%) of 636 patients with 1 RF (annual rate 0.65%), 27 (10.8%) of 249 patients with 2 RF (annual rate 1.3%), 7 (13.7%) of 51 patients with 3 RF (annual rate 1.9%) and 4 (40%) of 10 patients with ≥4 RF (annual rate 5.0%). The risk of SCD increased with multiple RF (2 RF: HR 2.87, p≤0.001; 3 RF: HR 4.32, p=0.001; ≥4 RF: HR 11.37, p<0.0001), but not with a single RF (HR 1.43 p=0.21). The area under time-dependent receiver operating characteristic curves (representing the probability of correctly identifying a patient at risk of SCD on the basis of RF profile) was 0.63 at 1 year and 0.64 at 5 years for the 2003 ACC/ESC algorithm and 0.61 at 1 year and 0.63 at 5 years for the 2011 ACCF/AHA algorithm.
Conclusions The risk of SCD increases with the aggregation of RF. The 2003 ACC/ESC and 2011 ACCF/AHA guidelines distinguish high from low risk individuals with limited power.
Statistics from Altmetric.com
Introduction
Sudden cardiac death (SCD) secondary to sustained ventricular arrhythmias is a common mode of death in hypertrophic cardiomyopathy (HCM).1 However, identification of patients who are at high risk of SCD and thus likely to benefit from an implantable cardioverter defibrillator (ICD) is challenging because of the low absolute risk of SCD and the marked clinical heterogeneity of the disease.2 ,3 In 2003, the American College of Cardiology (ACC) and European Society of Cardiology (ESC) proposed a SCD risk stratification and treatment algorithm based on the assessment of a small number of clinical features (non-sustained ventricular tachycardia (NSVT), severe hypertrophy, unexplained syncope, family history of SCD (FHSCD) and blood pressure response to exercise) shown in observational cohort studies to associate with an increased risk of SCD.4 Assuming that these features reflect the severity of the underlying arrhythmic substrate, the presence of multiple risk factors (RF) in an individual patient was considered sufficient justification for primary prevention ICD implantation. Recommendations for ICD therapy in patients with a solitary RF were less precisely defined, reflecting a concern that a restrictive recommendation to implant an ICD only in patients with multiple RF would result in a failure to treat some vulnerable patients.4
Although the ACC/ESC guidelines have never been formally validated, a similar approach has been endorsed in a recent position statement by the ACC Foundation (ACCF) and American Heart Association (AHA).5 While the two guidelines agree on the management of patients with multiple RF, the ACCF/AHA document recommends ICD implantation as a reasonable measure in patients with severe hypertrophy, unexplained syncope or FHSCD in isolation. Importantly, the ACCF/AHA guidelines consider NSVT and abnormal blood pressure response significant only when they occur in the presence of other clinical RF.
Accurate identification of patients who are at substantial risk of SCD is important to save lives and to protect low risk patients from the relatively high lifetime risk of device-related complications. Moreover, increasing pressure on healthcare resources makes it essential to target therapy at those individuals who are most likely to benefit. The absence of randomised trial data in patients with HCM makes determination of the impact of ICDs on survival problematic, but an appropriate device discharge rate of around 5% per annum provides some evidence that they afford protection to many patients.6 Equally, the fact that the majority of ICD recipients do not receive therapies and often experience device-related complications suggests that the current risk algorithm needs to be improved.6 The primary aim of this study was to assess the performance of the 2003 ACC/ESC and 2011 ACCF/AHA SCD risk stratification and treatment algorithms by determining their ability to distinguish high from low risk patients.
Methods
Study design
An observational, retrospective, longitudinal cohort study design was used. The study conforms to the principles of the Helsinki declaration. All authors have read and agreed to the manuscript as written.
Study population
The cohort consisted of all consecutively evaluated adult patients (≥16 years of age) with HCM who were evaluated in a dedicated cardiomyopathy clinic between 1988 and 2005. HCM was diagnosed in the presence of left ventricular hypertrophy (LVH) (more than two SDs from the normal range corrected for age and body size) in the absence of haemodynamic conditions that could account for the observed degree of hypertrophy or in accordance with criteria for the diagnosis of familial disease in patients with at least one first-degree relative with an unequivocal diagnosis of HCM.7 ,8 For the purpose of this study, patients with a history of aborted SCD or sustained ventricular arrhythmia prior to their first evaluation were excluded from the analysis. Patients with Friedreich's ataxia, Noonan syndrome and metabolic disorders that can cause ventricular hypertrophy were omitted from the analysis.
Patient assessment
Patients underwent clinical examination, resting and ambulatory electrocardiography, echocardiography and symptom limited exercise testing as previously described.3 RF for SCD were assessed at baseline and defined as follows:
-
Severe LVH: maximal left ventricular wall thickness ≥30 mm using echocardiography.4 ,5
-
Abnormal systolic blood pressure response to exercise (ABPRE): <25 mm Hg rise in systolic blood pressure from rest to peak exercise and/or >10 mm Hg drop from maximal systolic blood pressure when exercised to exhaustion on a treadmill or an upright bicycle ergometer. ABPRE was considered a RF only in those ≤40 years of age in accordance with previously published studies.3 ,9–11
-
Unexplained syncope: unexplained transient loss of consciousness at or prior to first evaluation. Vasovagal syncope was not considered a RF.4
-
FHSCD: one or more SCD in relatives <40 years of age or SCD in a relative with confirmed HCM at any age.4
-
NSVT: ≥3 consecutive ventricular extra systoles at a rate of ≥120 beats/min lasting <30 s during Holter monitoring.4 ,5
Endpoints and follow-up
All patients were routinely evaluated every 6–12 months or earlier if there was a clinical event, up to and including 14th January 2010. The primary endpoint was SCD defined as: witnessed or aborted SCD with or without documented ventricular fibrillation; death within 1 h of new symptoms; nocturnal deaths with no antecedent history of worsening symptoms; or an appropriate ICD shock for ventricular tachycardia or fibrillation as previously described.3 All ICDs had the capacity to store intracardiac electrograms and therapies were independently verified by two investigators (CO and PL) as previously described.6
Statistical analysis
STATA (V.11.1) was used for descriptive statistics and survival analysis. Normally distributed continuous data are expressed as mean±SD and non-normally distributed data as median and IQR. The percentage of categorical data is shown in parentheses. The follow-up period was calculated from the dates of first evaluation and reaching an endpoint. In patients not reaching the endpoint, the follow-up period extended to the most recent evaluation or censoring event up to 14th January 2010. The annual event rate was calculated by dividing the number of patients reaching an endpoint by the total follow-up period and expressed as a percentage. The cumulative probability for the occurrence of an endpoint was estimated using the Kaplan–Meier method and hazard ratios (HR) were calculated using Cox regression. HRs are presented with 95% CIs and p values. A two-sided p value <0.05 was considered significant.
The discriminating performance of the risk stratification algorithms was determined from time-dependent receiver operating characteristic (ROC(t)) curves using the Kaplan–Meier survivor function method.12 The 2003 ACC/ESC guidelines give each SCD RF equal weight and the RF profile is calculated as the simple arithmetic sum of the RF present. The 2011 ACCF/AHA guidelines consider NSVT and ABPRE significant only when occurring in association with other established RF. Thus, when calculating the RF profile of each patient with the 2011 ACCF/AHA guidelines, NSVT and ABPRE were not coded as RF when they occurred in isolation. The impact of emerging risk modifiers as defined in the ACCF/AHA guidelines could not be assessed. Missing data on RF were coded as absent. For the purposes of this analysis, the RF profile of each patient was considered as a continuous prognostic marker for SCD, ranging from 0 (when all RF were absent) to 4 (when four or more RF were present). The ROC curve was constructed by plotting the sensitivity against (1-specificity) when the dichotomised RF profile was higher than a particular prognostic threshold for all possible prognostic values (ie, ≥0 RF, ≥1 RF, ≥2 RF, ≥3 RF and ≥4 RF) and then calculating the area under the curve (AUC). This analysis was carried out in R (V.2.12.1) using the SurvivalROC package.12 The positive predictive value (PPV) of a particular RF profile was calculated by dividing (sensitivity × prevalence) by ((sensitivity × prevalence)+(1−specificity) × (1−prevalence)) and expressed as a percentage. The negative predictive value (NPV) of a particular RF profile was calculated by dividing (specificity × (1−prevalence)) by ((1−sensitivity × prevalence)+(specificity × 1−prevalence)) and expressed as a percentage.13
Results
Clinical characteristics
The study cohort consisted of 1606 patients. The baseline clinical characteristics are shown in table 1. HCM was diagnosed in 1474 patients (92%) using conventional diagnostic criteria and in 132 patients (8%) using the criteria for familial disease.8 During follow-up, 53 (3%) patients underwent alcohol septal ablation, 139 (9%) septal myectomy and 7 (0.4%) both procedures. During the study period, 302 (19%) patients were treated with an ICD.
Baseline clinical characteristics
Incidence of SCD or appropriate ICD shock during follow-up
During a follow-up period of 11 712 patient-years (median 6.6; IQR 4.1–10.0), 89 patients (6%) suffered SCD or an appropriate ICD shock with an annual rate of 0.75%/year (95% CI 0.6 to 0.9) and a 5-year cumulative incidence of 4% (95% CI 2.96 to 5.0). The combined endpoint consisted of 22 appropriate ICD shocks (25%), 57 SCD (64%) and 10 aborted SCD (11%).
Incidence of SCD/appropriate ICD shock and RF profile
The prevalence of each of the five major RF and the RF profile at baseline according to the 2003 ACC/ESC guidelines is shown in table 2. The endpoint of SCD/appropriate ICD shock was reached by 20 (3%) of the 660 patients with no RF (annual rate 0.45%, 95% CI 0.29 to 0.70), 31 (4.8%) of the 636 patients with one RF (annual rate 0.65%, 95% CI 0.45 to 0.92), 27 (10.8%) of the 249 patients with two RF (annual rate 1.3%, 95% CI 0.89 to 1.90), 7 (13.7%) of the 51 patients with three RF (annual rate 1.9%, 95% CI 0.92 to 4.10) and 4 (40%) of the 10 patients with four or more RF (annual rate 5.0%, 95% CI 1.88 to 13.4). The SCD/appropriate ICD shocks rates and the absolute number events in relation to RF profile are illustrated in figure 1.
Prevalence of major risk factors

Annual sudden cardiac death (SCD)/appropriate implantable cardioverter defibrillator (ICD) shocks rates and the absolute number events in relation to the 2003 American College of Cardiology/European Society of Cardiology (ACC/ESC) risk factor profile. (A) The annual SCD/appropriate ICD shocks rates with 95% CIs for each risk factor subgroup. (B) The bars represent the absolute number of events for each risk factor subgroup. The parentheses contain the number of SCD/appropriate ICD shocks divided by the population at risk for each risk factor subgroup (prevalence). Despite the low incidence of SCD in patients with one or no risk factors, these two subgroups contributed the majority of SCD/appropriate ICD shocks (57%) in the study population. The annual SCD/appropriate ICD shocks rates are inversely proportional to the absolute number events because the lower risk subgroups are larger in size.
The presence of a single RF was not associated with an increased risk of SCD/appropriate ICD shock when compared with no RF (HR 1.43, 95% CI 0.82 to 2.51, p=0.21). The rates of SCD in patients with a single RF are shown in table 3. There was no significant difference in the outcomes of patients with a single RF (Log rank test p=0.75). The Kaplan–Meier curves for each RF in isolation are shown in figure 2.
SCD/appropriate ICD shock in patients with a single risk factor

Kaplan–Meier curves for the cumulative incidence of sudden cardiac death (SCD) or appropriate implantable cardioverter defibrillator (ICD) shock in patients with solitary risk factors. Log rank test p=0.75. ABPRE, abnormal blood pressure response to exercise; FHSCD, family history of SCD; LVH, left ventricular hypertrophy; NSVT, non-sustained ventricular tachycardia.
Compared with patients without RF, those with multiple RF had an increased risk of SCD (2 RF: HR 2.87, 95% CI 1.61 to 5.14, p≤0.001; 3 RF: HR 4.32, 95% CI 1.82 to 10.21, p=0.001; 4 or more RF: HR 11.37, 95% CI 3.85 to 33.62, p<0.0001). The Kaplan–Meier curve stratified according to RF profile is shown in figure 3.

Kaplan–Meier curves for the cumulative incidence of sudden cardiac death (SCD) or appropriate implantable cardioverter defibrillator (ICD) shock, stratified according to risk factor (RF) profile. Log rank test p<0.0001 for both analyses. Panel A illustrates the cumulative incidence of SCD/appropriate ICD shocks according to RF profile. Panel B illustrates the same data stratified according to the presence of multiple (two or more), single and no RF. Patients with multiple RF have a higher risk of SCD compared with those without RF (HR 3.3, 95% CI 1.94 to 5.75, p<0.001). The risk of SCD in patients with a single RF is not significantly different when compared with patients without RF (HR 1.4, 95% CI 0.82 to 2.51, p=0.212). The RF profile is the simple arithmetic sum of the RF present.
Discrimination performance of the 2003 ACC/ESC risk stratification and treatment guidelines
The RF profile was treated as a continuous prognostic marker, ranging from 0 (absent RF) to 4 (when four or more RF were present). The sensitivity and specificity for SCD were determined for all possible prognostic values and the PPV and NPV were then calculated and summarised in table 4. The PPV is the probability that a patient will experience SCD/appropriate ICD shock when classified as high risk at a particular RF threshold. The 2003 ACCC/ESC guidelines recommend an ICD in those with ≥2 RF and the PPV for SCD of this treatment threshold is 23.3% at 5 years. The NPV is the probability of a patient not experiencing SCD/appropriate ICD shock when considered low risk below particular RF threshold. In the absence of all RF there is a 95.3% chance of being free from SCD/appropriate ICD shock at 5 years.
The PPV and NPV of accumulating major risk factors and SCD/appropriate ICD discharge
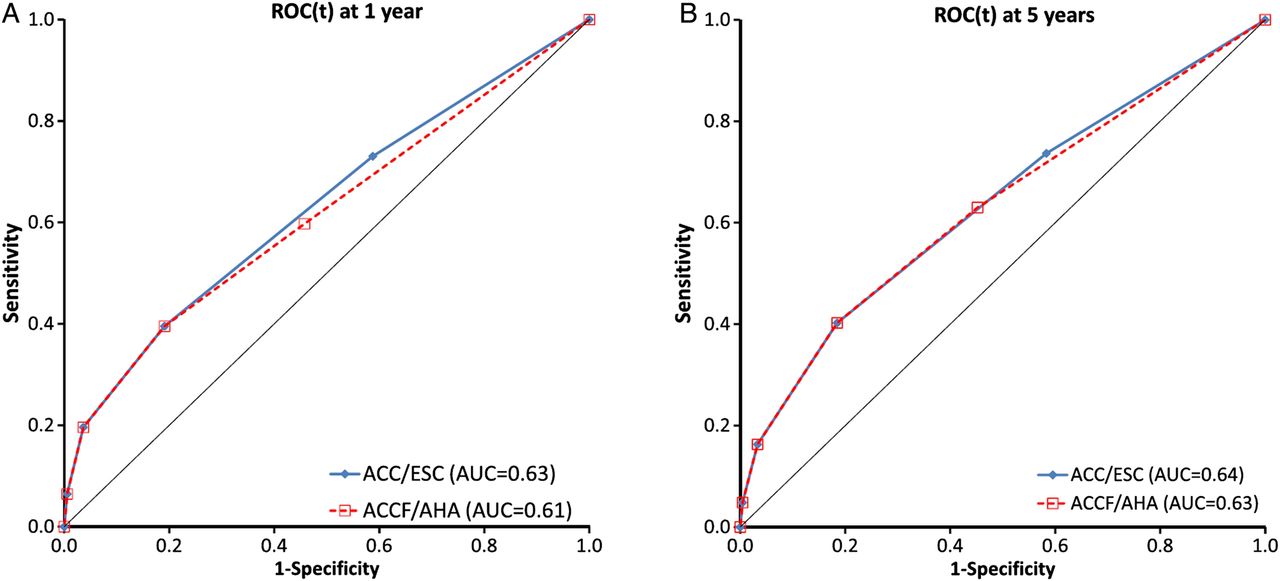
ROC(t) curves were constructed by plotting sensitivity against (1-specificity) as described in the Methods section. The area under the ROC(t) curves, which represents the probability of correctly identifying a patient at risk of SCD/appropriate ICD shock on the basis of their RF profile from random pairs of affected and unaffected patients,14 was 0.63 at 1 year and 0.64 at 5 years. The ROC(t) curves at 1 and 5 years are shown in figure 4.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Receiver operating characteristic (ROC(t)) curves for the American College of Cardiology/European Society of Cardiology (ACC/ESC) and ACC Foundation/American Heart Association (ACCF/AHA) guidelines. Panels A and B show the ROC(t) curves at 1 year and 5 years, respectively. A prognostic test with no discrimination power would lie on the black line where sensitivity equals 1−specificity and have an area under the curve of 0.5. The ROC(t) curves overlap since patients with multiple risk factors are stratified in the same way by both guidelines. The 2011 ACCF/AHA guidelines consider non-sustained ventricular tachycardia and abnormal systolic blood pressure response to exercise significant only in the presence of other risk factors leading to loss of discriminatory power and separation of the two ROC(t) curves.
Discrimination performance of the 2011 ACCF/AHA risk stratification and treatment guidelines
The RF profile was calculated as the arithmetic sum of the assessed RF (NSVT and ABPRE counted only when occurring in association with another established RF). The RF profile was treated as a continuous prognostic marker, ranging from 0 (absent RF) to 4 (when four or more RF were present). The 2011 ACCF/AHA guidelines recommend that an ICD is reasonable in patients with FHSCD, severe LVH or unexplained syncope, and in individuals with NSVT or ABPRE in the presence of other RF. The PPV for SCD/appropriate ICD shock at this RF profile threshold was 9.8% at 1 year and 10.5% at 5 years. The PPV for SCD/appropriate ICD shock for ≥2 RF is identical to the ACC/ESC guidelines. The NPV of the absence of FHSCD, severe LVH, unexplained syncope and NSVT or ABPRE when found with other RF was 94.1% at 1 year and 94.6% at 5 years. The 2011 ACCF/AHA algorithm had an the area under the ROC(t) curves of 0.61 at 1 year and 0.63 at 5 years, as shown in figure 4.
Discussion
Since the development of the ICD in the 1980s,15 appropriately selected HCM patients have been protected from the catastrophic consequences of sustained ventricular arrhythmias. Recipients of ICDs experience appropriate shocks frequently,6 ,16–23 and failure of the device to prevent SCD has been rarely reported.20 ,23 However, the rapid advances in ICD technology and their increasing availability have not been paralleled by similar advancements in risk stratification and as a consequence patient selection for this powerful technology remains suboptimal.
Making use of data from observational studies, the 2003 ACC/ESC guidelines proposed a risk stratification and treatment algorithm based on a number of RF that were previously found to associate with SCD.4 This is the first time since the publication of these guidelines that the ability of the 2003 ACC/ESC SCD risk algorithm to distinguish high from low risk patients has been evaluated. A perfectly discriminating risk stratification strategy will yield an AUC of 1.0, whereas purely random predictions result in an AUC of 0.5.14 The AUC for the 2003 ACC/ESC SCD risk stratification algorithm was 0.64 at 5 years indicating that it is able to distinguish high from low risk individuals but with limited power.24 The relatively low PPVs for SCD, reflecting the low prevalence of SCD in HCM, help explain the relatively low incidence of ICD shocks in HCM ICD recipients selected on the basis of their RF profile, with only a quarter receiving appropriate therapy at 5 years postimplant.6 ,16 ,18 ,19 ,21 The high NPVs support the current recommendation that patients without RF should be reassured.4
More recently, an alternative approach to the primary prevention of SCD has been proposed by the ACCF and AHA.5 While the 2003 ACC/ESC SCD risk stratification algorithm gives equal weight to each RF,4 the ACCF/AHA guideline suggests that greater emphasis should be given to FHSCD, severe LVH and recent unexplained syncope rather than NSVT or abnormal exercise blood pressure responses.5 The results from this study suggest that this change does not increase the ability of the 2011 ACCF/AHA SCD risk stratification algorithm to distinguish high from low risk individuals compared with the earlier ACC/ESC guidelines. This new approach is inconsistent with data from a recent meta-analysis in which the magnitude of the association of severe LVH and NSVT with SCD was greater than that of FHSCD.25 The ACCF/AHA guidelines also differ in the way that RF are used to determine treatment in that ICD implantation is considered reasonable in patients with FHSCD, severe LVH or recent unexplained syncope in isolation. The emphasis on the use of ICD therapy in patients with a single RF arises from the observation that appropriate ICD shocks are not associated with the aggregation of RF in observational studies of HCM patients treated with an ICD.5 ,6 ,18 ,23 However, ICD shocks are not accurate surrogates of SCD26 and generalising the results from these highly selected ICD cohorts to the general HCM population that the guidelines are intended for is questionable and contrary to the findings of larger, unselected HCM cohorts, including this study.10 ,11 ,27 ,28
Even though all patients with HCM have some risk of SCD (including those with no RF), the low overall incidence of SCD and the hazards of lifelong device therapy mean that ICD implantation should be used judiciously. International guidelines agree that HCM patients without RF for SCD should not be treated with an ICD.4 ,5 This study shows that the incidence of SCD in patients with a single RF is not significantly different from those without RF, indicating that the majority of such patients also do not need an ICD. However, as in patients with other disorders such as coronary artery disease,29 there is an inverse relation between the annual rate of SCD and the absolute number of events experienced by each RF subgroup, with the majority of events occurring in low risk subgroups. It is for this reason and the fact that patients with HCM are often young and likely to have an improved prognosis if SCD is prevented that current guidelines equivocate on the issue of ICD therapy in patients with low or intermediate risk.
This study shows that implantation of ICDs in accordance to current guidelines can effectively protect patients from SCD, but their modest discriminatory power means that this practice is at the expense of device implantation in a large number of patients who do not experience events. A major limitation of both the ACC/ESC and ACCF/ACC algorithms is their reliance on relative risk rather than individualised prognostic risk estimates. This detail is important as patients with very different absolute risks are managed in the same way. In addition, all major RF are considered in a dichotomous manner despite the continuous nature of risk. This gives rise to some obvious clinical dilemmas; for example, it is implausible that a maximal wall thickness of 29 mm confers a significantly different risk than a value of 30 mm.
In the absence of an alternative risk stratification strategy, this analysis suggests that patients with multiple RF should continue to be advised that they are likely to benefit from prophylactic ICD implantation. Although the vast majority of patients without multiple RF have a good prognosis, the intrinsic limitations of the current risk algorithms mean that these patients will continue to be determined largely at the discretion of treating clinicians. Technical advances, such as entirely subcutaneous ICD systems,30 might help to reduce implant complications and thus shift the balance in favour of ICD therapy in borderline cases. In the long term the best solution will be the development of a clinical risk predictor analogous to those used in other diseases such as atrial fibrillation31 and coronary artery disease32 that can generate individualised risk estimates that allow clinicians and patients to better understand the balance between disease and treatment-related risks. The development of such a tool will also empower patients and allow them to participate more actively in treatment decisions.
Limitations
We acknowledge that variance in the definitions of individual RF may introduce some bias into the comparison between the two guidelines. While the ACCF/AHA guidelines do not set an age limit, the ACC/ESC guidelines consider ABPRE a RF in those aged <50 years on the basis of a single study which reported a significant association between ABPRE in those <50 years and overall HCM-related mortality (but not specifically SCD).33 In the present study, like the majority of contemporary studies,3 ,10 ,11 a cut-off of ≤40 years was used based on previously published data that showed an association with SCD.9 When ABPRE was analysed as a RF using a cut-off of less than 50 years of age, the findings were similar (data not shown). When assessing unexplained syncope all events at or prior to first evaluation were used in keeping with the ACC/ESC guidelines. The ACCF/AHA guidelines suggest that recent unexplained syncope should be used as a RF, but do not explicitly set a time cut-off. A recent study examined syncope within 6 months as a RF of SCD in a multivariable analysis which did not include NSVT or ABPRE.34 Even though the study reported a significant association with SCD,34 the significance of this finding in the context of the current guidelines (which use NSVT and ABPRE as RF) is not known. Finally, FHSCD was defined as one or more SCD in relatives <40 years of age or SCD at any age in a relative with confirmed HCM. This definition is keeping with both the 2003 ACC/ESC and 2011 ACCF/AHA guidelines. Previous studies have used variable definitions, and this reflects the lack of consensus in the published literature of what constitutes a significant FHSCD.3 ,10 ,11 ,35–41
Both the ACC/ESC and ACCF/AHA guidelines recommend the individualisation of treatment by considering other potential/emerging SCD risk modifiers such as late gadolinium enhancement on cardiac MRI. Unfortunately, the duration of this study means these data are not available for most of the cohort. However, since the publication of the 2011 ACCF/AHA guidelines, a meta-analysis has failed to show that late gadolinium enhancement is associated with SCD.42
This study examined the performance of the two SCD risk algorithms in the short to medium term but their long term accuracy remains unknown and needs to be examined in studies with longer follow-up periods. Even though data on some RF were missing in some patients, this reflects the application of the guidelines in routine clinical practice where the absence of a RF is considered as absence of risk. Finally, we cannot exclude an effect of drug treatment or septal reduction therapy43 on the incidence of SCD.
Conclusions
The 2003 ACC/ESC and the 2011 ACCF/AHA guidelines distinguish high from low risk individuals with limited power. The risk of SCD increases with the aggregation of RF. ICD implantation is reasonable in patients with multiple RF but the majority of patients treated with an ICD based on contemporary guidelines do not suffer SCD in the short to medium term.
References
Footnotes
-
Contributors CO'M designed the study, collected and interpreted the data, carried out the statistical analysis and wrote the manuscript. MT-E, AP, DL and SD collected and/or interpreted the data, and contributed to the writing of the manuscript. PE was involved in the design of the study, interpretation of data and writing of the manuscript. WM was involved in the drafting of the manuscript and revising it critically for important intellectual content. CO'M and PE are responsible for the overall content and take responsibility for the final submission.
-
Funding This work was undertaken at the University College London Hospitals/University College London who received a proportion of funding from the Department of Health's National Institute for Health Research Biomedical Research Centres funding scheme.
-
Competing interests None.
-
Ethics approval Ethics approval not required under NHS research governance arrangements.
-
Provenance and peer review Not commissioned; internally peer reviewed.