Article Text

Abstract
Clinical introduction A woman in her 30s presented to the emergency department with sudden-onset abdominal pain with hypotension and tachycardia. She gave a history of congenital heart disease for which she had previously undergone multiple operations. On examination she demonstrated right upper quadrant tenderness. She underwent an urgent multiphase CT (figure 1A–C).
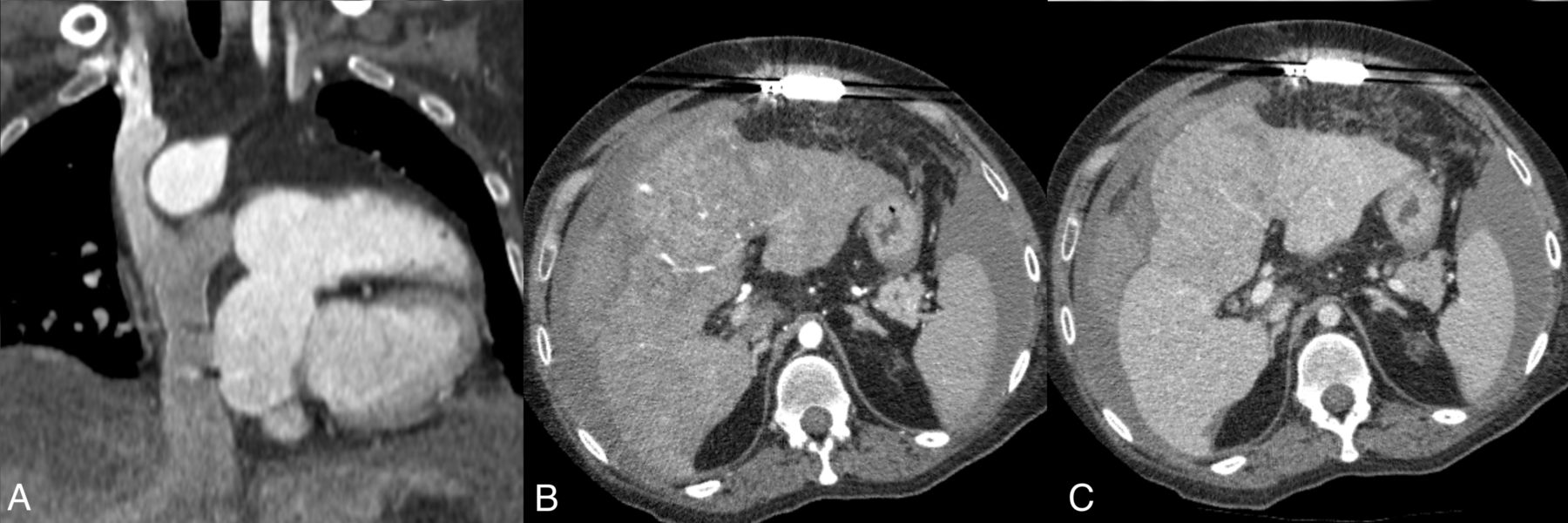
(A) Arterial phase coronal CT. (B) Arterial phase axial CT. (C) Portal venous phase axial CT.
Question What is the underlying liver pathology?
Hepatocellular adenoma
Cholangiocarcinoma
Hepatocellular carcinoma
Focal nodular hyperplasia
Hepatoblastoma
Question
- Fontan physiology
Statistics from Altmetric.com
Answer: C
CT images of the chest confirmed a Fontan circulation (figure 1A). CT of the upper abdomen showed a 14 cm mass in the liver with nodularity of the background liver contour in keeping with cirrhosis (figure 1B). On arterial phase images, the mass was hyperenhancing relative to the surrounding liver (figure 1B) and it demonstrated washout on portal venous phase images (figure 1C). Using the widely adopted LI-RADS system, a definitive diagnosis of hepatocellular carcinoma (HCC) can be made on the basis of imaging alone in a patient with cirrhosis when a lesion measuring greater than 2 cm demonstrates arterial hyperenhancement and portal venous washout.1 A biopsy is not required for confirmation. Serum alpha-fetoprotein was subsequently measured to be 2380 kU/L (normal range 0–10). There was active extravasation from the liver lesion with large volume haemoperitoneum in keeping with HCC rupture. Branches of the left hepatic artery supplying the hypervascular tumour were selectively embolised by interventional radiology (figure 2A). A repeat CT showed decreased vascularity of the HCC (figure 2B).

{kind=link}
{kind=link}
(A) Digital subtraction angiogram with microcatheter superselectively in left hepatic artery branch supplying enhancing tumour (arrows). (B) Postembolisation arterial phase CT showing decreased enhancement in the treated tumour.
It is now recognised that liver cirrhosis is an important late complication in patients who have previously undergone the Fontan procedure. The development of chronic liver disease has been shown to be related to Fontan duration and hepatic venous pressures2 and it is theorised that the resultant congestive hepatopathy can progress to hepatic fibrosis, cirrhosis and HCC. Arterialised so-called Fontan nodules are a frequent finding in the Fontan population occurring in 26% of patients in one series and the underlying pathology is felt to be focal nodular hyperplasia3; however, these Fontan nodules are usually small measuring less that 3 cm and they do not demonstrate portal venous phase washout which is a feature of HCC. A Japanese nationwide survey found that of 2700 patients who had undergone the Fontan procedure, 1.15% developed cirrhosis and/or HCC.4 In the same survey, the mean age of diagnosis of cirrhosis was 23 and the mean age of diagnosis of HCC was 31. It has been recommended that all Fontan patients should undergo surveillance liver imaging.5
Footnotes
Contributors ROD prepared the manuscript and images. SF and TJCB participated in the care of the patient and critically reviewed the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.