Article Text

Abstract
Objective To assess median and percentile birthweight distribution in women with various groups of heart disease relative to a contemporaneous comparison group.
Methods Data on birth weight and gestational age were collected from 1321 pregnancies ≥24 weeks’ gestation in 1053 women with heart disease from seven UK maternity units. Women were assigned to one of 16 groups according to their cardiac lesion. In units where it was possible, data on two births, one delivering before and one after index cases, were collected, giving 2307 comparators. Birthweight percentiles (corrected for gestational age, sex and parity) were calculated using Aberdeen norms. We assessed the association of birth weight with cardiac lesion, maternal hypoxaemia (saturations <90%), systemic ventricular function and beta-blockers.
Results 1321 pregnancies in women with heart disease and 2307 comparators were studied. Almost all groups with heart disease had lower median and percentile birth weights than comparators, significantly in 10 groups, the biggest effect seen in women with Fontan circulation, pulmonary hypertension, prosthetic heart valves, systemic right ventricle, Marfan syndrome, repaired tetralogy of Fallot and cardiomyopathy (in that order). In 307 pregnancies, women took beta-blockers; median birth weight adjusted for maternal age, parity and the effect of the cardiac lesion was 3116.7 g (IQR 790.4) when beta-blockers were used and 3354.3 g (IQR 634.1) when they were not (p<0.001). 17 women had saturations <90%, and median birth weight was significantly lower, 3105.4 g (IQR 1288.9) versus 3387.7 g (IQR 729.8) (p=0.006).
Conclusion Our findings identify specific groups of women with heart disease at risk of having a small baby.
- pregnancy
- congenital heart disease
Statistics from Altmetric.com
Introduction
Pregnancies complicated by maternal heart disease are increasingly common as more women with congenital heart disease are surviving to adulthood1 and deciding to have a family; women are delaying pregnancy when medical comorbidities including heart disease are more prevalent2 and increasingly assisted reproductive therapies are used in this group.3 Studies such as the European Registry of Heart Disease in Pregnancy (ROPAC) describe high rates of maternal and neonatal morbidity and mortality in pregnancies complicated by congenital and acquired heart disease.4 Maternal events such as heart failure and arrhythmia have been emphasised,5 6 but neonatal problems (particularly preterm delivery and fetal growth restriction) are more prevalent, but less well appreciated.7 Further, while scoring systems can identify those women who are at risk of cardiac complications during pregnancy with reasonable accuracy,8 they are unable to predict obstetric complications,9 implying that mechanisms other than the severity of the underlying cardiac condition are important. Gelson et al reported 331 pregnancies in women with heart disease; the corrected birthweight percentiles (corrected for gestational age, parity and fetal sex) were significantly lower compared with controls.7 Although not all low percentile birthweight babies (termed ‘small for gestational age’ (SGA)) are growth restricted (some are just ‘normally small’), an increase in the proportion of babies with birth weights below the tenth percentile indicates an increased rate of growth restriction. Birthweight percentiles epidemiological studies associate fetal growth restriction with long-term cardiovascular disease in the mother10 and worse immediate11 and long-term cardiovascular offspring outcomes12
Gelson et al reported that the use of beta-blockers in pregnancy correlated negatively with fetal growth, as did maternal cyanosis.7 ROPAC reported that the babies of the 291 mothers who took beta-blockers during pregnancy had a 270 g lower mean birth weight (from 2830 g vs 3100 g) compared with the 897 babies of pregnancies where the mother did not take any medications.13 However, the authors did not correct for the cardiac lesion for which the beta-blockers were used, so it remained a possibility that the lesion itself rather than the use of beta-blockers that was responsible. Ersboll et al showed women with cardiac disease had an increased risk of having a baby born SGA (OR 2.65),14 but it was underpowered to assess whether there was difference in birth weight between different types of cardiac lesion. Presbitero et al reported babies of mothers with cyanosis had a median birth weight at term of 2575 g, which approximates to the 10th percentile,15 suggesting a large proportion of neonates were SGA and also growth restricted.
Impaired placental development is associated with abnormal uterine artery blood flow and fetal growth restriction.16 Pieper et al observed similar changes in uterine artery blood flow patterns in pregnant women with compromised maternal cardiac function.17 In another study performed in a cohort of 49 women with corrected coarctation of the aorta, birth weight was reduced in the overall group, but lowest in women taking beta-blockers (mean difference 418 g; 3232 g vs 2814 g).18 To date, no large study has stratified women with different types of heart disease to assess whether some are at greater risk of having a small baby. We therefore carried out a multicentre cohort study to determine whether there is a relationship between the type of maternal heart disease and birth weight.
Methods
Data were collected through medical and obstetric notes review of women with heart disease giving birth between 1 January 1998 and 31 November 2017 in seven tertiary UK centres specialising in the care of such women. All centres kept contemporaneous records of women with heart disease who had been managed at their centre through an obstetric cardiac service. Units from which comparators were obtained have large maternity services serving their local geographical area as well as their specialised services, making the controls reasonably representative. Those with mitral valve prolapse and minor arrhythmias were excluded, as were cases where birth weight was missing. Collection of identifiable data previously recorded as part of routine clinical care was restricted to members of the clinical team. Aggregated data analysis was limited to data provided without patient identifiers, so informed consent was not required by UK law. Local research governance at Imperial College Healthcare approved the study protocol.
Demographic and baseline maternal data collected were age at pregnancy, race/ethnicity, smoking status, underlying cardiac diagnosis and anatomy, prior surgical repair, New York Heart Association class and presence of maternal hypoxaemia (resting saturations <90% at first maternity visit). We collated qualitative echocardiographic data assessing ventricular function by ejection fraction (%EF) prior to pregnancy, which was graded as normal (EF ≥55%), mild (EF 45%–54%), moderate (EF 30%–44%) or severe impairment (<30%). For the purposes of analysis, women were assigned to one of 16 functional groups (see table 1). When data collection systems made this possible, a comparator delivering immediately before and after the index case, matched for age (±5 years) and parity, was used to control for secular changes. Where comparators had obstetric problems potentially impacting on pregnancy outcome, these are listed in table 1. Cases with fetal chromosomal abnormalities and twin pregnancies were excluded.
Baseline demographics
We recorded the use of beta-blockers and the presence of the following obstetric complications that impact fetal growth: (1) pregnancy-induced hypertension (PIH, ≥140 mm Hg systolic or ≥90 mm Hg diastolic after 20 weeks’ gestation), (2) pre-eclampsia (PIH with proteinuria >0.3 g/24-hour urine collection or protein creatinine ratio >30) and (3) diabetes (both pre-existing and gestational). The first two are typically associated with lower birth weights, the last with higher birth weights. Gestational age at delivery and birth weight were noted, and birthweight percentiles were calculated using the Aberdeen norms, which allow for gestational age, parity and sex.19
Statistics
Data were analysed using SPSS V.23. Categorical data are presented as frequencies (numbers) and percentages. Data that approximate to a Gaussian distribution (maternal age, Body Mass Index (BMI)) are presented as mean values+1 SD. Non-Gaussian data are presented as medians with IQR. Correlations were calculated using Pearson’s product moment if variables were continuous and Spearman’s rank–order correlation if either of the variables was ordinal. Differences between continuous variables were assessed with the Mann-Whitney U test if they were not normally distributed. Multiple regression analysis correcting for the use of beta-blockers and relevant obstetric complications allowed us to identify whether a specific diagnostic group/lesion was associated lower birthweight percentile. All tests were two tailed and p value <0.05 was considered statistically significant.
Birth order significantly affects maternal and fetal/neonatal variables. Analysis was complicated by the fact that a third of women with heart disease (355; 33.7%) did not have their first pregnancies in the units for which data were collected, and therefore data on their first pregnancies were not available. This meant that exact correction for the effects of birth order was not possible. However, the major differences due to parity occur between first and second pregnancies, so we categorised pregnancies in both cases and comparators as either nulliparous (first pregnancy and labour) or parous (second or subsequent pregnancy) and adjusted for the differences by multiple regression.
Results
A total of 1321 pregnancies in 1053 women with heart disease were identified. In addition, 2307 comparators were identified from six centres. Four provided 2:1 comparators/cases (comparators before and after each index case) and two provided 1:1 comparators/cases (alternating between the women delivering before or after each index case). Matching for age (±5 years) and parity was only fully possible in three centres. In two centres, not all comparators could be matched for parity, in one there was only matching for age, in one matching for year of birth and not date of birth, and in one unit (contributing 6% of cases) collection of comparators was not possible. Accordingly, comparators could not be analysed as fully matched controls and instead statistical correction for differences in maternal age and parity was applied during the data analysis. Baseline demographics of all women are displayed in table 1. Data showing the number of pregnancies in each functional cardiac group, including the women’s original underlying diagnosis, are shown in table 2.
Functional diagnostic groups
Analysis of demographic factors showed there were significantly fewer women with heart disease who were South Asian compared with comparators (10.7% vs 13.8%). Also, despite matching for parity and age in a substantial proportion of cases and comparators, women with heart disease were significantly younger (30.0 years vs 30.4 years) and more likely to be nulliparous (52.8% vs 57.7%), although the differences were small and unlikely to be of major clinical significance. However, because of these differences, birth weight was adjusted for parity and maternal age during statistical analysis. Women with heart disease had a significantly higher BMI compared with comparators (25.1 vs 24.3 kg/m2), but no adjustment was made for height/weight/BMI as these can be part of the phenotype of the cardiac condition. Cigarette smoking rates did not differ significantly between groups, 7.5% in women with cardiac disease and 7.4% in comparators.
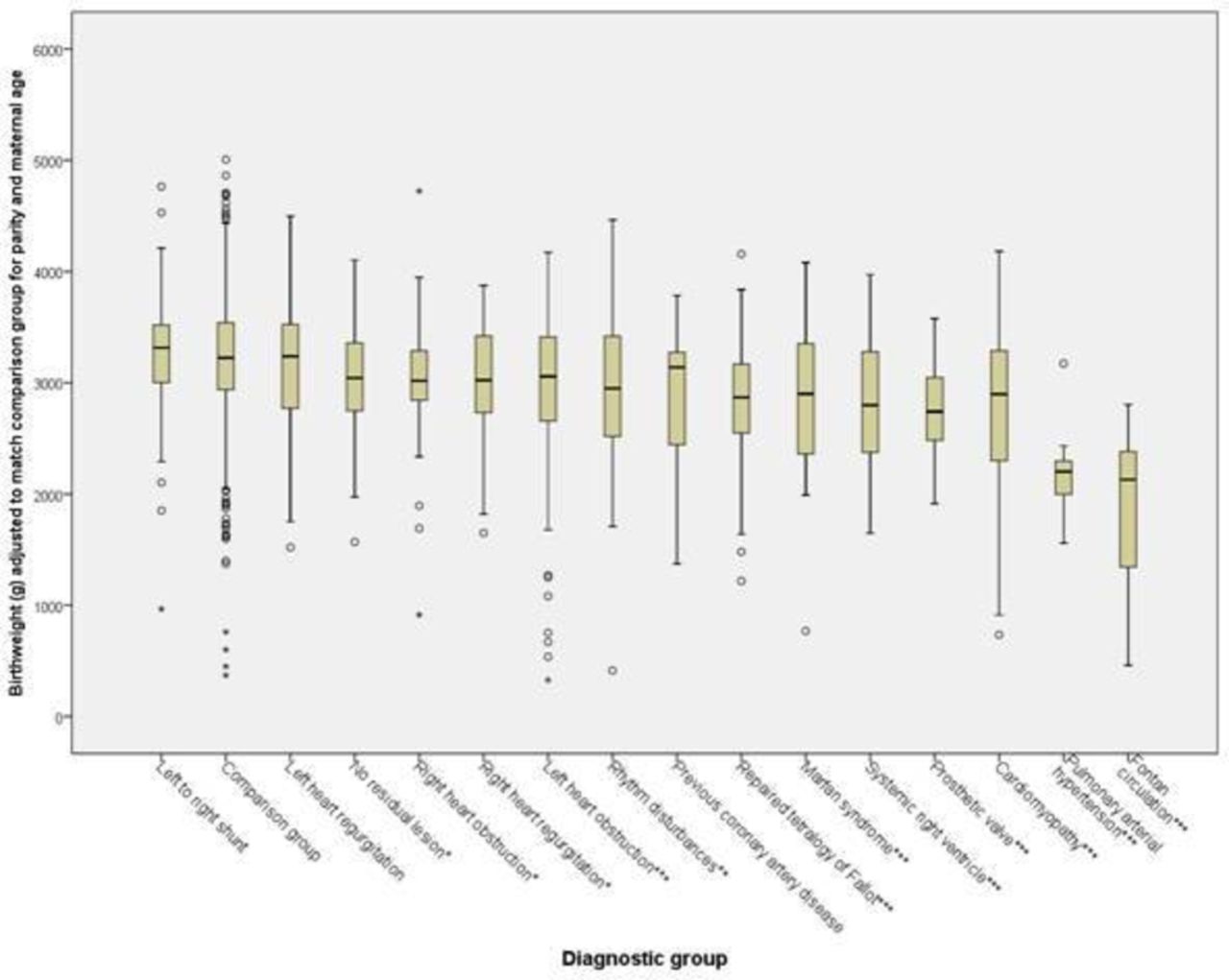
Univariate analysis demonstrated all 16 groups with heart disease had lower birth weights (adjusted for parity and age) than comparators (the reference for adjustment) (figure 1). Mann-Whitney U rank-sum analysis showed that this was not statistically significant for left-to-right shunt (p=0.286), non-residual lesion (p=0.063) or left heart regurgitation (p=0.401), but it was statistically significant in all other cases. Results were similar when only women having their first pregnancy were analysed (figure 2), meaning it is unlikely that any correlation between successive pregnancies has substantially affected our results.
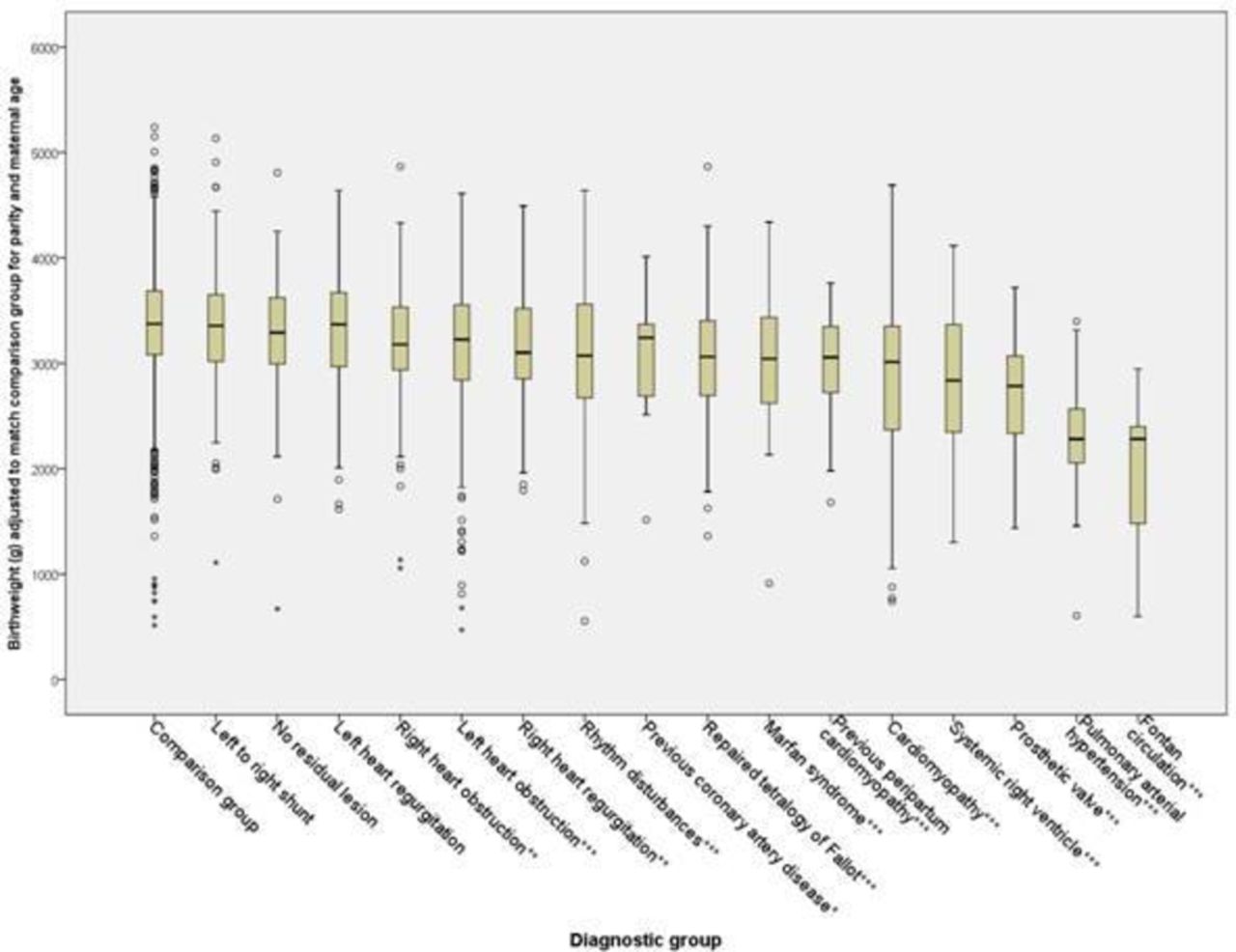
Birth weight adjusted by multiple regression for parity and maternal age and based on the median birth weight in the comparison group. The graph shows median (line) with IQR (box). The whiskers represent 1.5 times the overall height of the box, which with a normal distribution equates to approximately the 95% CIs of the population distribution, except that in cases with no outliers (circles) beyond the whisker, the whisker represents the minimum or maximum value. Significance: *p<0.05, **p<0.01, ***p<0.001. ± The significance values quoted refer to a comparison between each individual diagnostic subgroup and the overall comparison group, which was used as the universal reference of ‘normality’ and served to compensate for any changes of median birth weight and management policy of the whole population over time.

Birth weight adjusted by multiple regression for parity and maternal age and based on the median birth weight in the comparison group for first pregnancies only. The whiskers represent 1.5 times the overall height of the box, which with a normal distribution equates to approximately the 95% CIs of the population distribution, except that in cases with no outliers (circles) beyond the whisker, the whisker represents the minimum or maximum value. Significance: *p<0.05, **p<0.01, ***p<0.001. ± The significance values quoted refer to a comparison between each individual diagnostic subgroup and the overall comparison group, which was used as the universal reference of ‘normality’ and served to compensate for any changes of median birth weight and management policy of the whole population over time.
An important component of birth weight is gestation at delivery, and women with cardiac disease delivered earlier than comparators (figure 3). Mann-Whitney U rank-sum analysis showed that this was not statistically significant for left heart regurgitation (p=0.746) or left-to-right shunt (p=0.096), but it was significant for all other groups.

Gestational age in weeks. Graph shows median (line) with IQR (box). The whiskers represent 1.5 times the overall height of the box, which with a normal distribution equates to approximately the 95% CIs of the population distribution, except that in cases with no outliers (circles) beyond the whisker, the whisker represents the minimum or maximum value. Significance: *p<0.05, **p<0.01, ***p<0.001.
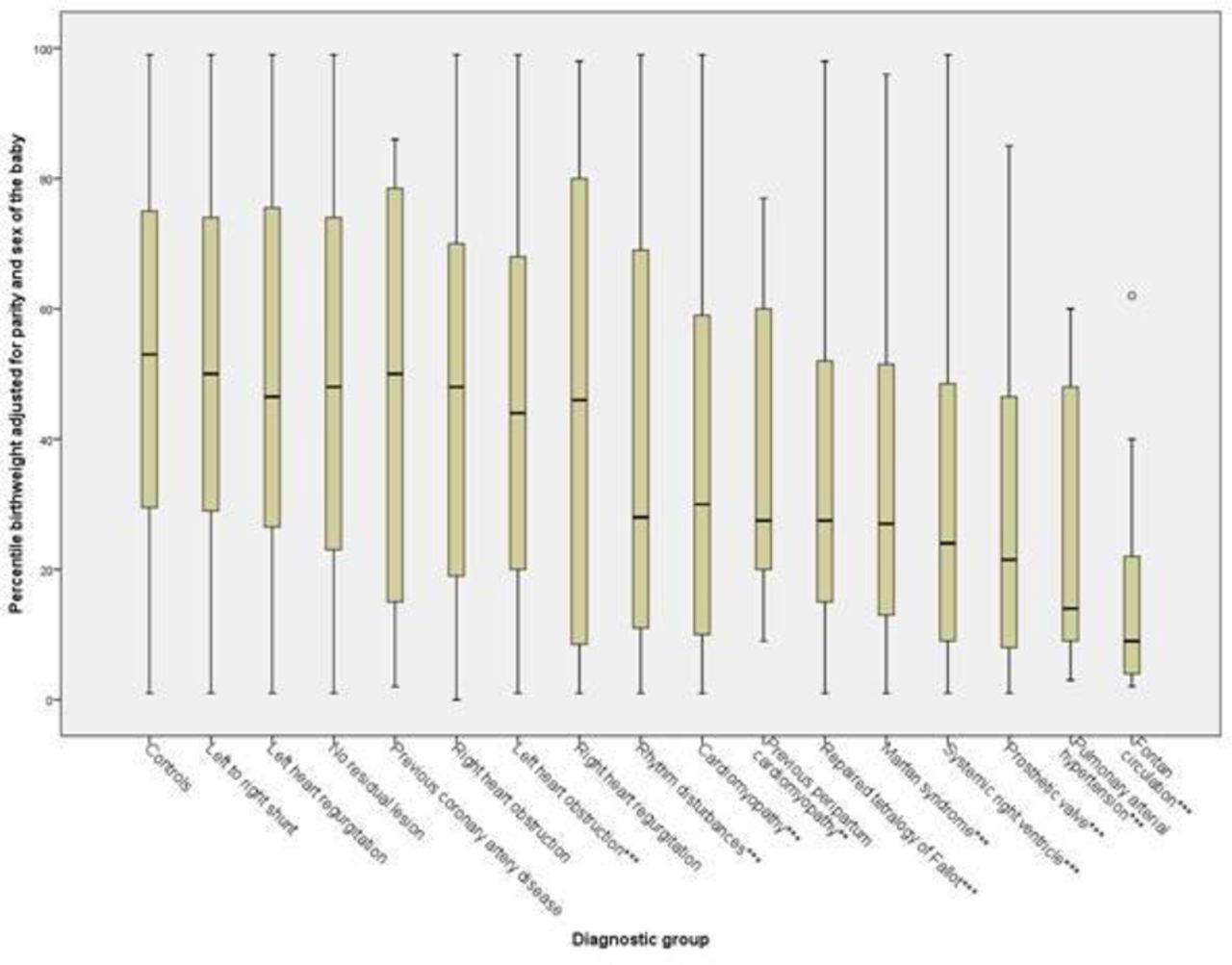
Assessment of fetal grfetalcan be made by calculating the percentile birth weight using Aberdeen nomograms, which adjust for gestational age, sex of the baby and the parity of the mother.19 Figure 4 shows percentile birth weight was lower in all groups with heart disease than in comparators; however, the difference was not significant for left-to-right shunt (p=0.870), coronary artery disease (p=0.338), left heart regurgitation (p=0.147), no residual lesion (p=0.059), right heart regurgitation (p=0.059) and right heart obstruction (p=0.051). It was significant for previous peripartum cardiomyopathy (PPCM) (p=0.002) and for all other groups (p<0.001).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Percentile birth weight adjusted for parity and sex of the baby. Graph shows median (line) with IQR (box). The whiskers represent 1.5 times the overall height of the box, which with a normal distribution equates to approximately the 95% CIs of the population distribution, except that in cases with no outliers (circles) beyond the whisker, the whisker represents the minimum or maximum value. Significance: *p<0.05, **p<0.01, ***p<0.001.
Analysis of obstetric variables showed that in women with heart disease, only the diagnosis of pre-eclampsia significantly impacted on birth weight corrected for age, parity and lesion (median birth weight 3059.7 g (IQR 962.0) in women with pre-eclampsia vs 3340.9 g (IQR 721.2) in those without (p=0.03)).
In 307 pregnancies in women with heart disease, beta-blockers were used (table 3). We were unable to determine the beta-blocker used, nor could we ascertain exactly when they were commenced. Beta-blocker usage was much higher in some conditions than others, as shown in table 1. As many lesions with high beta-blocker usage were also associated with low birth weight, we created a birth weight adjusted by multiple regression for parity, maternal age and cardiac lesion, with the population comparison group as the reference. This resulted in a mean birth weight for all groups of 3334.1 g, with medians ranging from 3306.2 g to 3620.1 g. Using this adjusted birth weight, there remained a highly significant association with the use of beta-blockers. Median birth weight was 3116.7 g (IQR 790.4) when beta-blockers were used and 3354.3 g (IQR 634.1) when they were not (p<0.006), a difference of 237.6 g. Seventeen women had saturations <90%, and their median birth weight was significantly lower, 3105.4 g (IQR 1288.9) vs 3387.7 g (IQR 729.8), a difference of 237.6 g (p=0.006).
Distribution of beta-blocker usage in all women included in the study
Echocardiography showed that in 103/1321 pregnancies, the mother had a degree of impaired ventricular function prior to pregnancy (67 mild impairment, 27 moderate impairment and 9 severe impairment). Impaired ventricular function was associated with a significantly lower birth weight corrected for parity, maternal age and lesion, 3052.6 g (IQR 888.9) vs 3401.9 g (IQR 711.1) (p<0.001), although there was no correlation with the severity of the impairment (3131.6 g if mildly impaired, 2977.6 g if moderately impaired and 3091.4 g if severely impaired). Median percentile birth weight adjusted for maternal age was also lower, 13.4 vs 28.9 (p<0.001).
Discussion
The principal finding of this study is that women with heart disease have smaller babies than controls and there is significant variation in birth weight between women with different forms of heart disease. Furthermore, the use of beta-blockers (even after correction for the effect of the individual lesion), impaired maternal ventricular function and maternal oxygen saturations <90% are all associated with significantly lower birth weight.
The strength of our study is that it included a large number of pregnancies, similar to ROPAC.4 Furthermore, our study is strengthened by the ability to compare outcomes of those with cardiac disease with a contemporaneous population comparison group. Unfortunately, matching all comparators for maternal age and parity was not possible, and it remains a weakness that one centre was not able to give us any such data, although comparators were missing for fewer than 6% of the cases.
By collating a large number of pregnancies, we have been able to examine the variation in birth weight with different maternal lesions. From the 16 cardiac lesions, there were eight where birth weight and birthweight percentile were significantly lower than controls, with the lowest in women with a Fontan circulation and pulmonary hypertension. Median gestation at delivery of babies in these last two groups was also lower at 36 and 35.5 weeks, respectively. In addition, mothers with prosthetic valves, systemic right ventricle (SRV), cardiomyopathy, previous PPCM, Marfan syndrome and repaired tetralogy of Fallot all had significantly smaller babies than controls.
Previously, impaired maternal cardiovascular adaptation to pregnancy in healthy women had been associated with fetal growth restriction and SGA neonates. In a cohort of healthy women, Bamfo et al demonstrated that cardiac output, stroke volume and stroke index were all significantly lower in women delivering a growth-restricted baby compared with those who did not.20 Melchiorre et al reported that maternal diastolic dysfunction was more common in pregnancies complicated by fetal growth restriction.21 It is possible that these associations are more marked in women with underlying heart disease. An American cohort study demonstrated that women with heart disease had a greater risk of having an SGA baby.22 In women with established congenital heart disease, the OR of having an SGA baby was 1.5 (CI 1.3 to 1.8) and in women with heart failure, the OR was 2.0 (CI 1.5 to 2.6).22 Our study found that women going into pregnancy with impaired ventricular function had a smaller baby, but surprisingly this did not vary significantly with the degree of impairment. This may be due to relatively small numbers in these groups. However, Siu et al found that impaired cardiac function was associated with a greater risk of having an SGA baby,23 although they combined a low ejection fraction with valvular obstruction and surprisingly only reported 14 of 252 babies (5.6%) as being <10th percentile at birth (compared with 225/1321, 17% in our study). We suggest that in those with established impaired ventricular function, growth may be diminished partly because of reduced maternal adaptation to pregnancy, alongside other mechanisms including impaired placental development.
Pieper et al demonstrated that abnormal uteroplacental flow was more common in women with cardiac disease and birth weight was significantly lower (3036 g vs 3578 g, p=0.005) and higher rates of SGA (16.3% vs 4.3%) in the cardiac group compared with controls.17 They related abnormalities in uterine blood flow to cardiac function, before and during pregnancy, suggesting a linkage between preceding cardiac dysfunction and placental development.
The use of beta-blockers was associated with a higher rate of low birth weight, with a median birth weight of 237.6 g less in those taking beta-blockers even after correcting for the nature of the cardiac lesion. This agrees with Ruys et al who demonstrated birth weight was 280 g less when beta-blockers were used.13 A Danish study examining beta-blocker usage in women with cardiac disease (51 treated vs 124 not) found them to be associated with a significantly higher rate of SGA babies (29% vs 15%). These results remained unchanged following a multivariate regression to assess the impact of other factors on birth weight.14 This effect is particularly important in women with Marfan syndrome, previous PPCM and cardiomyopathy, all of whom had a high rate of beta-blocker use (62% (47/76), 50% (13/26) and 49% (43/88), respectively).
Our study was not without its limitations; it was retrospective, and some data were incomplete or missing. Women were classified by their predominant cardiac lesion and we recognise that this classification may not always be appropriate. Our ability to compare cases with matched controls was limited in some of the centres. We were only able to ascertain systemic ventricular function at a single point prior to pregnancy. Furthermore, while we identified an association between beta-blockers and impaired fetal growth, we were unable to quantify exactly when women commenced beta-blockers and taking beta-blockers for longer periods had a more profound effect. There is the risk of confounding by indication, as those with more severe forms of heart disease are more likely to require beta-blocker treatment, while at the same time these women are more likely to have pregnancies complicated by fetal growth restriction. We have minimised this effect as much as we can by calculating a birth weight adjusted for lesion.
Understanding which women are more likely to have growth-restricted babies is important because it determines obstetric management. Women in higher risk groups require closer fetal surveillance with serial scans assessing fetal growth. Early delivery may be required as growth restriction is associated with higher rates of stillbirth.24 Further, growth-restricted babies are less able to tolerate labour, so are more likely to need delivery by emergency caesarean section.25 This has higher risks of bleeding, infection and thromboembolism, being undesirable for certain women with heart disease, particularly those with pulmonary hypertension and a Fontan circulation.26 27
Our data also demonstrate that although women in some groups of cardiac disease have babies with a slightly lower birth weight than controls, the majority of their babies have a birth weight within the normal range and, in these cases, extra fetal surveillance may not be warranted.
Key messages
What is already known on this subject?
Pregnancy in women with heart disease is known to be associated with a higher risk of both maternal and fetal cofetalations, including low birth weight, but previous studies have not quantified birth weight by cardiac lesion in relation to a contemporaneous population comparison group.
What might this study add?
This study suggests that almost all cardiac lesions are associated with lower birth weight than in a contemporaneous population comparison group, although this is only both clinically and statistically significant in some groups, in particular women with Fontan circulation, pulmonary arterial hypertension, prosthetic heart valves and systemic right ventricle. Ventricular impairment, low maternal oxygen saturations and use of beta-blockers are also associated with a lower birth weight.
How might this impact on clinical practice?
The identification of women who are at particular risk of having a small baby allows them to have extra fetal surveillance during pregnancy, enhancing the ability to counsel them regarding the timing and mode of delivery.
References
Footnotes
Contributors MC conceived the idea for the study and designed the data collection and collated data from C&W. MS, SW, GM, GU, TE, ADJ, ARM, SH, MS and JB were responsible for data collection at each of the other sites. MC and PS analysed the data. MC wrote the first draft revised by MRJ and PS. All authors reviewed and approved the final version of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.