Article Text

Abstract
Background Increased longevity in patients with congenital heart disease (CHD) is associated with late complications, mainly heart failure, which may not be amenable to redo surgery and become refractory to medical therapy and so, trigger referral for transplantation. We assessed the current role and future prospects of heart and heart-lung transplantation for patients with CHD in England.
Methods We performed a retrospective analysis of hospital episodes for England for 1997–2015, identifying patients with a CHD code (ICD-10 ‘Q2xx.x’), who underwent heart or heart-lung transplantation.
Results In total, 469 transplants (82.2% heart and 17.8% heart-lung) were performed in 444 patients. Half of patients transplanted had mild or moderate CHD complexity, this percentage increased with time (p=0.001). While overall, more transplantations were performed over the years, the proportion of heart-lung transplants declined (p<0.0001), whereas the proportion of transplants performed in adults remained static. Mortality was high during the first year, especially after heart-lung transplantation, but remained relatively low thereafter. Older age and heart-lung transplantation were strong predictors of death. While an increase in CHD transplants is anticipated, actual numbers in England seem to lag behind the increase in CHD patients with advanced heart failure.
Conclusions The current and future predicted increase in the numbers of CHD transplants does not appear to parallel the expansion of the CHD population, especially in adults. Further investment and changes in policy should be made to enhance the number of donors and increase CHD transplant capacity to address the increasing numbers of potential CHD recipients and optimise transplantation outcomes in this growing population.
- congenital heart disease
- transplantation
- survival
Statistics from Altmetric.com
Introduction
Major advances in the surgical and medical management of congenital heart disease (CHD) in recent decades have allowed an increasing number of patients to survive to adult life.1 2 In particular, the prevalence of CHD of great complexity in adults has increased: Almost half of patients with complex CHD in the year 2000 were adults and this number is likely to have risen further.3 With improved longevity, there has also been an increase in the incidence of long-term complications, especially chronic heart failure, which may not be amenable to surgical repair and may become refractory to medical therapy.4–6 Individuals with long-standing haemodynamic lesions, ventricular dysfunction or pulmonary hypertension may develop heart failure refractory to conventional therapies and should be considered for heart or heart-lung transplantation.7
While transplantation has been available to patients with CHD for many years, the number of individuals who receive transplantation has not risen in parallel with increasing demand.8 9 Indeed, patients with CHD are less likely to receive a transplant or mechanical circulatory support.10 11 Only 1.9%–3% of heart transplants are performed in adults with CHD.12 13 Beyond the scarcity of donors, there are challenges in timing transplant referrals in CHD and in preparing patients to increase survival on the waiting list and around the time of transplantation. Perioperative risk is increased in patients with CHD and relates to the need for extensive vascular reconstruction and long ischaemic times.7 14 15 Human leucocyte antigen (HLA) sensitisation due to previous surgery, skeletal abnormalities, pulmonary vascular disease, right ventricular failure after lung transplantation in patients with pulmonary hypertension, pulmonary venous stenoses and the need for pulmonary artery reconstruction (in patients with a Fontan-type surgery), removal of baffles in patients with atrial switch repair for transposition of great arteries and atrial isomerism requiring redirection of systemic venous flow are further examples of why transplantation in patients with CHD is not straightforward.8 15 Patients with advanced heart failure and chronic systemic venous congestion are likely to present with multiorgan failure, including renal and liver failure or cirrhosis.16 The latter is not infrequent in patients with a Fontan circulation, in whom combined heart-liver transplantation may be required.17
We assessed the number of heart and heart-lung transplants performed in England over the last 17 years, the perioperative, mid-term and long-term survival, and predictors of outcome between demographic and clinical data, including socioeconomic status. Moreover, we present a 10-year forecast of the number of CHD transplantations.
Methods
Retrospective analysis of the Hospital Episode Statistics (HES) database for England from 1997 to 2015 was performed. Patient events can be tracked for each patient under the National Health Service (NHS) in England. Data recorded for patients admitted to hospital include up to 20 most relevant diagnoses for the hospital episode, coded using the 10th revision of the International Classification of Diseases system (ICD-10), and the type of treatment using the ‘Office of Population Censuses and Surveys’ (OPCS-4) procedural classification. We identified all patients who underwent heart (OPCS-4 code ‘K02’) or heart-lung transplantation (‘K01’). We used the ‘I50’ ICD-10 code to identify patients admitted with heart failure. Also, patients with a congenital diagnosis but no primary lung diagnosis (eg, cystic fibrosis) who underwent lung transplantation were identified but were not the focus of our study. Patients undergoing transplantation from all units performing CHD transplant in England were included: Great Ormond Street Hospital for Children, Harefield Hospital in London, Papworth Hospital in Cambridge, University Hospitals Birmingham NHS Foundation Trust, University Hospital of South Manchester and Freeman Hospital in Newcastle. The HES data set does not include information from Scotland; patients from the Golden Jubilee National Hospital in Glasgow were not included in this study.
A principal diagnosis was determined for every patient and classified according to the 32nd Bethesda Conference document on CHD complexity. Data on mortality and cause of death were retrieved from the UK Office for National Statistics. Anonymised data are available for research purposes and access to the database was granted for this project by the Health and Social Care Information Centre and requires no formal ethics approval.
Statistical analysis
Statistical analyses were performed using R-package V.3.2.2 (R Foundation for Statistical Computing, Vienna, Austria). Continuous variables are presented as mean±SD or median (range). Categorical variables are presented as number and percentage. Comparison between groups was performed using the Wilcoxon rank-sum test for continuous variables and Χ2 test for categorical variables. To assess whether the change in the number of transplants over time was significant, we used a generalised linear model (Poisson) for modelling stationary count time series. This model accounts for autocorrelation by using lagged values of the dependent variable in the systematic component.18 19 The Kaplan-Meier method was used for assessing survival following first transplantation. Differences in survival were assessed using log-rank test, while Cox proportional hazards analysis was used to assess whether any of the following parameters were associated to all-cause death: age, gender, ethnicity, socioeconomic status, CHD complexity, type of transplantation (heart vs heart-lung), surgical era (prior to or after 2006), diabetes and hypertension. An autoregressive integrated moving average (ARIMA) model was used to produce a forecast of the number of transplantations in patients with CHD over the next 10 years. The auto.arima and forecast functions in the R package ‘forecast’. The model was checked by plotting a correlogram of the forecast errors and using the Ljung-Box test. A two-sided p value <0.05 was considered indicative of statistical significance.
Results
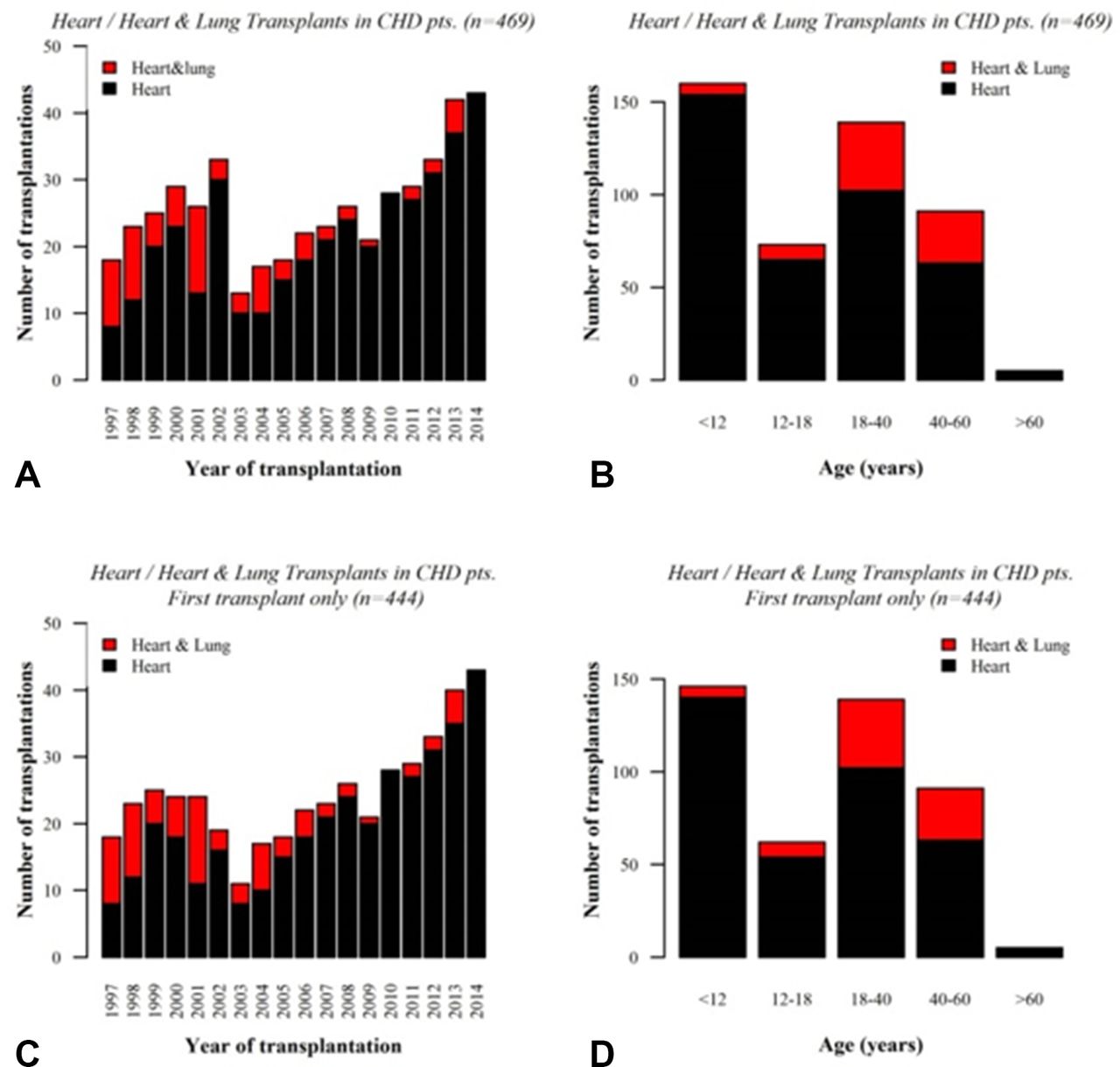
During the study period, 469 transplants were performed in 444 patients, of which 390 (83.2%) were heart and 79 (16.8%) were heart-lung (figure 1). When examining only the first transplant, 365 (82.2%) were heart transplants and 79 (17.8%) heart-lung (table 1). Median age at transplantation was 19.5 (0–63.6) years and was higher for patients with heart-lung compared with heart transplantation (p<0.0001). There was an almost equal split between paediatric and adult transplants (46.8% vs 53.2%) (table 1). Approximately one-half of recipients were male (52.9%) overall, but females were more likely to receive heart-lung transplantation compared with males (23.9% of females vs 12.3% males received a heart-lung transplant, p=0.002). The ethnic origin of most recipients was ‘white’, with no ethnic differences between heart and heart-lung transplantation. There were also no differences in terms of socioeconomic deprivation. As expected, the majority of patients had CHD of great (53.8%) or moderate (24.1%) complexity. Moreover, CHD complexity was greater in patients who underwent heart-lung transplantation: 92.4% of heart-lung recipients versus 45.5% of heart recipients had complex CHD, p<0.0001. The proportion of transplantations performed on patients with CHD of less than great complexity has increased over time (p=0.001). Until 2006, 63.4% of transplants were in patients with CHD of great complexity and this proportion decreased to 47.6% after 2006. In 2014, 58.1% of transplants were in patients with mild or moderate CHD complexity.
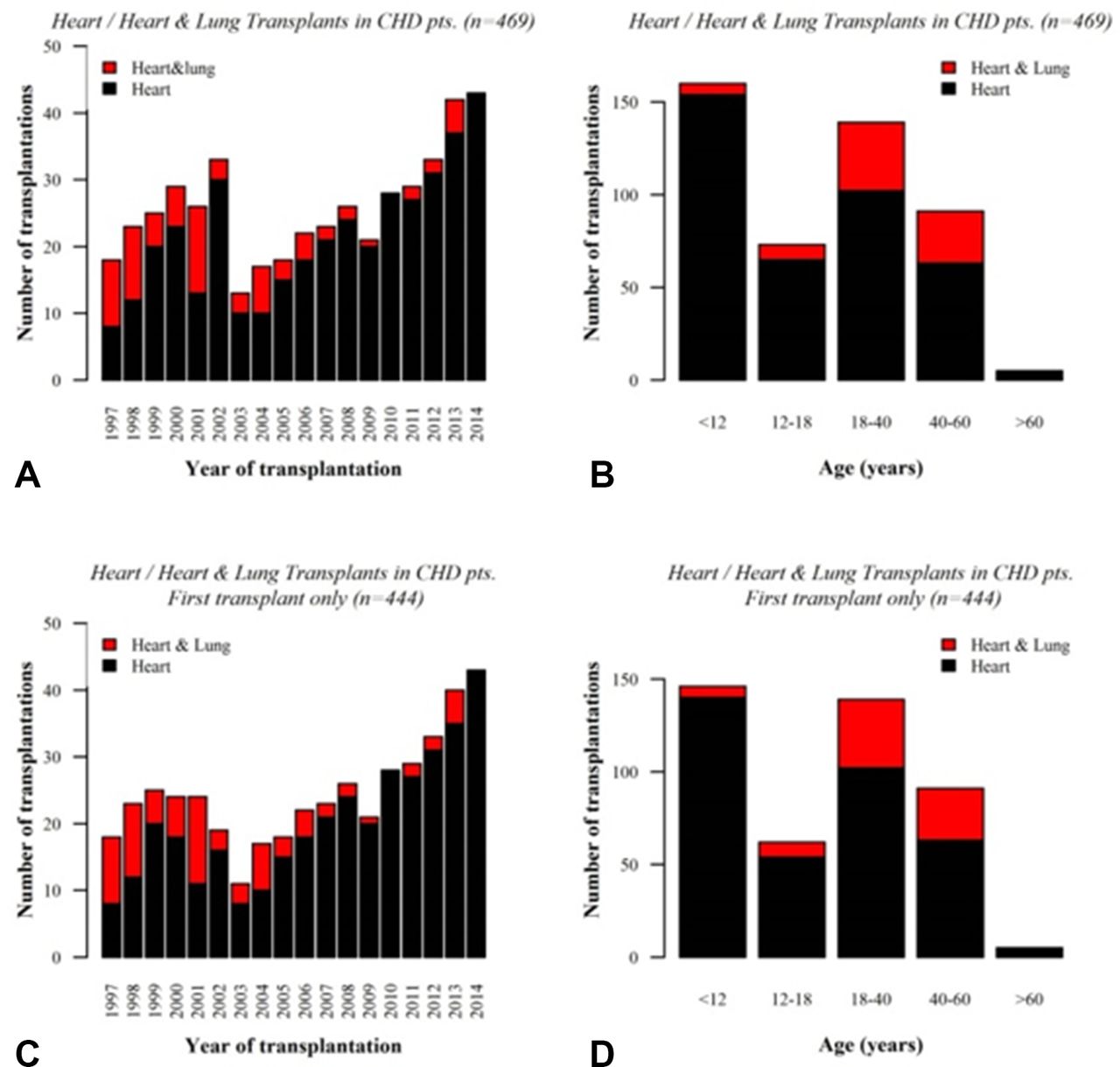
Number of heart and heart- lung transplantations by transplantation year and age at transplantation. The overall number of transplants (A, B) and first transplants only (C, D) is shown. There was a gradual increase in the overall number of heart or heart- lung transplantations between 1997 and 2014, with a peculiar dip around 2003 (A, C) and an apparent decline in the proportion of heart- lung transplantations over the study period. The majority of transplants were performed in adults, followed by children below the age of 12 years (B, D). CHD, congenital heart disease.
Baseline characteristics at first transplantation
The number of transplantations decreased around 2003, but then steadily increased over the next several years. The Poisson model fit for the number of transplantations over the years suggests there is a significant lagged dependence (p<0.0001), i.e., present transplant numbers significantly depend on past numbers. A greater number of heart-lung transplants were performed before 2006: of 269 transplants performed on or after 2006, 6.7% were heart-lung, whereas of 175 transplants performed pre-2005, 34.9% were heart-lung (p<0.0001). There was also no significant increase in the proportion of adult CHD transplants compared with paediatric ones over time (56.6% were performed in over 18 year-olds before 2006 and 50.9% in or after 2006, p=0.28).
An increase by approximately one-third in the number of heart or heart-lung transplants is predicted for the next 10 years, should the current trend persist (figure 2A). However, only 52 transplants are predicted nationally in the year 2020, even though the CIs are wide and reflect a high level of uncertainty in the prediction based on previous years. We also plotted the number of transplants per year (figure 2B, red line) against the number of patients admitted at least two (green line) or four times (blue line) over a 2-year period between 2004 and 2014 with a diagnosis of heart failure, many of whom are likely to become candidates for transplantation. This graph demonstrates that the increase in CHD transplants lags well behind the increase in the number of patients with CHD who develop advanced heart failure.
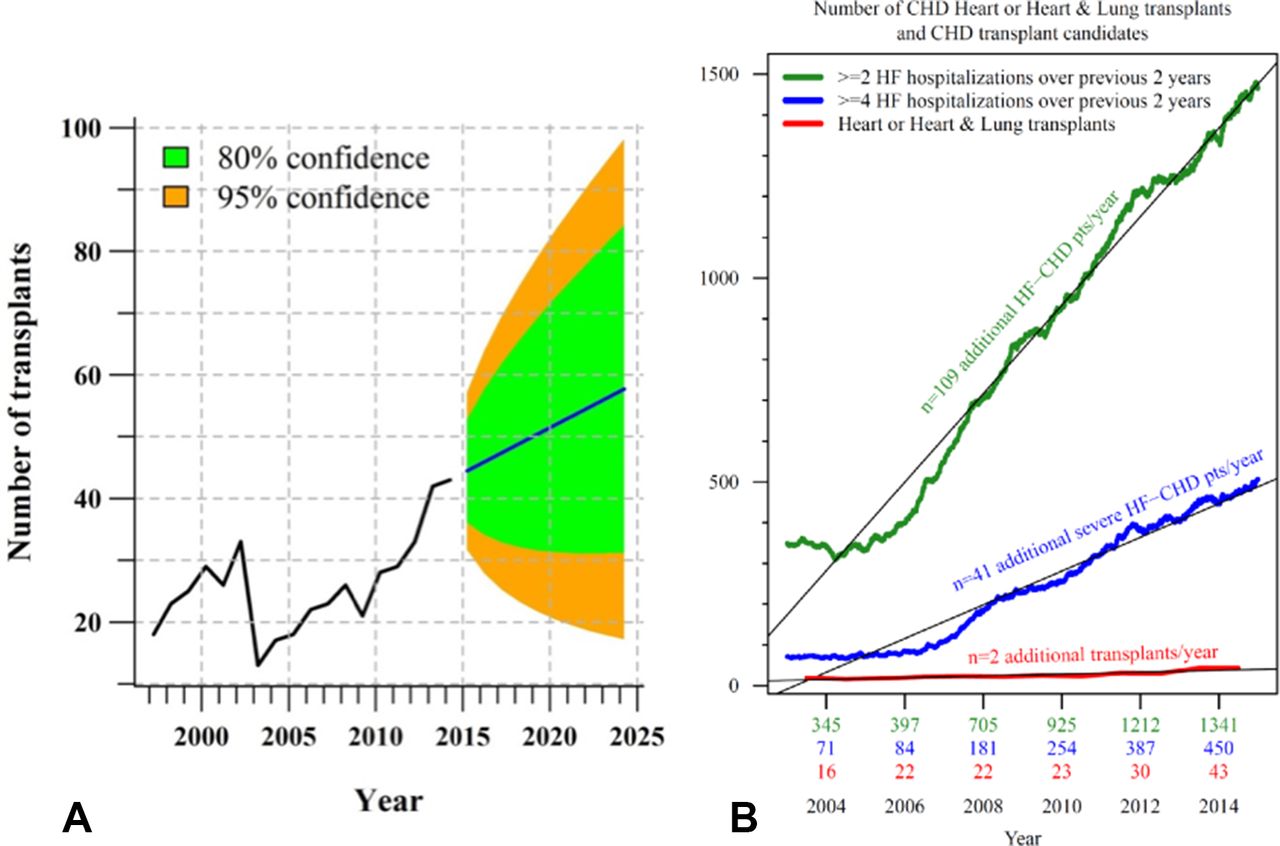
(A) Forecast of the number of transplants performed in CHD over the next 10 years in England (blue line), with 80% and 95% CIs (green and orange, respectively, ARIMA model). A steady increase is forecast based on previous years, even though only just over 50 heart or heart-lung transplants are predicted by year 2020. (B) Comparison between the number of patients with CHD hospitalised at least two (green) or four times (blue) within 2 years between 2004 and 2014 with a diagnosis of heart failure, compared with the number of CHD transplants, demonstrating a clear discrepancy between demand and availability. ARIMA, autoregressive integrated moving average; CHD, congenital heart disease; HF, heart failure.
Survival and predictors of all-cause death after transplantation
In the overall heart and heart-lung transplant population (first transplant only, n=444), over a median (IQR) follow-up of 4.6 (1.3–9.5) years, 130 patients died. Of these, 58.5% had CHD of great complexity, and 32.3% had undergone heart-lung transplantation. Survival at 30 days, 6 months, and 1, 5 and 10 years for heart transplant recipients was 89.3%, 87.1%, 85.7%, 78.9% and 73.2%, whereas for heart-lung transplantation this was 81%, 70.9%, 69.6%, 61.8% and 45.2%, respectively (figure 3A). There was no significant difference in 30-day mortality between patients with complex CHD versus those with CHD of mild or moderate complexity who underwent heart transplantation (15 (9.0%) vs 24 (12.1%), p=0.4).
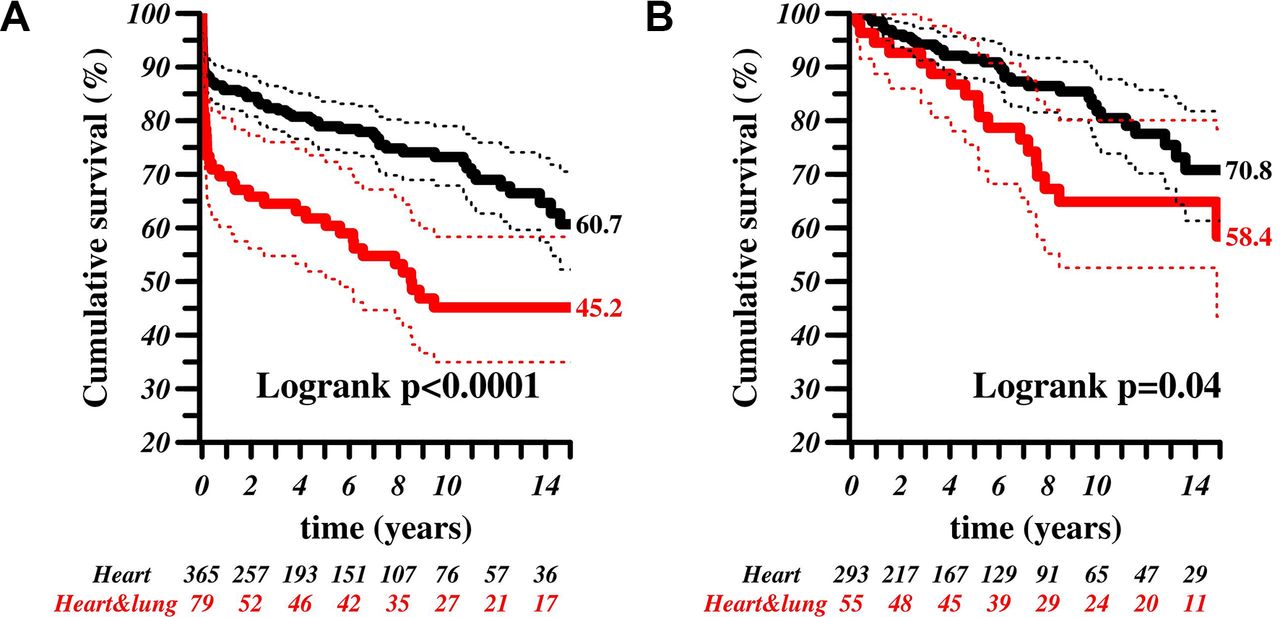
Kaplan-Meier curves depicting survival according to type of transplant (A) and conditional survival after 1 year by type of transplant (B). As expected, patients with heart-lung transplantation had a significantly worse survival compared with heart transplant recipients. Mortality was highest in the first year after transplantation (A) and remained low thereafter (B), especially for heart transplantation.
Univariate predictors of all-cause death in this population were older age (per 10-year increment HR 1.18, 95% CI 1.07 to 1.3, p=0.0007), heart-lung transplantation (HR 2.08, 95% CI 1.43 to 3.00, p=0.0001, figure 3A) and transplantation prior to 2006 (HR 1.48, 95% CI 1.02 to 2.14, p=0.04). There was no evidence that CHD complexity was related to survival (HR 1.14, 95% CI 0.8 to 1.62, p=0.46, figure 4A,C). Patients undergoing transplantation in adult life had an 80% higher hazard of dying compared with children (HR 1.82, 95% CI 1.27 to 2.62, p=0.01, figure 4B). On multivariate analysis, age and the type of transplant remained in the model. When analysing heart transplants only (first transplant only, n=365), age was the only predictor of outcome (per 10-year increments HR 1.14, 95% CI 1.02 to 1.28, p=0.02), with adults having a 72% higher hazard of death (HR 1.72, 95% CI 1.13 to 2.63, p=0.01).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Kaplan-Meier curves depicting overall survival after transplantation (A–D) according to complexity of the congenital defect (A) and age of the patients (adult vs child) (B). Moreover, survival beyond 1 year from transplantation according to congenital defect complexity (C) and age at transplant (D) is shown. Patients with congenital heart disease (CHD) of different severity did not demonstrate a difference in survival after transplantation. Adult patients with CHD had a significantly worse outcome than children, but the difference in mortality was concentrated in the first year from transplantation, with no significant difference thereafter.
Predictors of mortality beyond the 30 days from transplantation were also assessed: age (per 10 years HR 1.13, 95% CI 1 to 1.29, p=0.05) and transplant type (HR 2.22, 95% CI 1.38 to 3.56, p=0.001) were predictors of outcome. In heart recipients, none of the parameters assessed were predictive of outcome. Cumulative survival after the first year from transplantation for heart versus heart-lung (log-rank p=0.04) and children versus adults (p=0.19) is shown in figures 3B and 4D, respectively.
Discussion
The number of patients with CHD who have received heart or heart-lung transplantation in England has increased significantly in the last two decades, but this and the forecast increase are lagging well behind the exponential increase in the number of adult survivors. The numbers of heart-lung transplantations remain extremely low, greatly due to the scarce availability of donors. This re-enforces the value of early diagnosis and defect repair or transplant listing before pulmonary vascular disease develops. While mortality is high within the first year of transplantation, especially in heart-lung recipients, it remains relatively low thereafter, emphasising the importance of perioperative care in improving outcomes.
Transplant numbers in CHD recipients have remained low over time (figure 2), while the need is increasing. Paediatric patients with complex CHD (eg, ‘hypoplastic left heart syndrome’) are benefitting from advances in surgery and are surviving into adolescence and adulthood. Adult patients with CHD with a ‘failing Fontan’ circulation present a particular challenge to physicians, as therapeutic options are limited and multiorgan involvement complicates management, may contraindicate transplantation or may warrant two-organ transplantation (eg, heart-liver or heart-kidney). Even patients who have benefitted from biventricular repair for conditions such as tetralogy of Fallot and those with a systemic right ventricle often present in adult life with symptoms and signs of heart failure, which may be related to residual haemodynamic lesions or ventricular dysfunction. Systolic and especially diastolic dysfunction of the right and/or left ventricle can be difficult to treat, increases the risk of conventional surgery and is often the cause of recurrent hospital admissions. The chronicity of CHD, often an indolent process as opposed to the acute nature of other end-stage cardiac diseases, such as myocarditis, is likely to impact on recipient selection. Criteria used for transplantation listing may disadvantage patients with CHD. Some have advocated for separate prioritisation criteria for patients with CHD.
We observed a threefold increase over time in the number of patients with CHD with recurrent hospitalisations for heart failure, many of whom are likely to be considered for transplantation as they become refractory to medical therapy. The increase in the number of transplants in the same period was significantly smaller and may be due to reduced availability of donors, although other factors may significantly impact the number of patients with CHD being listed and transplanted. HLA sensitisation from previous blood transfusions, operations or pregnancies is common and leads to longer waiting times while increasing the risk of rejection and primary graft failure. Anatomical complexity requiring reconstruction of several structures (eg, in Fontan patients, those with transposed great vessels or with systemic venous anomalies) requires intraoperative CHD expertise or extra donor tissue and can prolong ischaemic times. Menachem et al 20 have recently reported a 100% 30-day survival in a cohort of 20 patients with CHD who underwent heart, heart-lung or heart-liver transplantation.20 This highlights the importance of involvement of adult CHD specialists in every stage of the transplant process and adult CHD surgeons supporting transplant surgeons. Over the last 15 years, the use of VADs has increased exponentially. This is not the case in patients with CHD where VADs are less used, reducing their chances of surviving on the waiting list.8
Only half of patients transplanted in our study had CHD of ‘great’ complexity. While counterintuitive, the increase in transplants performed in patients with ‘less complex’ CHD reflects the adult CHD experience: Simpler lesions with long-standing ventricular overload, recurrent surgery or genetic predisposition (eg, Noonan syndrome cardiomyopathy) often result in refractory heart failure. As a result, CHD complexity did not predict mortality after transplantation. Age was the strongest predictor of all-cause death in this population and is well described.21 The lack in gender and socioeconomic differences in outcome after transplantation is reassuring. The latter is likely to reflect the nature of the English healthcare system, which is free at the point of delivery and minimises inequalities in access to care.
Over the past 18 years, we found that the number of heart-lung transplantations in England has gradually reduced in line with the global trend.22 In patients with CHD, heart-lung transplantation is challenging and is therefore an unattractive option, especially in those with multiple prior operations, in the presence of collateral vessels and in patients with cyanosis, who have a higher risk of coagulopathy. There is an increasing demand in transplant recipients, but a scarcity of donors, leading to stricter selection criteria for heart-lung transplantation. There is also the ethical dilemma of using multiple organs in a single patient, when two patients could benefit from separate heart and lung transplants.
One of the most common indications for heart-lung transplantation in patients with CHD is Eisenmenger syndrome. While very limited functionally, adult patients may survive for decades after diagnosis and are currently felt to have better survival prospects without transplantation. Indeed, almost 90% of transplants on patients with Eisenmenger syndrome in our population were performed before 2005, with very few occurring in recent years. The introduction of advanced therapies for pulmonary arterial hypertension may have deferred transplantation in these patients. Long-standing low cardiac output, cyanosis and recurrent episodes of congestive heart failure eventually lead to refractory heart failure. In some patients, lung transplantation plus repair of the intracardiac defect could be considered. Optimal timing and selection criteria for transplantation in this population remain challenging.
The number of patients with CHD requiring heart transplantation will increase in the coming years. The mismatch between the number of patients with CHD requiring and receiving transplantation is due to the limited organ donor pool, an inherent limitation of transplantation shared across disease subgroups. Resourceful public health commissioning is required to promote organ donation to tackle this imbalance. Although there was an apparent reduction in heart transplants up to 2003, there has been a gradual increase over the last decade. To deal with this rise, there is a need to develop highly experienced multidisciplinary teams, including specialist CHD clinicians and surgeons. These ‘adult CHD transplantation teams’ should be established nationally to ensure higher volumes and quality and better training and succession.
With fewer than 200 heart transplants performed in the UK per year, there is a need to increase heart transplantation activity by other means, for example, by using hearts from donors after circulatory death and to increase the use of ventricular assist devices (VAD) in patients with CHD. The short-term results of durable left ventricular assist device (LVAD) support now rival heart transplantation, but medium and long-term results do not. If this changes in the future, the use of LVADs as destination therapy may replace heart transplantation for many forms of heart failure. Although the use of LVADs in non-congenital patients has increased over the last few years, this is not reflected in the CHD population. Recent data from the Interagency Registry for Mechanically Assisted Circulatory Support registry have shown similar outcomes between non-CHD patients and patients with CHD with a biventricular circulation requiring LVAD, independent of systemic ventricular morphology. Options for patients with biventricular failure are limited.23 The only Food and Drug Administration-approved total artificial heart is a pneumatically driven device for temporary use (bridge to transplant) based on technology that is more than three decades old. Additionally, the mortality is higher in patients with CHD requiring biventricular assist devices.23 Finally, novel forms of mechanical support need to be developed for patients with univentricular circulations.
Limitations
This is a retrospective study based on recorded hospitalisation events from a national database. A full congenital diagnosis and other clinical information beyond what is presented here is not available for analysis. Statistical prediction of the future number of transplants depends heavily on previous trends and suffers from a high degree of uncertainty. Our data, nevertheless, highlight the significant need for ongoing investment in transplant programmes for patients with CHD to accommodate the increasing demand.
Conclusions
The current and projected increase in capacity for CHD transplantation does not appear to parallel the ongoing expansion of patients with CHD, with increasing numbers presenting with heart failure. Additional investment in adult CHD transplantation seems necessary to ensure such effective therapy for ‘end-stage’ CHD, addressing increasing numbers and anatomic complexity, and optimising short and long-term outcomes of transplantation, whether heart or heart-lung.
Key messages
What is already known on this subject?
Patients with congenital heart disease (CHD) are less likely to receive a heart transplant or mechanical circulatory support.
Transplantation is technically challenging in this population and there is a higher perioperative mortality.
What might this study add?
This study provides a contemporary assessment of the number of heart and heart-lung transplants performed in the CHD population of England over the past 17 years until 2015.
We report on the post-transplantation survival in this cohort of patients and identify age and transplant type as predictors of outcome. Finally, we present a forecast of the number of CHD transplants required over the next decade.
How might this impact on clinical practice?
By exploring the specific barriers facing this group of patients, we highlight the need for collaboration between transplantation services and experienced CHD multidisciplinary teams, specialised CHD clinicians and surgeons.
The current and future expansion of the population of patients with CHD requiring heart or heart-lung transplantation must be met by resourceful public health commissioning to increase the donor pool.
References
Footnotes
KD and KM contributed equally.
Contributors Substantial contribution to the conception and design of the work: KD, AK. Acquisition, analysis and interpretation of data for the work: KD, AK, RAG, AHC. Drafting the manuscript and critical appraisal: KD, KM, RAG, NRB, SJW, LS, AHC, MAG, GPD, AK. Final approval of the published version: KD, KM, RAG, NRB, SJW, LS, AHC, MAG, GPD, AK. Guarantor: KD.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Disclaimer No sponsor played any role in the design and conduct of this study, including in data collection, analysis, data interpretation, and in the preparation, review or approval of the manuscript.
Competing interests MAG and the Royal Brompton Hospital Adult Congenital Centre and Centre for Pulmonary Hypertension have received support from the British Heart Foundation. MAG, GPD and KD acted as consultants for Actelion UK, Pfizer UK and GSK UK and received unrestricted educational grants from Actelion and Pfizer. RAG acted as consultant for Lilly Spain and Pfizer Spain. AK has received an unrestricted research grant from Actelion Global. SJW has received unrestricted educational and research grants from Bayer UK, Pfizer UK, Actelion UK and GSK UK as well as the Pulmonary Hypertension Association (UK).
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Not required.