Article Text

Abstract
The management of atrial fibrillation (AF) has focused on anticoagulation, rhythm control and ventricular rate control. Recently, a fourth pillar of AF management has been incorporated recognising the importance of risk factor management (RFM). There are several risk factors that contribute to the development and progression of AF, these include traditional risk factors such as age, hypertension, heart failure, diabetes and valvular heart disease. However, increasingly it is recognised that obesity, sleep apnoea, hyperlipidaemia, smoking, alcohol, physical inactivity, genetics, aortic stiffness are associated with the development of AF. Importantly, several of these risk factors are modifiable. We have seen the evolution of RFM programmes which have demonstrated promising results. Indeed, the evidence is now so compelling that major clinical guidelines strongly advocate that aggressive treatment of these risk factors as a key component of AF management. Patients with AF who comprehensively managed their risk factors demonstrate greater reduction in symptoms, AF burden, more successful ablations and improved outcomes with greater AF freedom. In this article, we will review the evidence for the association between cardiac risk factors and AF and assess the burgeoning evidence for improved AF outcomes associated with aggressive cardiac RFM.
- atrial fibrillation
- hypertension
- metabolic syndrome
- smoking cessation
- obesity
Statistics from Altmetric.com
Introduction
Atrial fibrillation (AF) is the most common cardiac arrhythmia. A diagnosis of AF is associated with a 1.5-fold to 2-fold increase in all-cause mortality with a further significant impact on morbidity (heart failure and ischaemic stroke) and risk of hospitalisation.1 The economic burden of AF is therefore huge, contributing to around 1% of total healthcare expenditure. It is therefore imperative we implement new strategies to manage this chronic condition.
Risk factors associated with AF
Strong epidemiological evidence suggests that the risk factors associated with the development of AF are remarkably similar to those of other chronic cardiovascular conditions such as coronary artery disease. For coronary artery disease, it has long been established that good management should involve careful management of risk factors, including good blood pressure, glycaemic control, weight management and smoking cessation. The idea that these same risk factors may also contribute to AF is relatively novel. Furthermore, there is a growing understanding of the basic science mechanisms underlying these associations, through animal and human studies.
Obesity
Epidemiological studies have demonstrated a clear correlation between obesity and AF. Risk of incident AF has been shown to increase up to 29% with every 5-point increase in body mass index (BMI).2 Significant weight loss is associated with a much reduced risk of incident AF development.3
The link between obesity and AF is likely multifactorial. Animal studies have revealed that the atria demonstrate significant conduction slowing, increased conduction heterogeneity and electrogram fractionation, all of which create the electrophysiological milieu for AF.4 5 In the clinical setting, obese individuals have been demonstrated to have significantly increased left atrial (LA) pressure and volume,6 and altered electroanatomic features in areas contiguous with pericardial fat.7 Obesity is also known to significantly alter circulatory haemodynamics, creating a high cardiac output state conducive to structural remodelling of the heart,8 and results in an increase in the central blood volume as well as increased systemic vascular resistance which increase left ventricular wall stress causing hypertrophy and diastolic dysfunction. This results in LA enlargement, which is known to be a potent independent predictor of AF.9 Another mechanism through which obesity or fat deposition may contribute to the development of AF is through the direct communication between epicardial fat and the LA. Obesity is associated with increased epicardial and pericardial fat deposition. Individuals with increased volumes of pericardial fat are more likely to develop AF.10 Furthermore, AF is likely to be more severe, both in terms of severity of symptoms and persistence, and less responsive to catheter ablation.10 The pathophysiology underlying this observed phenomenon is not fully understood currently but has been postulated to be related to fibrotic remodelling of the LA due to either direct fatty infiltration of the LA or paracrine effects of adipose tissue releasing cytokines or chemokines.11
Hypertension
The atherosclerosis risk in communities study showed that elevated blood pressure was the most important determinant, contributing to 20%–25% of all AF.12 The mechanisms underlying this association relates to both haemodynamic alterations and activation of the renin-angiotensin-aldosterone system. In similar fashion to the haemodynamic changes seen in association with obesity, hypertension causes increased ventricular afterload and results in left ventricular hypertrophy, LA enlargement and stiffness. The resultant diastolic dysfunction results in chronic LA stretch and dilatation. In addition, it is well known that hypertension increases levels of circulating angiotensin II. Angiotensin II has also been shown to induce atrial fibrosis and hypertrophy, increasing the risk of electrophysiological changes associated with the development of AF. Hypertension has been shown to be responsible for progression of atrial remodelling and the substrate therefore leading to AF.13–15 An early ovine study assessing a chronic hypertension model of 5 years found this resulted in significant conduction slowing, increase atrial fibrosis and evidence of cellular myolysis which in turn resulted in increase of AF.16 Similar changes have also been observed in patients with hypertension.17 Therefore, studies indicate that therapies targeting the substrate promote tight blood pressure control, is imperative in managing patients with AF.18 19
Obstructive sleep apnoea
Obstructive sleep apnoea (OSA) is a condition characterised by recurrent pharyngeal airway collapse leading to repetitive interruption of ventilation during sleep. Clinically, the condition presents with excessive daytime somnolence and treatment is with continuous positive airway pressure (CPAP). Risk factors for the development of OSA are like those for AF and include obesity, hypertension, heart failure, ageing and upper airway soft tissue abnormalities. Indeed, observational studies have suggested that OSA increases the risk of AF in a dose-dependent manner (increased severity OSA is associated with increased risk of AF).20 Furthermore, it has been shown that risk of AF recurrence after cardioversion or AF ablation is significantly increased in patients with sleep apnoea and treatment with CPAP can reduce this risk.20
It has been suggested that both the acute impact of short apnoeic spells as well as the chronic effects of long-term OSA contribute to the increased risk of atrial arrhythmogenesis. Short-term physiological changes occur with each apnoeic episode; large oscillations in intrathoracic pressures due to upper airway occlusion results in increased venous return, increased ventricular afterload and resultant increased LA pressures, leading to LA enlargement.20 The intermittent hypoxaemia seen in apnoeic episodes may also have an effect on atrial effective refractory period, thereby increasing atrial susceptibility to AF. The long-term AF-inducing effects of OSA include systemic inflammation, the development of a prothrombotic state and atrial fibrosis and electrical remodelling (decreased atrial voltage, slower atrial conduction velocity and more widespread complex electrograms).20 21 There is, therefore, epidemiological, clinical and mechanistic evidence for the causal relationship between OSA and AF.
Physical inactivity
It has been shown that the US sedentary rates have increased from 19% to 52% in women and 11% to 44% in men from 1988 to 2010.22 Physical activity has been widely reported to reduce cardiovascular disease incidence. Compared with sedentary, runners had a significantly reduced risk of 30% and 45% of all-cause and cardiovascular mortality, respectively.23 This reduction in risk was achieved by running as low as 5–10 min a day and slow speeds. Sedentary lifestyle has been shown to promote all risk factors for metabolic syndrome. Physical inactivity is known to promote obesity. It has been shown that early inactivity leads to subsequent obesity. Independent of obesity, physical activity predicts a lower risk of cardiovascular disease. Specifically for AF, greater levels of physical activity result in lowered incidence of AF.24 Importantly, physical activity has also been reported to diminish the risk associated with other notable risk factors such as obesity. The Nord-Trøndelag Health Study 3 (HUNT3) study showed that active individuals with obesity had a 22% lower risk of AF than those who were obese and sedentary, therefore suggesting physical activity seems to offset some of the risks associated with that of obesity and AF.25 The Cardiovascular Health Study highlighted that moderate-to-intense physical activity was associated with a 28% lower incidence of AF.24
Diabetes
Diabetes mellitus is another well-known cardiac risk factor. Evidence for an independent association between diabetes and AF is strong, although the studies available have significant limitations. Fibrotic change within the atria in diabetes has been demonstrated in animals and humans, while electrical remodelling also appears to be an important mechanism for the association. In particular, changes in the sodium current have been demonstrated within atrial myocytes of diabetic rabbits.26 In addition, expression of connexin 40 has also been demonstrated to be downregulated in a rat model of diabetes, resulting in slowed conduction velocities and heterogeneous conduction patterns.27 These changes likely contribute to increased susceptibility to AF in diabetes.
Smoking
The literature demonstrates that smoking results in an increase in sympathetic tone, inflammation, thrombus, endothelial dysfunction, atrial fibrosis and oxidative stress, which are potential mechanisms for the development of AF.28 The Framingham study demonstrated the risk of AF for males smokers was 1.0 (95% CI 0.8 to 1.4) and for females 1.4 (95% CI 1.0 to 2.0).29 The The Atherosclerosis Risk in Communities Study (ARIC) has shown more than a twofold increase in the incidence of AF for current smokers. The risk of AF reduced for those who were former smokers and similarly the risk of AF decreased in those who ceased smoking (HR 0.88; 95% CI 0.65 to 1.17).30
Alcohol
The mechanisms by which alcohol is attributed to the development of AF can be associated with direct cellular effects on atrial myocytes with acute oxidative stress and autonomic function by sympathetic activation and change in heart rate variability. Long-term alcohol consumption together with cardiovascular risk factors are responsible for LA remodelling and dilation, with an increase in LA pressure and fibrosis. There have been varied findings relating to the proarrhythmogenic influence of alcohol intake, likely due to significant heterogeneity methods acquired for measuring and reporting alcohol intake. A meta-analysis of the literature showed based on alcohol intake those with high consumption had an increased risk of AF (HR 1.34, 95% CI 1.20 to 1.49, p<0.001), for moderate intake the risk of AF was increased for males but not females (HR 1.26, 95% CI 1.04 to 1.54, p=0.02 and HR 1.03, 95% CI 0.86 to 1.25, p=0.37), respectively. For low alcohol intake there was no associated risk of AF.31 A recent publication has demonstrated regular moderate alcohol consumption was associated lower atrial voltage and conduction slowing suggesting these electrical and structural changes may explain AF at this level of consumption.32 These studies while heterogeneous do demonstrate a direct influence of alcohol as a risk factor for the development of AF.
AF risk factors and lifestyle
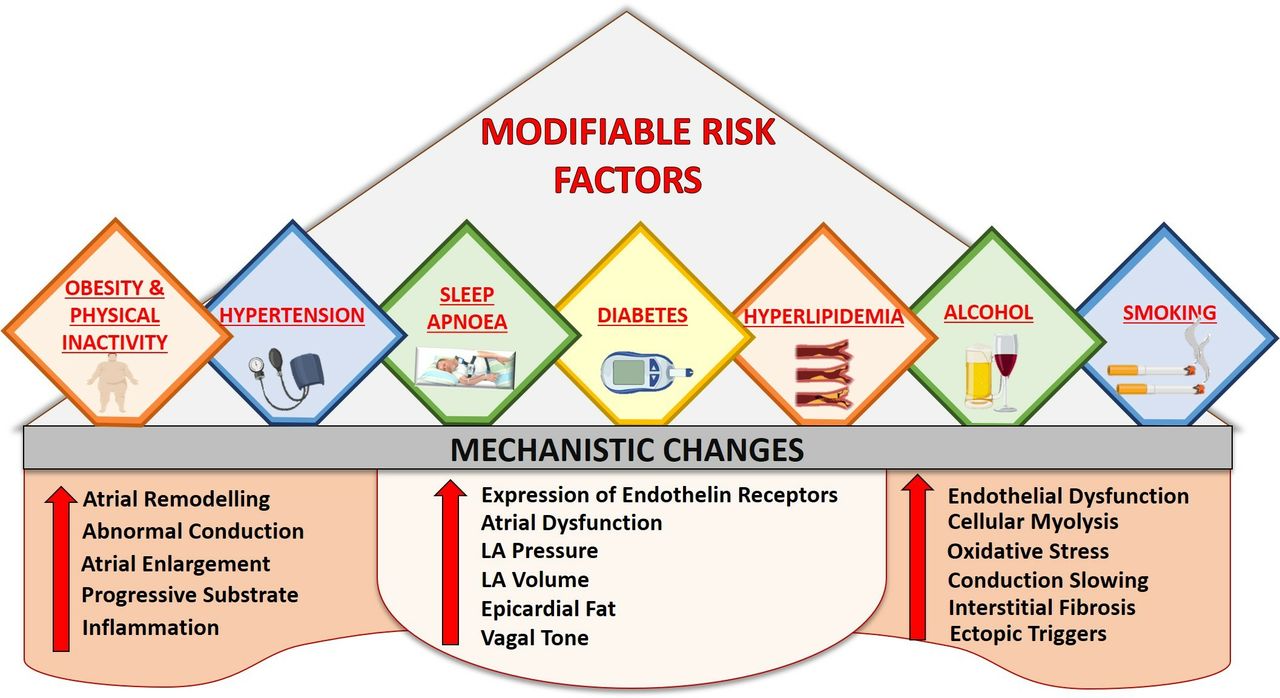
One common characteristic of these modifiable risk factors is that lifestyle factors play an important role in their development. Given the now established association between these risk factors and AF, it stands to reason that lifestyle modifications have a significant impact on management of AF (figure 1). Several studies (table 1) have now demonstrated that lifestyle changes have the potential to reduce AF symptoms but also reverse its natural progression and improve overall quality of life.

Modifiable risk factors: there are several modifiable risk factors that contribute to the development of atrial fibrillation. These risk factors result in several mechanistic changes. LA, left atrial.
Current studies on risk factor modification and atrial fibrillation
Supplemental material
Method of lifestyle and risk factor management delivery
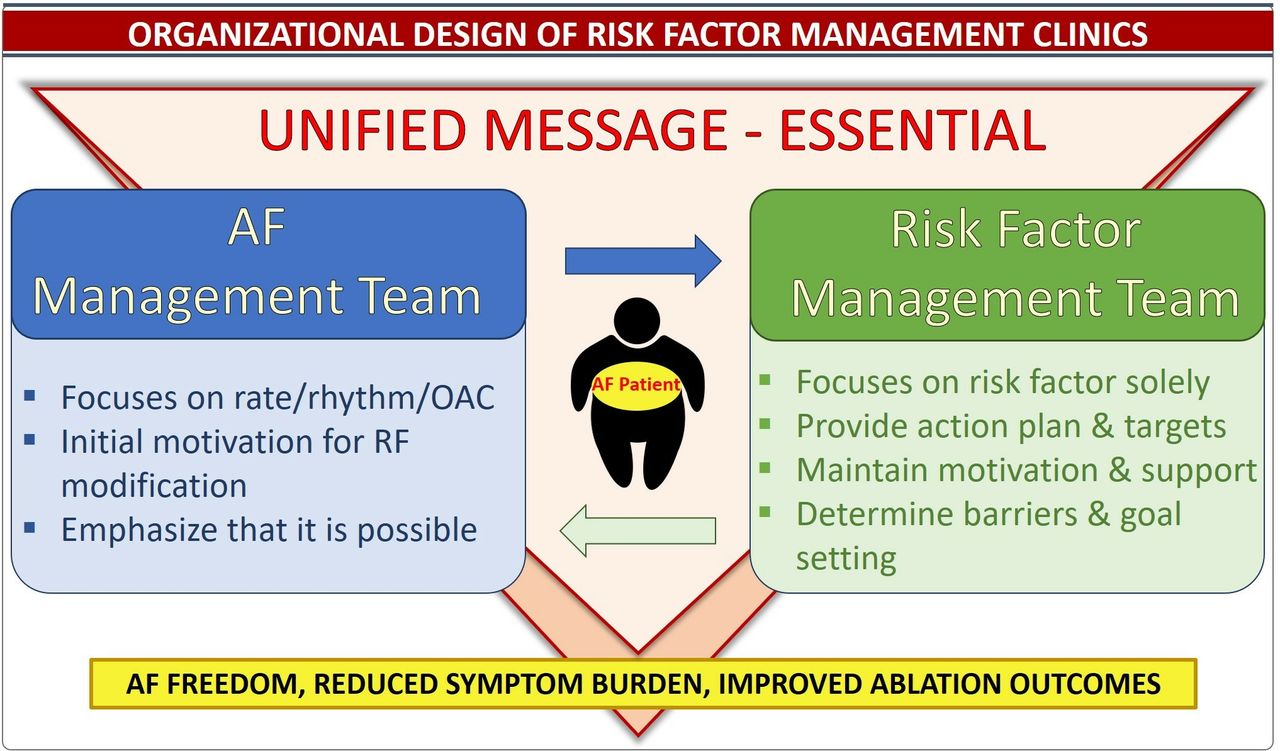
Several approaches could be used to achieve lifestyle and risk factor management (RFM) in patients with AF. In the management of AF, to date, a dedicated risk factor clinic has been shown to yield the most impressive results (figure 2). The programme focuses on all the primary modifiable risk factor targeting lifestyle and diet changes to achieve outcomes based on each individual patient’s particular risk factors (figure 3). This begins with personalised assessment with patients maintaining a lifestyle journal, recording food intake and exercise (figure 4). This is reviewed, and recommendations based on the patients current diet to gradually promote a diet of high protein, low glycaemic index with calorie restriction and portion control. Sodium restriction is encouraged particularly in patients with hypertension. Individuals are encouraged to exercise up to 30 min 3–4 times a week with an aim to increase this up to 200 min a week. All patients with AF undergo sleep studies to evaluate if this risk factor is a causative factor, with CPAP initiated if the Apnoea-Hypopnea Index (AHI) is >30. Hypertension is managed aggressively by patients recording this 2–3 times a day targeting <130/80 mm Hg 80% of the time on home readings. In addition, patients undergo a clinical stress test to ensure there is no exercise-induced hypertension with BP remaining <200/100 mm Hg. Patients are screened for hyperlipidaemia which is managed by lifestyle and dietary changes if this is not achieved then statins or fibrates are introduced. Diabetes is also managed with dietary and lifestyle changes with metformin introduced if haemoglobin A1c is >6.5%, patients are also referred to endocrinologist for management. Smoking cessation is encouraged as well as reduce alcohol intake to three standard drinks a week.33 As demonstrated in other chronic care models, in order to have a successful outcome it is important to change patient behaviour. This is done by targeting their specific risk factors, building a rapport, finding their individual motivations and working with them on behaviour change through achievable targets which then in turn become habitual practice (figure 5). These methods in achieving effective outcomes in patients with AF can be successfully managed with personalised education34 and an integrated care approach (figure 6).35

Organisational design of risk factor management clinics: successful organisational clinics rely on an atrial fibrillation (AF) management team working together with a risk factor management team, each focusing on their task but providing a unified message to the patient.OAC,oral anticoagulation.

Aggressive risk factor management targets: evaluation and management of each patient’s individual risk factors to set goals and targets for patients to achieve. ACEI, ACE inhibitor; ARB, angiotensin receptor blocker; BMI, body mass index; BP, blood pressure; CPAP, continuous positive airway pressure; HbA1c, haemoglobin A1c; HT, hypertension; LDL, low-density lipoprotein; OSA, obstructive sleep apnoea; TG, triglyceride.

Flow diagram of risk factor management (RFM): it is important to work through a process with the patient with atrial fibrillation (AF). Together with the AF management team, each step will achieve the final goal of risk factor management and sinus rhythm maintenance. AAD, anti-arrhythmic drugs.

Behavioural change: as demonstrated in other chronic conditions to follow instal behavioural change involves knowing the patient, setting a plan with achievable goals, with regular review to address setbacks and drive motivation resulting in eventual habitual change.

Integrated care approach: the fundamentals of integrated care involve four key elements. Patient involvement, multidisciplinary teams, technology tools and access to all treatment options for atrial fibrillation (AF). These are delivered by a team of healthcare practitioners who work closely with the patient to improve AF outcomes.
Impact of risk factor management on symptoms
A randomised clinical trial demonstrated that weight loss and RFM in overweight or obese individuals with AF, resulted in a dramatic reduction in patient symptoms and AF burden determined by ambulatory monitoring. In the group who underwent intervention with weight loss and lifestyle changes, there were significant improvements in patient well-being, blood pressure, glycaemic control and cholesterol.36
Impact of risk factor management on ablation outcomes
The Aggressive Risk Factor Reduction Study for Atrial Fibrillation (ARREST-AF) cohort study showed the benefits of RFM on the outcomes of AF ablation.37 This showed that AF frequency, symptoms and duration improve in the group undergoing RFM compared with the controls and there was more favourable ablation outcomes with 62% AF freedom in the RFM group compared with 26% in the control group following single procedure. This was replicated in multiple procedural outcomes with 87% in the RFM group and 48% in the control group free from AF at final follow-up. Additionally, AF freedom was demonstrated at follow-up with a stepwise improvement based on the degree of weight loss, with ≥10% weight loss associated with 46% AF freedom, compared with 13% in those who lost <3% weight without the use of anti-arrhythmic drugs or ablation.37
Long-term outcomes of risk factor management
In a prospective cohort study analysis, the Long-Term Effect of Goal-Directed Weight Management in an Atrial Fibrillation Cohort: A Long-Term Follow-Up Study (LEGACY) highlighted the importance of long-term weight loss and RFM.38 A stepwise reduction in weight resulted in a relative reduction in patient symptoms and overall AF burden. Importantly, in the group who lost ≥10% of their initial body mass, 46% patients remained free from AF without the use of rhythm control strategies over long-term follow-up of 5 years. Fascinatingly, LEGACY further showed the weight loss achieved must be maintained long-term; significant weight fluctuation (>5% annual change in weight) offset the benefits of overall weight loss and increased the risk of arrhythmia recurrence.
Role of exercise and risk factor management
Several studies have addressed the benefits of exercise and cardiorespiratory fitness in the management of AF. The Impact of CARDIOrespiratory FITness on Arrhythmia Recurrence in Obese Individuals With Atrial Fibrillation (CARDIO-FIT) study demonstrated that patients who achieved a cardiorespiratory fitness gain ≥2 metabolic equivalents (METs), significantly improved freedom from AF and alleviated AF-specific symptoms, when compared with those with <2 METs.33 Furthermore, gains of >2 METs in cardiorespiratory fitness obtained during the course (48 months) of the study were associated with a twofold (12%) increased chance of freedom from AF. A recent randomised trial also demonstrated reduced AF burden with aerobic interval training, alongside fewer hospital admission and cardioversions resulting in reduced AF symptoms, improved quality of life and peak oxygen uptake.39 These studies support the prescription of exercise in the management of AF.
Lifestyle modification reverses the natural progression of AF
Progression of AF from paroxysmal to persistent AF is associated with increased morbidity and mortality.40 Poorer outcomes attributed to persistent AF are associated with increased risk of ischaemic stroke in addition to worsened left ventricular function. Furthermore, as paroxysmal AF progresses to persistence, it becomes increasingly difficult to manage with lower success rates observed with rhythm control strategies (including invasive catheter ablation).41 Delaying the natural progression of AF may therefore be key to improving the long-term outcomes associated with AF.
The PREVEntion and regReSsive Effect of weight-loss and risk factor modification on Atrial Fibrillation (REVERSE-AF) study is seminal in providing evidence that RFM aimed at reducing weight by 10% has the potential to reverse this natural progression.42 This study showed that significant weight loss (≥10%) in patients with AF with BMI >27 kg/m2 was associated with less progression from paroxysmal to persistent AF and increased reversal from persistent to paroxysmal AF or no AF. This beneficial effect may be due to structural remodelling of the LA. In addition, treatment of OSA with CPAP in patients who have undergone AF ablation also results in atrial reverse remodelling and improved AF outcomes.43
Cost-effectiveness of risk factor management
Importantly, despite the expense of regular face-to-face counselling at RFM clinics, the Cost-Effectiveness and Clinical Effectiveness of the Risk Factor Management Clinic in Atrial Fibrillation (CENT) study confirmed the significant health economic benefits of such a strategy through reductions in the need for cardioversions, emergency department attendances, unscheduled specialist appointments, hospitalisations, ablation procedures and additional medications.44 Overall, the study showed that the cost-saving per patient in the RFM group reached US$2968±US$498 which, when projected over a 10-year model, corresponded to a total healthcare saving of US$12 094.
Additional studies addressing risk factors for AF
The Substrate Modification with Aggressive Blood Pressure Control for Atrial Fibrillation (SMAC-AF) study looked at the impact treatment in aggressive management of blood pressure would have in the reduction of AF symptom burden and prevent recurrence following ablation. Following ablation and the aggressive treatment of modest hypertension, there was no reduction in AF in patients with a BP >130/80 mm Hg, and they found that the aggressive treatment consequently resulted in more hypotension.45 This study demonstrated no real reduction in recurrence of AF, potentially due to only addressing one risk factor rather than all concomitant risks. In contrast, a study treating severe drug-resistant hypertension using renal artery denervation in conjunction with AF ablation, resulted in significant improved control of blood pressure and a significantly better control of AF.46 These findings suggest that perhaps in exaggerated forms of risk factors, managing an isolated factor may have a role.
Similarly, in a study which focused on weight loss and OSA as risk factors, it was demonstrated an intervention by a nurse resulted in significantly greater weight loss, resulting in less fluctuation, together with better referral to sleep study and compliance.47 However, they were not able to demonstrate significant change in other risk factors or AF type, freedom or management including ablation of AF.
In terms of other risk factor clinics, the Routine versus Aggressive upstream rhythm Control for prevention of Early AF in heart failure (RACE3) trial assessed cardiac rehabilitation in patients with AF focusing on pharmacotherapy.48 While not strictly a clinic which focused solely on risk factors, patients were provided general dietary and physical activity advice. This study demonstrated patients who were randomised to targeted therapy in the intervention group were more likely to be in sinus rhythm at final follow-up.
In patients with long-standing persistent AF with morbid obesity, a study evaluated the impact of weight loss in 90 patients.49 While there was significant weight loss over 12 months, they were unable to demonstrate improvement in symptoms, AF burden and ablation outcomes. This raises the possibility that prolonged morbid obesity or long-standing persistent AF (or both) may portend an irreversible substrate—‘too little too late’. However, a recent report of managing morbid obesity and predominantly patients with persistent AF using bariatric surgery has challenged this notion demonstrating significant improvement in maintenance of sinus rhythm after ablation.50
Conclusion
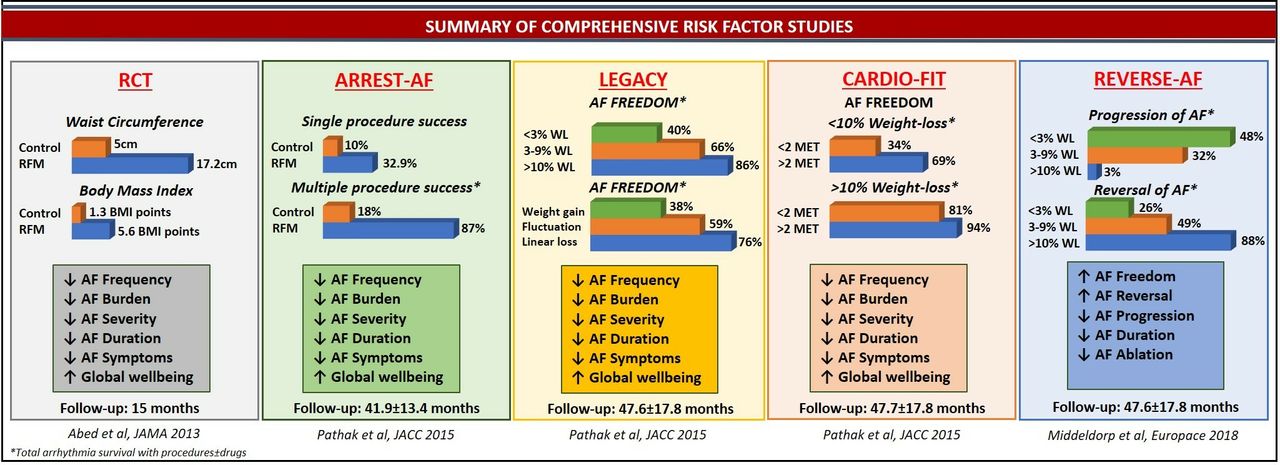
There is evidence to suggest that AF is a manifestation of systemic illness associated with an unhealthy lifestyle and poorly controlled risk factors. Traditional management of AF has focused on the sequalae of this systemic disease rather than the underlying causes. Several recently published studies (figure 7) have now shown evidence that aggressive management of these risk factors improves outcomes in AF and reverses the natural progression of AF. These new insights provide all clinicians with additional tools to improve individual and population outcomes in a significantly more cost-effective manner.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Overview of all comprehensive risk factor management clinics: this figure combines the results of studies which have undertaken a comprehensive risk factor programme highlighting the outcomes seen across the studies. AF, atrial fibrillation; RCT, randomised controlled trial; RFM, risk factor management; WL, weight loss.
References
Footnotes
Twitter @PrashSanders
Contributors All authors have contributed to the writing of the manuscript.
Funding MEM is supported by Postdoctoral Fellowships from the University of Adelaide. DL is supported by a Fellowship from the Hospital Research Foundation and by the Robert J Craig Lectureship from the University of Adelaide. PS is supported by Practitioner Fellowships from the National Health and Medical Research Council of Australia. PS are supported by the National Heart Foundation of Australia.
Competing interests DL reports that the University of Adelaide has received on his behalf lecture, travel and/or research funding from Abbott Medical, Bayer, Boehringer Ingelheim, Biotronik and Medtronic. PS reports having served on the advisory board of Medtronic, Abbott Medical, Boston Scientific, CathRx and Pacemate. PS reports that the University of Adelaide has received on his behalf lecture and/or consulting fees from Medtronic, Abbott Medical and Boston Scientific. PS reports that the University of Adelaide has received on his behalf research funding from Medtronic, Abbott Medical, Boston Scientific and Microport.
Patient consent for publication Not required.
Provenance and peer review Commissioned; externally peer reviewed.