Article Text

Abstract
Objective To examine the association between chronic immune-mediated diseases (rheumatoid arthritis, systemic lupus erythematosus or the following chronic immune-mediated inflammatory diagnoses groups: inflammatory bowel diseases, inflammatory polyarthropathies, systemic connective tissue disorders and spondylopathies) and the 6-year coronary artery disease, stroke, cardiovascular disease incidence and overall mortality; and to estimate the population attributable fractions for all four end-points for each chronic immune-mediated inflammatory disease.
Methods Cohort study of individuals aged 35–85 years, with no history of cardiovascular disease from Catalonia (Spain). The coded diagnoses of chronic immune-mediated diseases and cardiovascular diseases were ascertained and registered using validated codes, and date of death was obtained from administrative data. Cox regression models for each outcome according to exposure were fitted to estimate HRs in two models1: after adjustment for sex, age, cardiovascular risk factors and2 further adjusted for drug use. Population attributable fractions were estimated for each exposure.
Results Data were collected from 991 546 participants. The risk of cardiovascular disease was increased in systemic connective tissue disorders (model 1: HR=1.38 (95% CI 1.21 to 1.57) and model 2: HR=1.31 (95% CI 1.15 to 1.49)), rheumatoid arthritis (HR=1.43 (95% CI 1.26 to 1.62) and HR=1.31 (95% CI 1.15 to 1.49)) and inflammatory bowel diseases (HR=1.18 (95% CI 1.06 to 1.32) and HR=1.12 (95% CI 1.01 to 1.25)). The effect of anti-inflammatory treatment was significant in all instances (HR=1.50 (95% CI 1.24 to 1.81); HR=1.47 (95% CI 1.23 to 1.75); HR=1.43 (95% CI 1.19 to 1.73), respectively). The population attributable fractions for all three disorders were 13.4%, 15.7% and 10.7%, respectively.
Conclusion Systemic connective tissue disorders and rheumatoid arthritis conferred the highest cardiovascular risk and population impact, followed by inflammatory bowel diseases.
- Cardiovascular disease
- Inflammation
- Arthritis
- Connective Tissue Diseases
- Inflammatory Bowel Diseases
- Spondyloarthritis
Statistics from Altmetric.com
- Cardiovascular disease
- Inflammation
- Arthritis
- Connective Tissue Diseases
- Inflammatory Bowel Diseases
- Spondyloarthritis
Introduction
The primary prevention of cardiovascular diseases (CVD) is a paramount priority of the public health agenda because it is the main cause of death in the developed world and is increasing in developing countries.1 The common basis of CVD is atherosclerosis, an inflammatory degenerative process present throughout a person’s lifetime.2 The pathogenesis of CVD in patients with chronic immune-mediated inflammatory diseases (CIID) is multifactorial and is thought to result from an interaction of inflammation, metabolic factors, therapy and disease-related factors.3
Individuals diagnosed with inflammatory bowel diseases,4 rheumatoid arthritis,5 systemic lupus erythematosus (SLE),6 systemic sclerosis7 or ankylosing spondylitis8 have shown an increased CVD risk. However, straightforward comparison of the studies is difficult owing to the different inclusion criteria used. Better understanding of the association between these conditions and cardiovascular morbidities can help in early assessment and management of risk factors and may help improve long-term outcomes in patients with CIID.
The objectives of the study were: (1) to ascertain whether 6-year risk of coronary artery disease, stroke, CVD incidence and overall mortality is associated with the diagnosis of rheumatoid arthritis, SLE or the following CIID diagnoses groups: inflammatory bowel diseases, inflammatory polyarthropathies, systemic connective tissue disorders and spondylopathies; and (2) to estimate the population-based burden of coronary artery disease, stroke, CVD and mortality attributable to each of the studied CIID.
Methods
Data sources
The System for the Development of Research in Primary Care (SIDIAP) is an electronic medical records database derived from general practices of the Catalan Institute of Health in Catalonia (Spain). Data on approximately 5.8 million patients are recorded by general practitioners as part of patients’ clinical records. Since approximately 80% of the population is registered with a general practitioner of the Catalan Institute of Health, SIDIAP is considered representative of the population in Catalonia.9 The International Classification of Diseases 10th Edition (ICD-10) is used to code diagnoses and the Anatomical Therapeutic Chemical Classification System is used for the classification of drugs. SIDIAP is also linked with hospital admissions data.
SIDIAPQ is the subsample of individuals assigned to the 40% of general practitioners periodically selected to provide researchers with the best quality registry data and has been validated for the study of the epidemiology of CVD. The methodology for selecting this subsample has been explained elsewhere.9 The present study was approved by the local ethics committees.
Study design
We conducted a cohort study of individuals included in SIDIAPQ. The inclusion period spanned 1 January 2007 through 31 December 2012. Participants were 35–85 years old and those who had a record documenting a prior history of myocardial infarction, angina, stroke, transient ischaemic attack, intermittent claudication or coronary revascularisation procedures prior to the inclusion were excluded. Patients were followed up until they experienced the outcomes of interest, died, left the SIDIAPQ database (eg, change of address) or the follow-up ended (31 December 2012), whichever came first.
Definition of CIID
A prespecified list of ICD-10 codes, set a priori and based on previous work in the field,10 11 was used to screen SIDIAPQ records in order to identify all patients with CIID and classify them in four groups: (1) inflammatory bowel disease, (2) inflammatory polyarthropathies, (3) systemic connective tissue disorders and (4) spondylopathies (see the disorders included in each group in online supplementary table 1). In addition, a complementary analysis was performed for the most prevalent single diagnoses: (5) rheumatoid arthritis and (6) SLE. We included individuals without a registered diagnosis who required a continued prescription for a medication that would normally be used to treat inflammatory bowel disease, rheumatoid arthritis or SLE, based on evidence-based recommendations.12–15 If an individual presented with more than two diagnoses, we considered the oldest one for the purpose of this analysis. Individuals who developed CIID during follow-up were considered non-exposed. Since the CIIDs considered in this study have physical features, adverse prognosis and the database has been previously validated1011 diagnoses are expected to be accurately recorded.
Supplementary file 1
Identification of outcomes
The end-points considered were: (1) coronary artery disease: incident myocardial infarction or angina; (2) incident stroke; (3) CVD: coronary artery disease or stroke; and (4) all-cause mortality (online supplementary table 2). All end-points were identified from the SIDIAP and Hospital Discharge registries. The methodology for case finding used in the SIDIAP database has shown high validity and good representativeness of the population for use in epidemiological studies of CVD.9
Assessment of covariates
Data were obtained from electronic records on sex, age, systolic and diastolic blood pressures, glucose, triglycerides, total, high-density lipoprotein (HDL) and low-density lipoprotein (LDL) cholesterol, glycaemia, weight and height at baseline. Presence of cardiovascular risk factors was based on the presence of relevant codes with a date prior to the inclusion of each participant: (1) diabetes mellitus: ICD-10 categories E11, E12, E14, and subcategories thereof; (2) hypertension: ICD-10 categories I10, I15, and subcategories thereof; (3) hypercholesterolaemia: ICD-10 category E78 and its subcategories, except for E78.3 and E78.6; (4) smoking: ICD-10 category F17 for smokers or Z72.0 for ex-smokers; and (5) obesity: ICD-10 category E66 and subcategories except for E66.1 and E66.2.9 Coronary artery disease risk was estimated in participants aged 35–74 years with the Framingham-REGICOR function validated for the Spanish population.16 Participants were categorised into three treatment groups: disease-modifying antirheumatic drugs (DMARD) including biological therapies, anti-inflammatory drugs (ie, non-steroidal anti-inflammatory drugs (NSAID), glucocorticoids, other non-inflammatory drugs) and non-users of DMARD and anti-inflammatory drugs. Lipid-lowering and antihypertensive treatments were also considered. The drugs included in each group are summarised in online supplementary tables 3–5.
Statistical analysis
We used 10 multiple imputations by chained equations17 to replace missing baseline values for cholesterol (total, HDL, LDL), triglycerides, glycaemia, systolic and diastolic blood pressures, height, weight and MEDEA index (a deprivation index designed to capture sex-related inequalities). In addition to incorporating the missing-at-random assumption, we compared case-complete results alone with the multiple imputations as a sensitivity analysis.
Continuous variables were summarised as mean (SD) or median (IQR) when their distribution departed from normal, and categorical variables as proportions. The incidence of coronary artery disease, stroke and CVD events and overall mortality was estimated. We plotted the Kaplan-Meier curves for all four end-points by CIID diagnoses and in population with no CIID and we performed log-rank tests to estimate the differences between each diagnosis and CIID-free individuals. Bonferroni correction for multiple comparisons was applied, considering as significant a p-value <0.002.
To assess the association between the CIID diagnoses and the 6-year incidence of coronary artery disease, stroke and CVD events or death, we adjusted two Cox regression models for each outcome. The first was adjusted for sex, age, systolic and diastolic blood pressures, total and HDL cholesterol, diabetes and smoking. The second was further adjusted for lipid-lowering, antihypertensive and rheumatic-specific drug use divided in three categories. The proportionality assumption was tested for all models (online supplementary table 6). To test the robustness of case definition, we performed several sensitivity analyses. In the first, we excluded patients with no record of a diagnosis but who required continued prescription of a medication normally used to treat inflammatory bowel disease, rheumatoid arthritis or SLE, based on evidence-based recommendations. The second sensitivity analysis excluded those individuals who were receiving anti-inflammatory treatment (NSAIDs or DMARDs) before the CIID diagnosis. The third excluded those individuals with chronic diseases that may be related with both inflammation and cardiovascular risk (eg, chronic kidney disease, sleep disorders and liver disease). The fourth excluded those individuals with a CVD diagnosis in the 12 months after the study start date to minimise the possibility of prevalent CVD. Also, as a sensitivity analysis, model 2 was adjusted using the Fine and Gray method for coronary artery disease, stroke and CVD outcomes and considering death as a competing event.
Finally, to estimate the burden of CVD and mortality attributable to each CIID, the population attributable fractions (PAF) were estimated for all four end-points using Levin’s formula. We used the adjusted HR according to model 2 and the prevalence of every CIID diagnosis observed in our cohort.
All calculations were made with R statistical package (V.3.3.3; R Foundation for Statistical Computing, Vienna, Austria).
Results
We included 991 546 individuals in our analysis, 467 494 (47.1%) men, mean age 53 years (SD=13). Inflammatory polyarthropathies were the most prevalent CIID diagnosis (2.3%), followed by inflammatory bowel diseases (1.0%), systemic connective tissue disorders (0.5%) and spondylopathies (0.2%) (figure 1). Additionally, 5552 (0.6%) presented with rheumatoid arthritis and 664 (0.07%) with SLE. Individuals with CIID were older, and more often presented with diabetes, hypertension, dyslipidaemia and higher 10-year cardiovascular risk than those without CIID. Finally, the individuals with CIID were more frequently on treatment with statins, aspirin and DMARDs (table 1).

Participants’ flow chart. CAD, coronary artery disease; CIID, chronic immune-mediated inflammatory disease; CVD, cardiovascular disease.
Baseline characteristics of participants according to diagnosis of CIID
Annual incidence rates for all end-points showed significantly higher rates in those diagnosed with CIID (table 2). Additionally, the Kaplan-Meier curves showed significantly lower disease-free time (ie, coronary artery disease, cerebrovascular diseases and CVD) and survival for all CIID diagnoses compared with CIID-free population, except for SLE and spondylopathies. Indeed, the latter only presented with higher risk for death (figure 2).
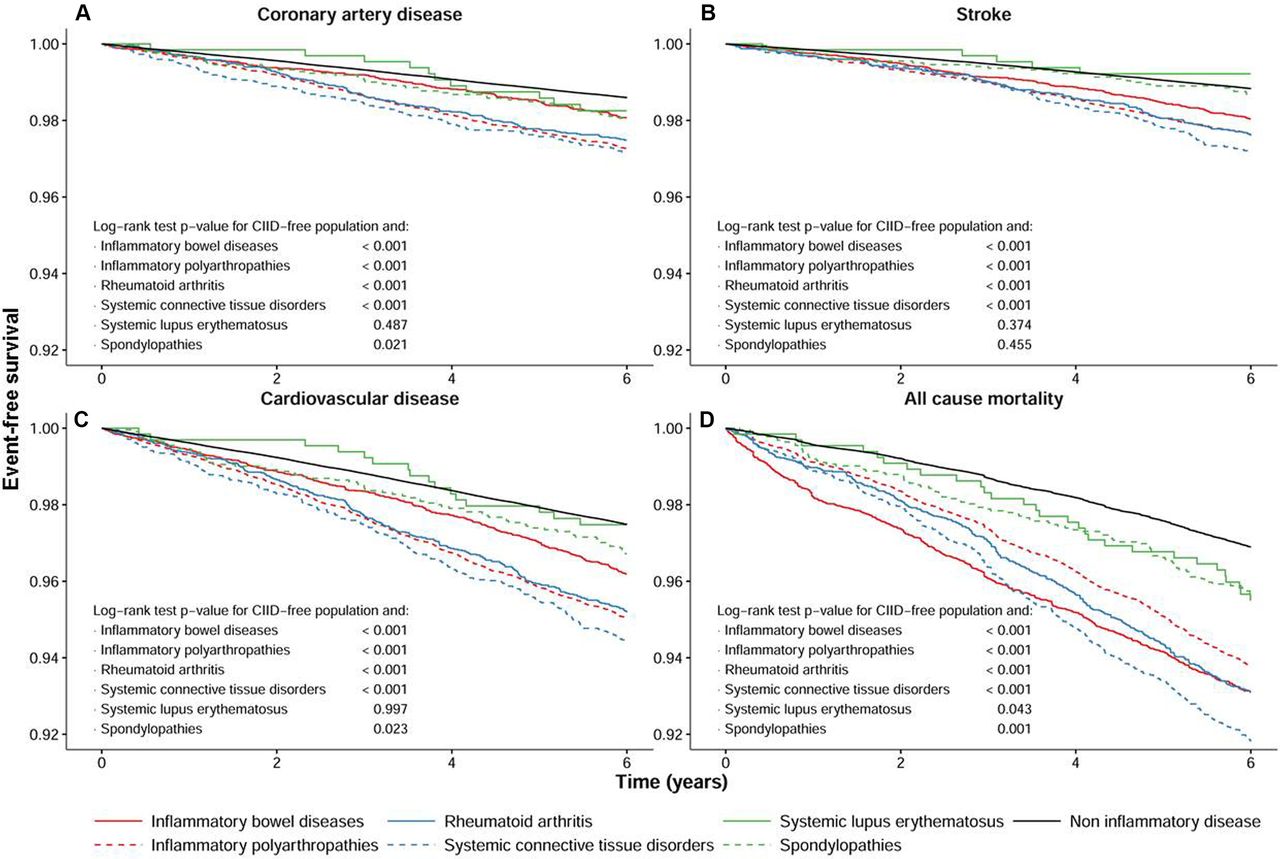
Survival curves for 6-year incidence of coronary artery disease (A), stroke (B), cardiovascular disease (C) and overall mortality (D) according to CIID diagnoses and in CIID-free population. Log-rank test p values have been computed for each CIID diagnosis and CIID-free individuals. CIID, chronic immune-mediated inflammatory disease.
Annual incidence rates for cardiovascular end-points and overall mortality according to different CIID diagnoses per 1000 person-years (95% CI) compared with the general population
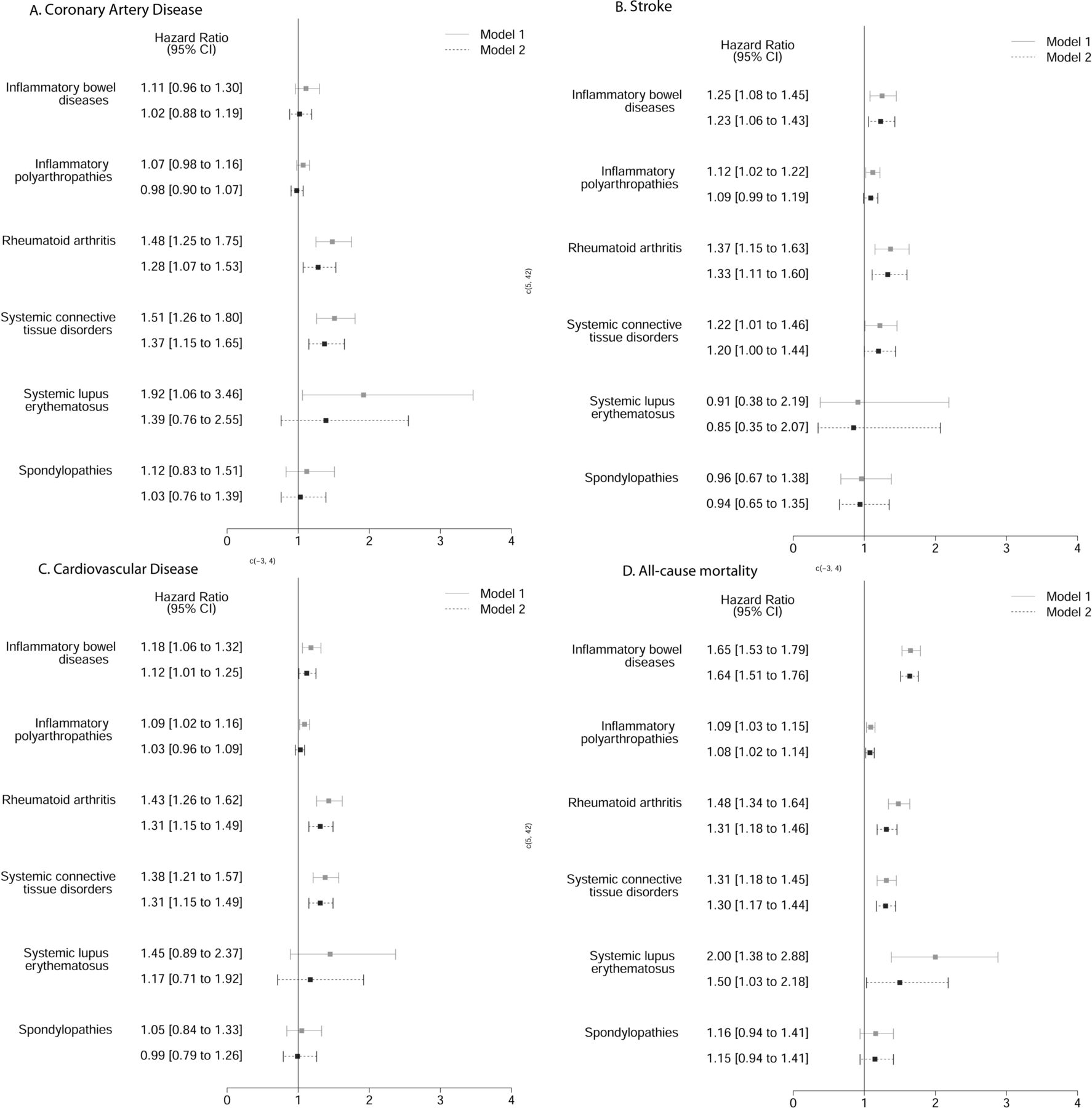
The multivariable models showed that systemic connective tissue disorders and rheumatoid arthritis increased the risk of all end-points considered, particularly coronary artery disease for the first (HR=1.37 (95% CI 1.15 to 1.65)) and stroke for the latter (HR=1.33 (95% CI 1.11 to 1.60)). Among individuals with SLE, only the risk of mortality was significantly higher (HR=1.50 (95% CI 1.03–2.18)), even though the group in which this disease is included (ie, systemic connective tissue disorders) conferred an increased risk for all end-points. On the other hand, the group of inflammatory polyarthropathies only showed a marginally significant association with stroke (HR=1.09 (95% CI 0.99 to 1.19)). Finally, inflammatory bowel diseases had a significant association with stroke and with overall mortality (HR=1.23 (95% CI 1.06 to 1.43) and HR=1.64 (95% CI 1.51 to 1.76), respectively). The association between inflammatory bowel diseases and overall mortality did not meet the proportionality assumption. We stratified the follow-up in three periods: (0–1 year), (1–4 years), (>4 years), and the proportionality assumption was met. The HRs were 2.9 (95% CI 2.49 to 3.39), 1.60 (95% CI 1.42 to 1.80) and 1.22 (95% CI 1.06 to 1.41), respectively (figure 3). No significant differences were found between the main analysis and any sensitivity analysis performed (online supplementary tables 7–13).
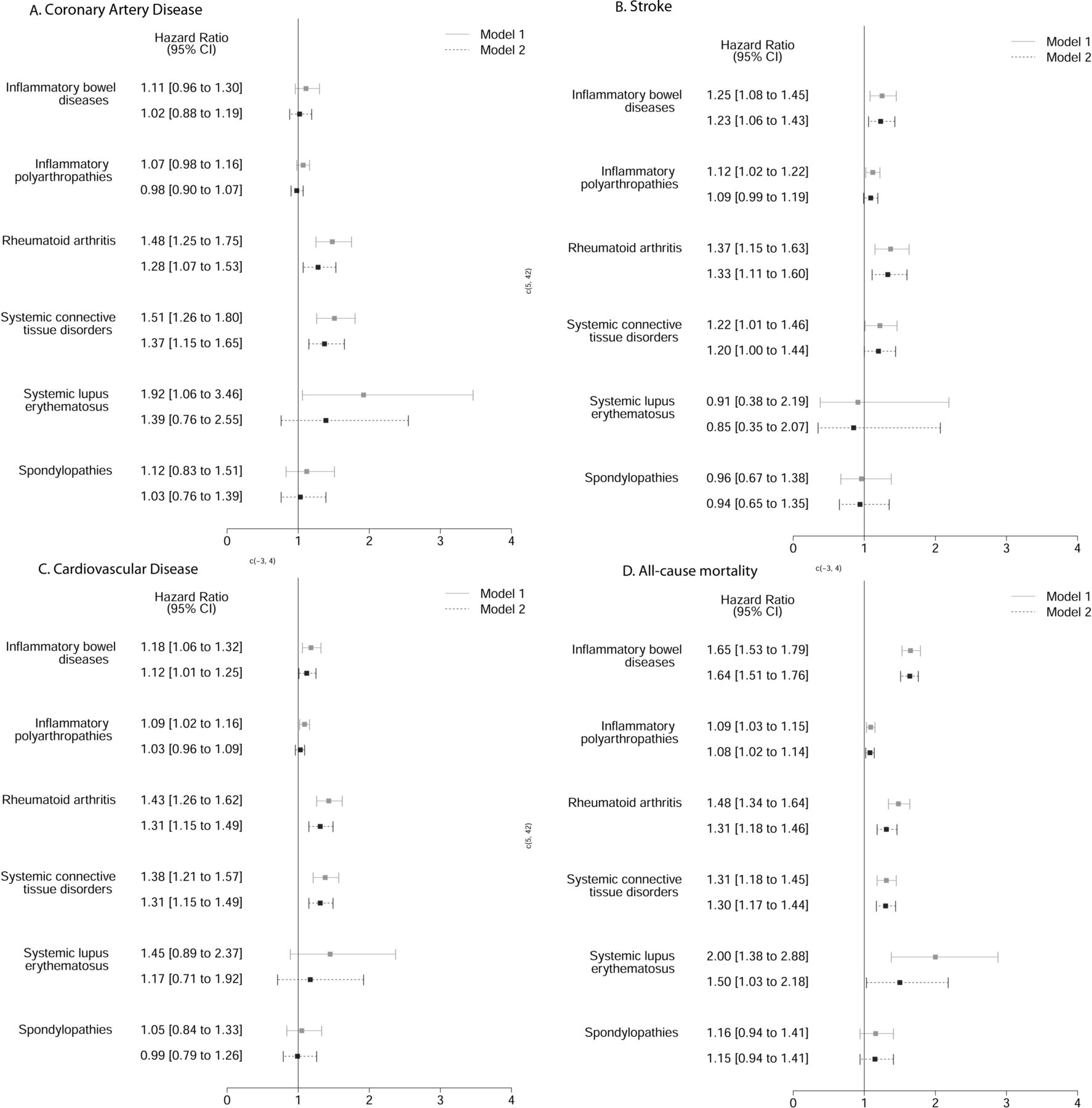
HRs for 6-year incidence of coronary artery disease (A), stroke (B), cardiovascular disease (C) and overall mortality (D) among participants with CIID diagnosis compared with those without CIID. Model 1 has been adjusted by age, sex, smoking status, total cholesterol, high-density lipoprotein cholesterol, systolic blood pressure and diastolic blood pressure. Model 2 has been further adjusted for statins, hypertensive drugs and three categories of exposure to antirheumatic-specific treatments: disease-modifying antirheumatic drugs, other anti-inflammatory drugs, no exposure. CIID, chronic immune-mediated inflammatory disease.
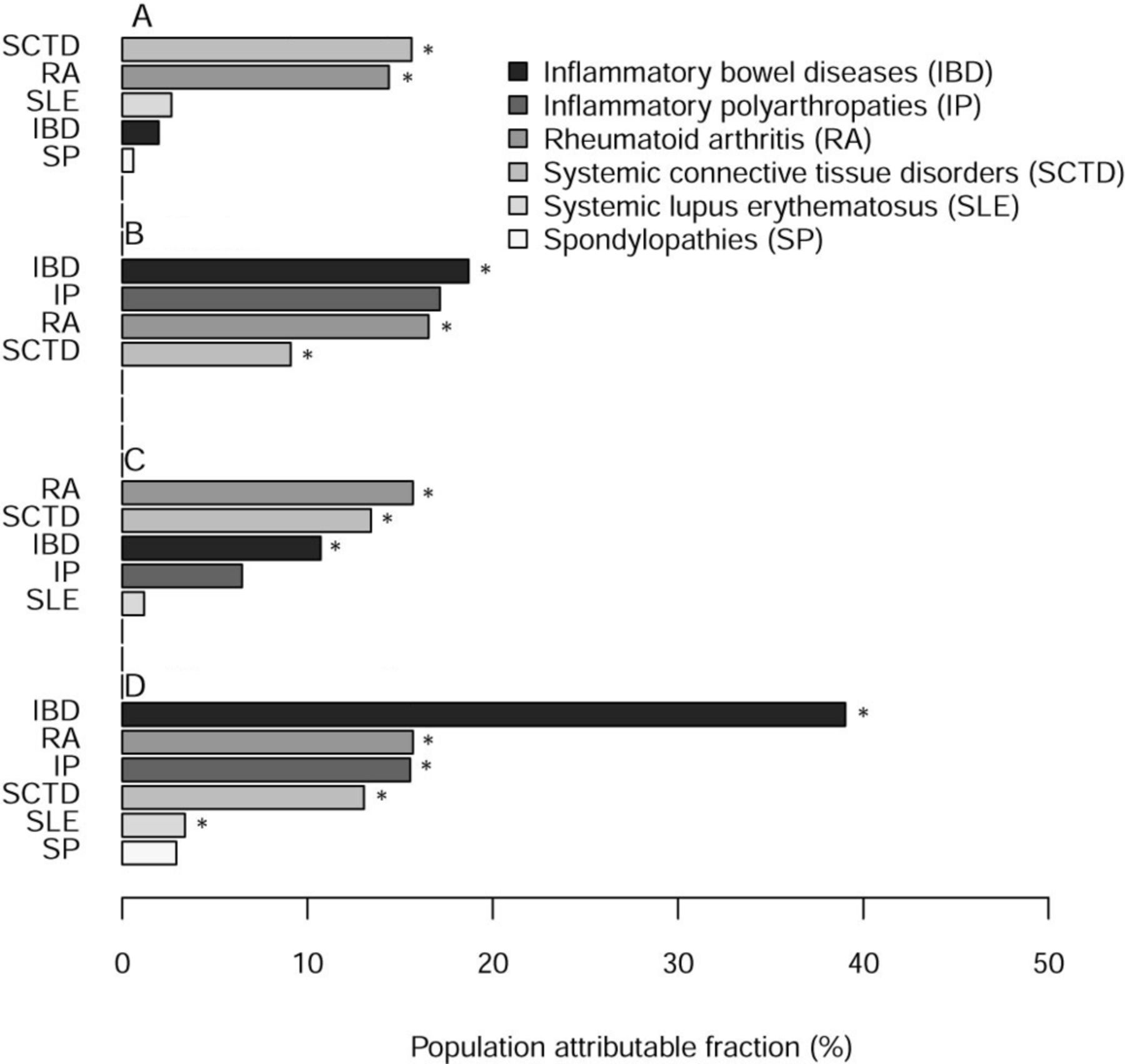
The CIIDs with significant population impact on coronary artery disease, stroke and CVD were systemic connective tissue disorders (15.6%, 9.1% and 13.4%, respectively) and rheumatoid arthritis (14.4%, 16.5% and 15.7%, respectively). In addition, inflammatory bowel diseases presented significant PAF for stroke (18.7%) and for CVD (10.7%). Finally, the population impact on overall mortality was significant for all CIIDs, except for the spondylopathies, although the magnitude ranged from 39.0% for inflammatory bowel diseases to 3.4% for SLE (figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Population attributable fraction for 6-year incidence of coronary artery disease (A), stroke (B), cardiovascular disease (C) and overall mortality (D) for different chronic immune-mediated diseases. Bars are ordered according to the magnitude of the population attributable fraction for each group of chronic immune-mediated disease diagnoses.
Discussion
Diagnoses of CIID conferred an increased risk of CVD and overall mortality in this cohort study. This risk was particularly pronounced in individuals diagnosed with systemic connective tissue disorders and rheumatoid arthritis. Overall mortality risk was increased in both groups of diseases. This greater risk was not explained by ageing, the higher prevalence of cardiovascular risk factors observed in CIID individuals, nor by the use of DMARDs and anti-inflammatory drugs, which may have a role in the modulation of cardiovascular risk. Indeed, the differences in the estimated cardiovascular risk did not reflect higher incidence in individuals with CIID compared with those without, pointing out the effect of other variables not included in such estimates. Additionally, inflammatory bowel diseases raised the risk of stroke and the overall mortality risk.
Risk of CVD in CIID
Individuals with CIID were older and had a worse cardiovascular risk factor profile; however, the multivariable analysis adjusted for the relevant variables showed an added risk not explained by these cardiovascular risk-related variables. A previous study, which also analysed data from electronic medical records, showed similar coronary artery disease and stroke incidence in individuals with systemic connective disorders, inflammatory polyarthropathies and inflammatory bowel diseases.18 Additionally, we performed the same analysis separately for rheumatoid arthritis and for SLE, the most prevalent diseases within both groups, and therefore the most reported in the literature. As previously described, rheumatoid arthritis showed a significant risk in all four end-points, even after adjustment for drug therapy.19 Lazzerini et al pointed out that a higher risk of rhythm disturbances, particularly tachyarrhythmias, in such individuals may significantly contribute to the high cardiovascular morbidity and mortality.20 SLE only showed a significant association with overall mortality. The systematic review by Schoenfeld et al showed that SLE at least doubled cardiovascular risk; however, the authors also pointed out the discrepancies found within the literature.21 Concurring with Andersohn et al, individuals with inflammatory bowel diseases presented higher risk of stroke.22 On the other hand, the association between these diseases and coronary artery disease has not been totally clarified. Similar to previous reports, we did not find an increased risk of coronary artery disease in these individuals18; however, this association was significant in the analysis of a nationwide, population-based Danish cohort.23 Finally, individuals with spondylopathies did not present with significantly higher risk for any of the end-points analysed.
Prevention of CVD in CIID
The most used treatments for controlling CIID, and particularly rheumatoid arthritis, the most thoroughly described, may have antagonistic effects on cardiovascular risk. The DMARD drugs may confer a cardioprotective effect mostly attributed to the inhibition of systemic inflammation.24 However, Aviña-Zubieta et al described a dual effect of glucocorticoids on myocardial infarction risk in individuals with rheumatoid arthritis: an immediate effect mediated through current dosage and a long-term effect of cumulative exposure.25 In addition, del Rincón et al pointed out that daily doses higher than 8 mg were associated with higher cardiovascular and overall mortality in such individuals.26 Recently, O’Neill et al showed in a randomised clinical trial the beneficial effect of certain anti-inflammatory treatments that modulate the tumour necrosis factor-α pathway (eg, methotrexate + infliximab), to restore the beneficial effects of HDL on the vasculature.27
To minimise the confounder effect of such variables, model 2 of the present analysis was adjusted for drug use, divided in three categories (DMARDs, anti-inflammatory drugs and non-DMARD non-anti-inflammatory drugs). Indeed, further pharmacoepidemiology studies are needed to ascertain the effect of antirheumatic treatments in all CIID diagnoses.
A reduction in the number of individuals diagnosed with systemic connective tissue disorders and rheumatoid arthritis may have a moderate population impact on preventing coronary artery disease, stroke and CVD. However, the diagnosis of such CIIDs together with an adverse cardiovascular profile may have an additive effect on the risk of coronary artery disease and CVD. The most recent European League Against Rheumatism guideline promotes a proactive management of cardiovascular risk in individuals with inflammatory polyarthritis and spondylopathies. The objective is to control systemic inflammation and cardiovascular risk factors.28 These recommendations have also been proposed for individuals with SLE29 but could probably be extended to individuals with any systemic connective tissue disorder. In addition, the development of new tools for the prediction of cardiovascular events, which could incorporate CIID activity biomarkers, may help reduce the incidence of such events.24 ,30
Characteristics and limitations of the study
The results of our study confirm the high cardiovascular risk conferred by previous studies exploring CIID incidence with lower sample sizes.4 6–8 22 However, some biases inherent to the observational design of the study should be considered. First, reverse causality is not likely to be present in our study because the design meets the temporality criteria and the individuals with a history of CVD were excluded at recruitment. In addition, the results of the sensitivity analysis excluding those who presented with a CVD event within the first 12 months of follow-up did not differ from the main analysis. To avoid misclassification bias, we used the medical diagnosis of CIID extracted from SIDIAP, a primary care database. Although this source of data may contain under-reporting, the validity of SIDIAP coding for ICD-10 diagnosis of cardiovascular and rheumatic diseases has been documented.10 11 Indeed, the results of the sensitivity analyses confirmed the robustness of the case definition. In addition, the representativeness of data ensures the generalisability of the results. The covariates of the present analysis had missing values (ranging from 9% to 78%) that could influence the results. To avoid selection bias, wherever the population with missing data differed from those with complete data, we imputed the missing values for continuous variables instead of excluding records with missing data. The appropriateness of performing multiple imputations depends on the percentage and mechanism of missing values and on the number of complete observations used in the imputation process. In our study, 218 140 complete cases were available to impute variables with missing values. Exposure variables (ie, CIID diagnoses) and outcomes had no missing values. We selected the two most frequent single CIID diagnoses (rheumatoid arthritis and SLE) in the population and in the literature for analysis. In addition, we provided broad definitions of CIID diagnosis (ie, inflammatory bowel diseases, inflammatory polyarthropathies, systemic connective tissue disorders and spondylopathies). This approach, proposed by Dregan et al, allowed for comparison of results.18 The present analysis did not consider variables such as severity or elapsed time between CIID diagnosis and the incidence of cardiovascular events or death. The use of broad CIID definitions may complicate the use of such variables due to the number and heterogeneity of the diseases included in each group. Finally, to minimise confounding by indication bias, all our analyses were adjusted for any medication with potential effects on inflammation and cardiovascular risk (DMARDs, antihypertensive treatments and statins). Despite all our efforts, however, residual confounding is likely to exist. Thus, pharmacoepidemiology studies considering each CIID’s specific variables are needed to ascertain the best way to prevent CVD in such individuals.
Conclusion
Systemic connective tissue disorders and rheumatoid arthritis were the CIID diagnoses with the highest 6-year risk of coronary artery disease or any cardiovascular event and the greatest population impact. Diagnosis of inflammatory bowel diseases (ie, ulcerative colitis and Crohn’s disease) conferred a significant risk and PAF for stroke. Regarding overall mortality, all CIID diagnoses except spondylopathies increased 6-year mortality.
Key messages
What is already known on this subject?
Individuals diagnosed with chronic immune-mediated inflammatory diseases (CIID) present with increased cardiovascular disease risk.
There are no comparable indicators to ascertain the cardiovascular risk associated with each CIID due to the different inclusion criteria used in previous publications.
What might this study add?
Cardiovascular events and overall mortality risk were particularly pronounced in individuals diagnosed with systemic connective tissue disorders (HR=1.31 (95% CI 1.15 to 1.49) and HR=1.30 (95% CI 1.17 to 1.44), respectively) and rheumatoid arthritis (HR=1.31 (95% CI 1.15 to 1.49) and HR=1.31 (95% CI 1.18 to 1.46), respectively). This risk was not explained by the higher prevalence of cardiovascular risk factors, nor by the use of DMARDs and anti-inflammatory drugs.
How might this impact on clinical practice?
The development of new tools for the prediction of cardiovascular events, which could incorporate CIID activity biomarkers, may help reduce the incidence of such events.
Acknowledgments
The authors are grateful to the System for the Development of Research in Primary Care (SIDIAP) database and to Dr Albert Escola Campabadal for the expert review on chronic immune-mediated inflammatory disorders, and also appreciate the revision of the English text by Elaine Lilly, PhD.
References
Footnotes
Contributors JMBD, MGG, MCC, RR and MG conceived and designed the study. JMBD, MGG, MCC, RR, DPA, RE and MG acquired, analysed and interpreted the data. JMBD, BSG, IRD and MG drafted the manuscript. MGG, MCC and JP carried out the statistical analysis. JMBD and MG supervised the study. MG had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Funding This work has been supported by grants from the Instituto de Salud Carlos III FEDER (CP12/03287; HERACLES RD12/0042; RedIAPP RD12/0005), AGAUR (2014 SGR 240). IRD was funded by the RECERCAIXA Program, ObraSocial ‘La Caixa’ (RE087465).
Competing interests None declared.
Patient consent This manuscript is based on electronic medical records review.
Ethics approval CEIC PSMAR.
Provenance and peer review Not commissioned; externally peer reviewed.