Article Text

Abstract
Objective Data describing clinical relevance of chronic total occlusion (CTO) identified by coronary CT angiography (CCTA) have not been reported to date. We investigated the prognosis of CTO on CCTA.
Methods We identified 22 828 patients without prior known coronary artery disease (CAD), who were followed for a median of 26 months. Based on CCTA, coronary lesions were graded as normal (no atherosclerosis), non-obstructive (1%–49%), moderate-to-severe (50%–99%) or totally occluded (100%). All-cause mortality, and major adverse cardiac events defined as mortality, non-fatal myocardial infarction and late coronary revascularisation (≥90 days after CCTA) were assessed.
Results The distribution of patients with normal coronaries, non-obstructive CAD, moderate-to-severe CAD and CTO was 10 034 (44%), 7965 (34.9%), 4598 (20.1%) and 231 (1%), respectively. The mortality rate per 1000 person-years of CTO patients was non-significantly different from patients with moderate-to-severe CAD (22.95; 95% CI 12.71 to 41.45 vs 14.46; 95% CI 12.34 to 16.94; p=0.163), and significantly higher than of those with normal coronaries and non-obstructive CAD (p<0.001 for both). Among 14 382 individuals with follow-up for the composite end point, patients with CTO had a higher rate of events than those with moderate-to-severe CAD (106.56; 95% CI 76.51 to 148.42 vs 65.45; 95% CI 58.01 to 73.84, p=0.009). This difference was primarily driven by an increase in late revascularisations in CTO patients (27 of 35 events). After multivariable adjustment, compared with individuals with normal coronaries, the presence of CTO conferred the highest risk for adverse cardiac events (14.54; 95% CI 9.11 to 23.20, p<0.001).
Conclusions The detection of CTO on non-invasive CCTA is associated with increased rate of late revascularisation but similar 2-year mortality as compared with moderate-to-severe CAD.
Trial registration number NCT01443637.
- cardiac computer tomographic (ct) imaging
- heart disease
Statistics from Altmetric.com
Introduction
Chronic total occlusion (CTO) of a coronary artery can be found in 15%—30% of all patients referred for coronary angiography, and is associated with poor prognosis in the setting of stable coronary artery disease (CAD) and acute myocardial infarction.1–3 During the last decade, coronary CT angiography (CCTA) has shown good performance for diagnosis and prognosis of CAD,4 5 and has been increasingly used in the planning of CTO revascularisation.6 7
Recently, our group reported the non-negligible rate of CTO (6.2% in individuals with obstructive CAD defined as ≥50% stenosis) associated with a high burden of CAD risk factors among patients undergoing CCTA for suspected CAD.8 While the prognosis of CTO has been examined in the setting of percutaneous coronary intervention or myocardial infarction,2 3 there are no data describing the relevance of CTO when found incidentally at the time of CCTA. The aim of the current study was to assess the prognosis of CTO detected on CCTA among a large, international registry of patients without previous known CAD.
Methods
Study population
The COronary CT Angiography EvaluatioN For Clinical Outcomes: An InteRnational Multicenter (CONFIRM) registry is an international, multicentre, observational registry collecting clinical, procedural and follow-up data of patients who underwent ≥64 detector row CCTA between 2005 and 2010 at 17 centres in 7 countries (USA, Canada, Germany, Switzerland, Italy, Austria and South Korea). A detailed description of the study design has been published elsewhere.9 We included patients with suspected CAD, but without prior known CAD, defined as previous myocardial infarction and/or coronary revascularisation. We excluded patients with missing demographic, CAD or all-cause mortality follow-up data, and censored patients with early revascularisation (<90 days). All centres had institutional review board approval for patient enrolment including follow-up procedures.
The CONFIRM registry employs a standardised data collection method to gather information about baseline cardiovascular risk factors, symptoms, detailed angiographic results and clinical outcomes.10 Pretest probability of CAD was defined using the Diamond-Forrester score,11 and symptom presentation was classified into typical chest pain, atypical chest pain, non-cardiac pain or asymptomatic.12
Image acquisition and analysis
CT image acquisition was performed using single-source or dual-source 64-slice scanners. Patient preparation, data acquisition and interpretations were performed in direct accordance with the Society of Cardiovascular CT guidelines as previously described.13 Dose reduction strategies including ECG-gated tube current modulation, reduced tube voltage, and prospective axial triggering were used whenever possible, with estimated radiation doses ranging from 3 to 18 mSv.
Reconstructed data were evaluated in a uniform fashion across all study sites by level III-qualified readers using all necessary postprocessing techniques to determine the presence of CAD. Coronary segments were scored visually for the presence and composition of coronary plaque and degree of luminal stenosis with a 16-segment American Heart Association coronary artery model.14 The proximal segments were defined as follows: left main, proximal and mid left anterior descending artery, proximal left circumflex and first obtuse marginal branch and proximal and mid-right coronary artery.5 Coronary lesions were graded as normal (no atherosclerosis), non-obstructive (1%–49% stenosis), moderate-to-severe (50%–99%) or totally occluded (100%) in epicardial coronary arteries of ≥2 mm in diameter.8 Coronary lesions with ≥50% luminal stenosis severity were defined as obstructive. CTO was defined as complete interruption of the contrast-enhanced lumen of the coronary artery with recurrence of luminal opacification distal to the occlusion site as assessed by multiplanar reconstructions by CCTA (see online supplementary figure I).7 Plaque composition was classified as non-calcified, mixed (partially calcified) or calcified.5 Per-vessel classification and calculation of segment-stenosis score are further mentioned in the online supplementary file.
Supplemental material
Follow-up and study outcomes
The primary end point was time to death from all causes. In patients with complete follow-up for major adverse cardiac events, a secondary composite end point of all-cause death, non-fatal myocardial infarction and late coronary revascularisations performed ≥90 days after CCTA (driven by disease worsening rather than the results of CCTA as previously demonstrated)5 was assessed. Ascertainment of study outcomes is described in the online supplementary file.
Statistical methods
Categorical variables are presented as counts with proportions and were assessed using Pearson’s Χ2 test or Fisher’s exact test for cell counts <6. Continuous variables are presented as mean ± SD when normally distributed, or median with interquartile range when non-normally distributed, and analysed using Student’s unpaired t-test or Mann-Whitney U test, as appropriate. Cumulative event-free rates of time to all-cause mortality, non-fatal myocardial infarction and late coronary revascularisation were calculated using the Kaplan-Meier method and compared with the log rank test. Both univariate and multivariate Cox proportional hazards models, adjusted for differences in age, gender, cardiovascular risk factors and symptoms were used. Additionally, the adjustment for segment-stenosis score (categorically entered as 0, 1, 2, 3, 4, 5, 6, 7 and 8+) was made in the online supplementary file. To account for potential within-site correlations that may have arisen from referral bias or limited pooling of data and outcomes, we treated each site as the shared frailty (aka random effect) in each Cox model. Model overfitting was carefully considered and the proportional hazards assumption was assessed in all analyses. Statistical significance was accepted for two-tailed p values <0.05. Calculations were performed using STATA V.14.1 (StataCorp, College Station, Texas, USA).
Results
Study population
Of a total of 27 125 adult patients from the CONFIRM registry, we excluded patients with known CAD (n=2350), congenital heart disease (n=111) and missing demographics or CAD severity (n=919). Of the remaining 23 745 patients, we excluded 137 patients with missing follow-up for all-cause death and censored 780 patients with early revascularisation, resulting in a final study sample of 22 828 individuals.
The distribution of patients with normal coronaries, non-obstructive CAD, moderate-to-severe CAD and CTO was 10 034 (44%), 7965 (34.9%), 4598 (20.1%) and 231 (1%), respectively. Detailed patient characteristics and CCTA results according to the presence or absence of CTO are shown in table 1. Patients with CTO were generally older, more often male and had a higher prevalence of CAD risk factors. Among 231 patients with CTO, the number of obstructive coronary vessels (≥50% stenosis) inclusive of CTO was single-vessel in 40.3% (93/231), two-vessel in 32.5% (75/231) and three-vessel or left main in 27.3% (63/231), respectively. The number of occluded vessels (100% stenosis) was single-vessel in 89.6% (207/231), two-vessel in 10% (23/231) and three-vessel or left main in 0.4% (1/231), respectively. In total, 256 vessels (112 right coronary arteries, 83 left anterior descending arteries, 61 left circumflex arteries) were occluded. The location of CTO was proximal in the majority of cases (67.2%). Most CTO had mixed plaque morphology (60.5%), followed by non-calcified CTO (24.3%) and calcified CTO (15.2%).
Baseline characteristics of the study population (n=22 828)
Follow-up and all-cause mortality
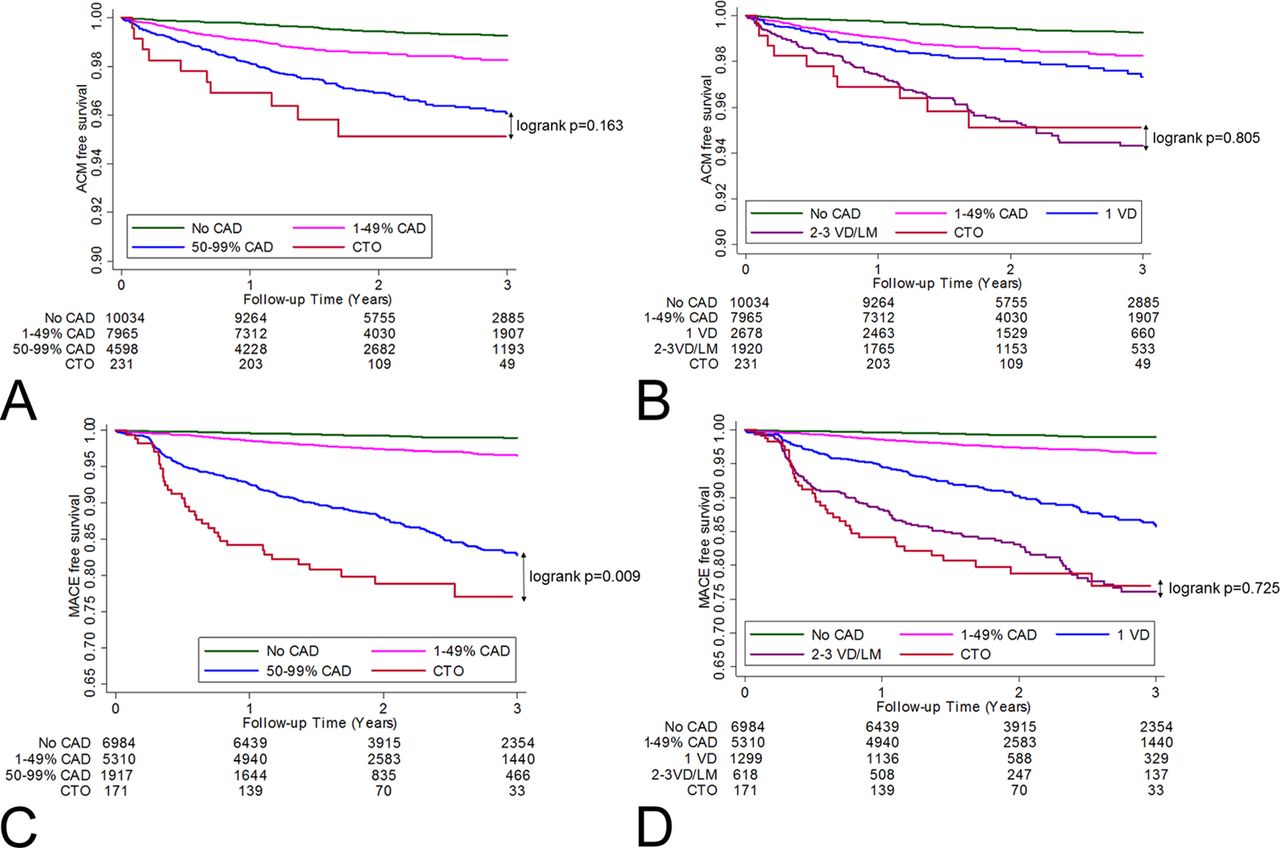
During the median follow-up of 26 months (25th to 75th percentile, 18–37 months), there were 339 deaths by any cause among 22 828 individuals, with an overall cumulative mortality rate of 6.46 (95% CI 5.81 to 7.19) per 1000 person-years. Specifically, whereas there was no evidence of difference in the mortality rate between CTO patients (22.95; 95% CI 12.71 to 41.45; 11 deaths) and patients with moderate-to-severe CAD (14.46; 95% CI 12.34 to 16.94; 153 deaths, log rank p=0.163), patients with CTO had significantly higher mortality than subjects without CAD (2.52; 95% CI 1.96 to 3.25; 60 deaths, log rank p<0.001) or with non-obstructive CAD (6.54; 95% CI 5.45 to 7.85; 115 deaths, log rank p<0.001) (figure 1A). When restricted to individuals with proximal CTO, there was a significant increase in the rate of all-cause mortality (31.01; 95% CI 16.69 to 57.64; 10 deaths) when compared with patients with moderate-to-severe CAD (log rank p=0.024) (figure 2A). In adjusted Cox proportional-hazards analysis, compared with patients without CAD, the presence of CTO and proximal CTO conferred the highest HRs for all-cause mortality by 2.65 (95% CI 1.32 to 5.28, p=0.006) and 3.73 (95% CI 1.81 to 7.66, p<0.001), respectively (table 2).
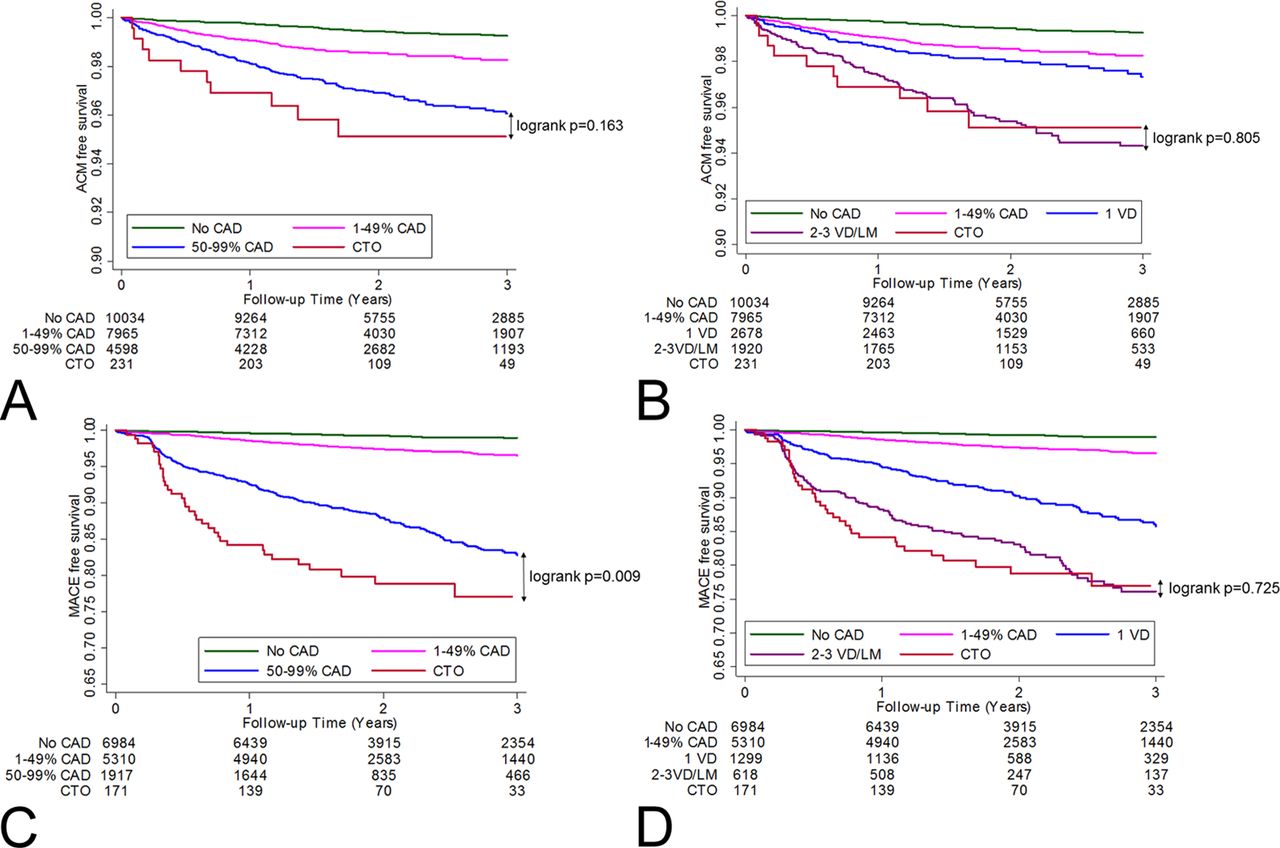
(A) ACM-free survival according to the severity of CAD and the presence or absence of CTO on CCTA. (B) ACM-free survival according to the extent of CAD and the presence or absence of CTO on CCTA. (C) Composite outcome of ACM, non-fatal myocardial infarction and late revascularisation-free survival according to the severity of CAD and the presence or absence of CTO on CCTA. (D) Composite outcome of ACM, non-fatal myocardial infarction and late revascularisation-free survival according to the extent of CAD and the presence or absence of CTO on CCTA. For the purpose of the per-vessel analysis, patients with one VD and multivessel or LM CAD had non-occlusive CAD. ACM, all-ause mortality; CAD, coronary artery disease; CCTA, coronary CT angiography; CTO, chronic total occlusion; LM, left main; MACE, major adverse cardiac events; VD, vessel disease.
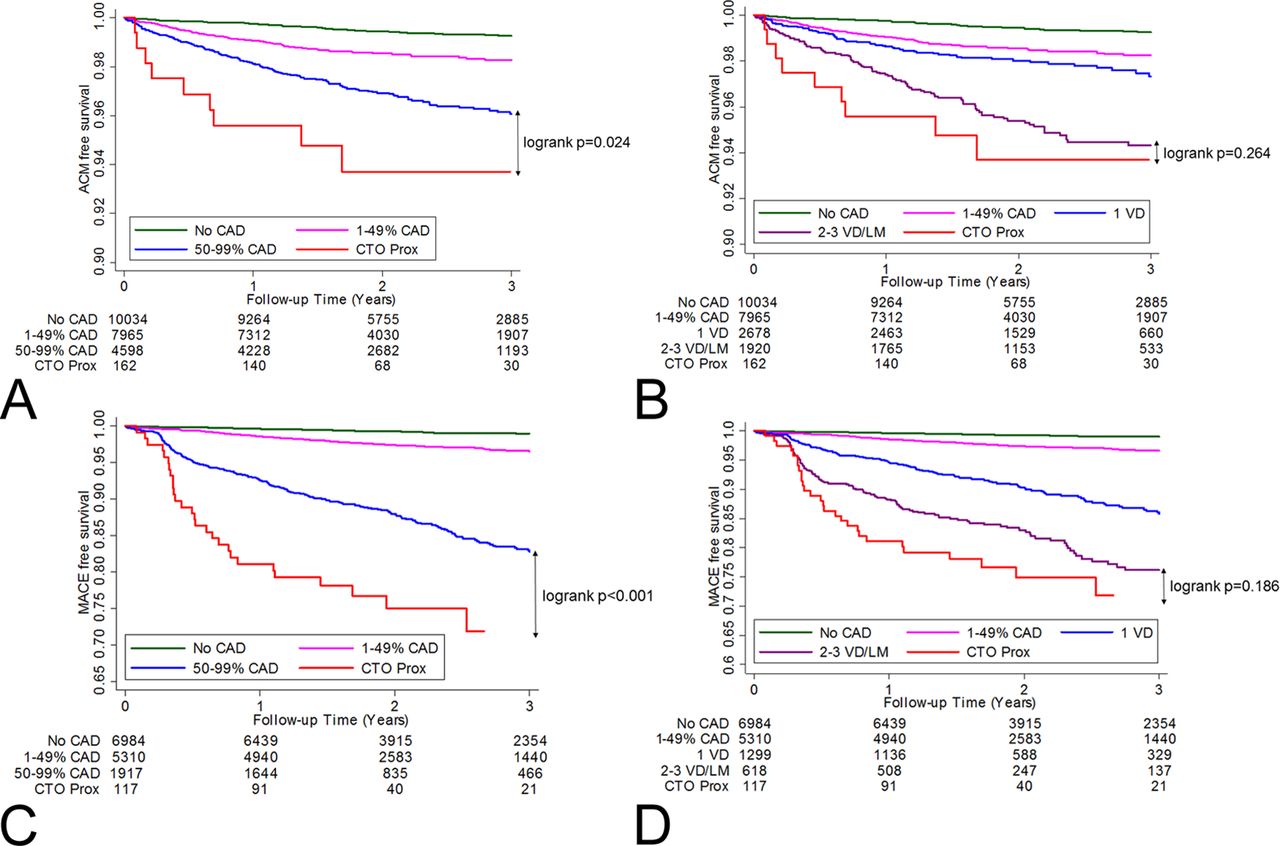
(A) ACM-free survival according to the severity of CAD and the presence or absence of proximal CTO on CCTA. (B) ACM-free survival according to the extent of CAD and the presence or absence of proximal CTO on CCTA. (C) Composite outcome of ACM, non-fatal myocardial infarction and late revascularisation-free survival according to the severity of CAD and the presence or absence of proximal CTO on CCTA. (D) Composite outcome of ACM, non-fatal myocardial infarction and late revascularisation-free survival according to the extent of CAD and the presence or absence of proximal CTO on CCTA. For the purpose of the per-vessel analysis, patients with one VD and multivessel or LM CAD had non-occlusive CAD. ACM, all-cause mortality; CAD, coronary artery disease; CCTA, coronary CT angiography; CTO, chronic total occlusion; LM, left main; MACE, major adverse cardiac events; VD, vessel disease.
HRs for all-cause death according to the severity and extent of obstructive CAD (n=22 828)
In the analysis stratified by the number of involved vessels (≥50% stenosis), there was no evidence of difference in the mortality rates of patients with CTO and with proximal CTO compared with patients with multivessel or left main CAD (figures 1B and 2B). In adjusted Cox proportional-hazards analyses, the relative hazards for death increased proportionally to CAD extent conferring the highest risk for proximal CTO and multivessel or left main CAD (table 2, online supplementary table I).
Major adverse cardiac events
Among 14 382 individuals with follow-up for the composite end point (1917 with moderate-to-severe CAD and 171 with CTO), 503 events (159 deaths, 105 non-fatal myocardial infarctions and 239 late revascularisations) occurred, with the overall cumulative adverse events rate per 1000 person-years of 15.08 (95% CI 13.82 to 16.46). Compared with patients with moderate-to-severe CAD (65.45; 95% CI 58.01 to 73.84; 264 events), both patients with CTO (106.56; 95% CI 76.51 to 148.42; 35 events, log rank p=0.009) and proximal CTO (132.09; 95% CI 91.20 to 191.30; 28 events, log rank p<0.001) showed a significantly higher rate of the composite end point (figures 1C and 2C).
Whereas there was no evidence of difference in the rate of major adverse cardiac events among patients with CTO and with proximal CTO compared with patients with multivessel or left main CAD, patients with CTO had a higher rate of major adverse cardiac events than those with one-vessel disease (figures 1D and 2D). After multivariable adjustment, the presence of CTO and proximal CTO conferred the highest risk for adverse cardiac events (table 3, online supplementary table II). This difference was primarily driven by an increase in late revascularisations (27 of 35 events) (figure 3, table 4).

{kind=link}
{kind=link}
{kind=link}
Composite outcome of all-cause mortality, non-fatal myocardial infarction and late coronary revascularisation stratified by the presence or absence of CTO and the extent and severity of CAD on CCTA. For the purpose of the per-vessel analysis, patients with one VD and multivessel or LM CAD had non-occlusive CAD. CAD, coronary artery disease; CCTA, coronary CT angiography; CTO, chronic total occlusion; LM, left main; MI, myocardial infarction; VD, vessel disease.
Hazard ratios for the composite outcome of all-cause mortality, non-fatal myocardial infarction and late revascularisation according to the severity and extent of obstructive CAD (n=14 382)
Composite outcome of all-cause mortality, non-fatal myocardial infarction and late revascularisation according to the severity and extent of obstructive CAD (n=14 382)
Patients with multivessel CAD
Although there was no significant difference in the rate of all-cause mortality in the subgroup of patients with multivessel or left main CAD with versus without CTO (33.5; 95% CI 17.45 to 64.46; 9 deaths vs 20.73; 95% CI 16.90 to 25.42; 92 deaths, log rank p=0.215) (online supplementary figure II), the rate of major adverse cardiac events among patients with multivessel or left main CAD and CTO (169.75; 95% CI 117.96 to 244.27; 29 events) was significantly higher than of those without CTO (96.99; 95% CI 81.04 to 116.07; 119 events, log rank p=0.017) (online supplementary figure III). After multivariable adjustment, the presence of CTO among patients with multivessel or left main CAD conferred the highest risk for the composite end point (online supplementary table III).
Influence of CTO target vessel and plaque composition
Whereas there was no difference in the rate of all-cause mortality depending on the target CTO vessel and plaque composition, the presence of occluded right coronary artery (HR 2.11; 95% CI 1.28 to 3.49, p=0.003) and mixed CTO plaque (HR 1.64; 95% CI 1.04 to 2.60, p=0.035) were independently predictive of the composite end point compared with patients with moderate-to-severe CAD. This was primarily driven by an independent association between occluded right coronary artery (HR 2.46; 95% CI 1.41 to 4.30, p=0.002) and mixed CTO plaque (HR 1.72; 95% CI 1.02 to 2.92, p=0.043) and late revascularisation.
Supplementary analyses
The hazards models additionally adjusted for differences in segment-stenosis score (see online supplementary tables IV and V) as well as prognostic analyses of the final study sample including subjects with early revascularisation are presented in the online supplementary file (see online supplementary figures IV to VII and online supplementary tables VI to VII).
Discussion
In this large prospective multicentre international registry of consecutive individuals with suspected CAD, we determined the prognosis of CTO detected at the time of CCTA. In the intermediate-term follow-up, the presence of CTO was incrementally and significantly associated with decreased survival compared with normal coronary arteries and non-obstructive CAD, and equalled the mortality rates of moderate-to-severe CAD or multivessel or left main CAD. Furthermore, the non-invasive diagnosis of CTO conferred the highest adjusted risk for the composite prognosis end point both in the overall population as well as in patients with multivessel CAD—an observation that was primarily driven by an increase in late coronary revascularisations. Our observations may be considered widely generalisable given the fact that our cohort represents the largest available number of patients undergoing CCTA across multiple international sites.
There are limited data about the prognosis of CTO. As such, the majority of the angiographic reports in stable CTO patients were conducted to investigate the effect of CTO recanalisation on mortality. Most of these non-randomised cohort studies and meta-analyses showed improved survival with successful (re-opened) versus failed or non-attempted CTO percutaneous coronary intervention.2 15–18 Subsequently, an array of longitudinal reports in acute myocardial infarction and ischaemic systolic heart failure found an independent relationship between the presence of CTO and higher mortality at follow-up.3 19 20 In view of these findings, the current investigation may be considered the first to provide a direct comparison between CTO and a wider spectrum of coronary lesions rather than the re-opened or absent CTO only. Specifically, CTO conferred a mortality rate that was ninefold higher compared with normal coronaries, and threefold higher than non-obstructive CAD, but similar in magnitude to moderate-to-severe CAD and multivessel or left main CAD. Although the rates of all-cause mortality at 12 months for CTO (2.3%) and multivessel or left main CAD (2.1%) in our cohort slightly fell behind the present conventional criterion of ‘high risk’ (traditionally defined as >3% annual mortality rate),10 21 the rate of death for proximal CTO corresponded to 12-month increment of 3.1%. This latter observation corresponds well with the Swedish registry among 14 441 patients with CTO, wherein CTO in proximal segments were associated with higher mortality risk than CTO in distal segments.19 Our results extend prior angiographic data, and emphasise the importance of integration of CTO detected non-invasively as a marker of reduced survival similar to moderate-to-severe CAD.
Our report also provides data on subsequent myocardial infarction and late coronary revascularisation in patients with CTO. Particularly, the presence of CTO conferred the highest adjusted risk for the composite outcome of all-cause mortality, non-fatal myocardial infarction and late revascularisation in the risk-adjusted models stratified by the severity and extent of obstructive CAD. Whereas this difference was primarily driven by an increase in late coronary revascularisations, we failed to demonstrate any additional risk of all-cause mortality and non-fatal myocardial infarction in CTO compared with moderate-to-severe CAD. Of note, this replicates the latest cohort studies on CTO, indicating comparable rates of myocardial infarction in successful (re-opened) versus failed CTO percutaneous coronary intervention,22 23 and strengthens the need for a randomised trial to fully understand the impact of CTO on downstream myocardial infarction and late coronary revascularisation. Altogether, our findings reinforce the notion that CTO does not increase the risk of myocardial infarction per se. Nevertheless, the coexistence of CTO in a non-infarct-related artery supplied by collaterals from the infarct-related artery almost invariably results in greater myocardial mass injury and inferior outcomes.3 19
Given almost two-thirds of our CTO patients had a multivessel CAD, we adjusted for the presence of concomitant obstructive but non-occlusive coronary vessels, showing the association between CTO and significantly higher rate of the composite outcome (driven by an increase in late revascularisation) in the subset of patients with multivessel or left main CAD. It might be that CTO are accompanied by less collateral flow from the obstructive coronary stenoses localised in the non-CTO vessels (and vice versa) resulting in a lower threshold for symptoms during follow-up. These findings may offer clues as to the clinical reasoning behind late coronary revascularisation in CTO, and large-scale outcome studies assessing the relevance of concomitant CAD among individuals with CTO now appear warranted.
We have hypothesised that the deleterious effect of CTO might be limited to certain subgroups. Particularly germane to this concept, we observed a significantly higher rate of late revascularisation in a CTO located in the right coronary artery but not in a CTO located in the left coronary artery when compared with moderate-to-severe CAD. We speculate that the presence of CTO located in the right coronary artery may more easily precipitate angina exacerbation resulting from impaired coronary flow through concomitant stenoses located in the left coronary artery system. Additionally, the presence of mixed CTO plaque but not the presence of purely calcified CTO plaque was independently predictive of late revascularisation. Again, we hypothesise this finding may be partly explained by higher difficulty levels of percutaneous recanalisation in severely calcified CTO lesions that might have been less frequently attempted in our cohort.
There are some caveats associated with our report. Because it is an observational study, there may be unmeasured or residual confounding despite adjustment for differences in symptoms, age, gender, cardiovascular risk factors and segment-stenosis score. Selection bias cannot be discounted, and 37% of subjects had missing follow-up data for major adverse cardiac events. Furthermore, we had no information on ischaemia-driven or target vessel revascularisation as well as its procedural outcome and relation to plaque composition. Also, the subanalysis with respect to the method of late coronary revascularisation was underpowered to draw any definite conclusions. Since the presence of CTO was adopted from CCTA images and not coronary angiography, the possibility of both false-positive and false-negative results cannot be dismissed. Furthermore, the employed definition of CTO did not account for the estimated time of occlusion prior to CCTA, which may have influenced the perceived rate of prognosis endpoints. The analysis of the predictive value of CCTA over traditional risk factors in CTO was not possible due to the restricted number of observations. Finally, given the fixed cut-off value for statistical significance within multiple comparisons we cannot exclude that some of the significant results are due to chance.
Conclusions
The present study represents the first data to determine the prognostic value of CTO among patients undergoing non-invasive angiography for suspected CAD. Whereas the presence of CTO did not predict mortality over moderate-to-severe CAD, it conferred the highest adjusted risk for major adverse cardiovascular events (driven by an increase in late coronary revascularisations) both in the overall population as well as in patients with multivessel or left main CAD.
Key messages
What is already known on this subject?
While the prognosis of chronic total occlusion (CTO) has been examined in the setting of percutaneous coronary intervention or myocardial infarction, the associations between future clinical outcomes and CTO in patients undergoing non-invasive coronary CT angiography (CCTA) for suspected coronary artery disease (CAD) have not been reported to date.
What might this study add?
Our study demonstrates that the non-invasive detection of CTO by CCTA is associated with decreased survival compared with normal coronaries and non-obstructive CAD, but equals the mortality rates of moderate-to-severe CAD.
In addition, the presence of CTO conferred the highest adjusted risk for major adverse cardiovascular events (driven primarily by an increase in late coronary revascularisations).
How might this impact on clinical practice?
This study highlights the need for developing strict clinical surveillance and management plan (including the rationale for late coronary revascularisation) for individuals with CTO detected on CCTA.
References
Footnotes
Contributors Drs MPO and FYL contributed to data analysis and interpretation as well as drafting, critical revision and final approval of the manuscript. Drs YL, SA, MHAl-M, DA, JJB, DSB, MJB, FC, TQC, H-JC, KC, BJWC, RCC, ADL, GMF, MH, JH, PAK, Y-JK, JAL, EM, HM, GP, GR, RR, LJS, TCV, MG, ECJ and JMP contributed to data acquisition and interpretation as well as critical revision and final approval of the manuscript. Dr HG contributed to data analysis as well as critical revision and final approval of the manuscript. Dr JKM contributed to planning, design, conduction and reporting of the work described in the article as well as critical revision and final approval of the manuscript. Dr JKM is responsible for the overall content as guarantor.
Funding The research reported in this publication was funded, in part, by the Heart, Lung and Blood Institute of the National Institutes of Health (Bethesda, Maryland, USA) under award number R01 HL115150, and also supported, in part, by the Dalio Institute of Cardiovascular Imaging (New York, New York, USA) and the Michael Wolk Heart Foundation (New York, New York, USA).
Competing interests Dr JKM receives funding from the Dalio Foundation, National Institutes of Health and GE Healthcare. Dr JKM serves on the scientific advisory board of Arineta and GE Healthcare, and has an equity interest in Cleerly. All other coauthors have no relevant disclosures.
Patient consent Obtained.
Ethics approval Weill Cornell Institutional Review Board.
Provenance and peer review Not commissioned; externally peer reviewed.