Article Text

Abstract
Objective Left atrial (LA) thrombus is routinely excluded by transoesophageal echocardiography (TOE) before cardioversion for non-valvular atrial fibrillation (AF). In the D-dimer blood concentrations to exclude LA thrombus in patients with AF study, two D-dimer cut-offs were compared to exclude LA thrombus prior to cardioversion. One was fixed to 500 ng/mL (DD500), based on clinical practice where such values are commonly accepted to exclude a thrombus. The other cut-off was adjusted to 10 times the patient’s age (DDAge), based on the cut-off used to exclude pulmonary embolism.
Methods 142 consecutive patients with non-valvular AF aged 69.7±11.4 years (52% with paroxysmal AF) referred for precardioversion TOE to exclude LA thrombus were prospectively enrolled. D-dimers were measured at the time of TOE by an ELISA test.
Results LA thrombus was excluded with TOE in 129 (91%) and confirmed in 13 (9%) patients. D-dimers were significantly lower in patients without LA thrombus (729±611 vs 2376±1081 ng/L; p<0.05). DDAge indicated absence of LA thrombus with higher specificity than DD500 (66.4% vs 50.4%; p<0.05). Both cut-offs were able to identify all 13 patients with LA thrombus (false negative 0%). Patients with D-dimers <DDAge and without LA thrombus (true negative) represented 60.6% of the population and could have safely avoided TOE (flow chart).
Conclusions This study demonstrates the efficacy of D-dimer cut-offs to exclude LA thrombus in patients with AF. Age adjustment greatly increases the proportion of patients in whom LA thrombus can be safely excluded and consequently avoid precardioversion TOE.
- atrial fibrillation
- stroke
- echocardiography
Statistics from Altmetric.com
INTRODUCTION
Atrial fibrillation (AF) is the most common type of supraventricular arrhythmia occurring in 1%–2% of the general population, with increasing prevalence.1 To restore sinus rhythm, electrical cardioversion has proven to be the most rapid and effective method.2 Due to the potential thrombus presence in the left atrium (LA), cardioversion entails significant thromboembolic risk, persisting up to 10 days postcardioversion.3
Following current guidelines, efficient anticoagulation therapy for a minimum of 3 weeks or transoesophageal echocardiography (TOE) are necessary prior to cardioversion to minimise the thromboembolic risk in AF lasting for >48 hours.4 However, as TOE is a semi-invasive technique, it has several disadvantages. As TOE is operator-dependent and potentially incurs oesophageal lesions, the transmission of infectious disease by droplets and aerosols can occur.5–7 In precardioversion TOE, visualisation of LA thrombus is estimated to range between 8.5% and 12%.8–10
D-dimers are considered biological markers of coagulation activation and fibrinolysis.11 Their presence may indicate thromboembolic phenomena, such as pulmonary embolism (PE), deep vein thrombosis, acute coronary syndrome or aortic dissection.12–14 D-dimer levels increase with age, thereby decreasing the specificity (Sp) of cut-off values, especially in patients over 60 years of age.15 A correlation between D-dimer and the presence of LA thrombus in patients with AF has been described in various studies.16 17 However, to the best of our knowledge, an association between age-adjusted D-dimer and the absence of LA thrombus has not yet been investigated. The present study aimed to evaluate the use of age-adjusted D-dimer values to exclude LA thrombus in patients with AF to minimise precardioversion TOE. The secondary objective was to determine clinical criteria in patients with AF that may be useful in their predictive value for the presence of LA thrombus.
Methods
Population
Between August 2018 and September 2019, 142 consecutive patients with non-valvular AF were enrolled in the study. All patients were referred to the cardiology department of CHU Brugmann, Brussels or AZ Sint Jan, Bruges for cardioversion with prior TOE. All patients had a transthoracic echocardiography within 6 months before cardioversion. Blood was collected for D-dimer testing on the same day of the TOE. A follow-up visit was scheduled 1 month after cardioversion and included a clinical examination and an ECG. Exclusion criteria were as follows: age below 18 years or above 90 years, moderate and severe valvular heart disease, valvular mechanical prostheses, aortic aneurysm or dissection, presence of ventricular thrombus, pregnancy, active neoplasia, inflammatory disease, recent surgery, stroke, deep venous thrombosis or PE.
Patient data, including demographics, medical history and treatment, including anticoagulation, are shown in table 1. AF was classified as paroxysmal and non-paroxysmal in accordance with the recommendations of the European Society of Cardiology.4
Patient characteristics
D-dimer testing
Blood samples were collected in sodium citrate tubes within 24 hours before TOE and processed at each laboratory using an identical technique (Liatest, Diagnostica Stago; Asnières, France). The assay is based on a rapid ELISA, whereby latex microspheres are coated with two anti-D-dimer monoclonal antibodies. The presence of D-dimer in the samples induces an agglutination of the microparticles, leading to increased turbidity in the reaction mixture. D-dimer levels were measured using the STAÒ (Diagnostica Stago; Asnières, France) analyser range, and expressed in ng/mL.
The standard ELISA cut-off value was 500 ng/mL, according to the manufacturers’ instructions. Age-adjusted D-dimer values are currently used as part of an algorithm to exclude PE.18
To test our hypothesis of an age-adjusted D-dimer to exclude LA thrombus in patients with AF, two D-dimer cut-offs were defined. The fixed standard D-dimer value of 500 ng/mL, DD500; and age-adjusted D-dimer value defined as 10 times the patient’s age, DDAge.
Transoesophageal echography
Indication of TOE followed the ESC guidelines to exclude LA thrombus before cardioversion.4 Therefore, all TOE included in the present study were performed in the following scenarios: anticoagulation duration shorter than 3 weeks at the time of cardioversion, a time in therapeutic range of <70% in patients receiving vitamin K antagonists and no anticoagulation with undetermined onset of arrhythmia. TOE was performed either under local anaesthesia or mild sedation (midazolam or propofol), with continuous monitoring of blood pressure and oximetry.
A 5–7 MHz multiplane probe was used, and images were independently assessed by two experienced echocardiographers. TOE operators and assessors were blinded to the D-dimer values of the patients. Images were obtained in multiple standard tomographic planes. LA thrombus was defined as a localised, uniform, ultrasound-dense, multiplane intracavitary structure distinct from the LA wall or its appendage pectinate muscle.
Statistical analysis
In the absence of previous studies evaluating adjusted D-dimers to exclude LA thrombus in patient with AF, our sample size estimation was based on statistical parameters. Most publications report a LA thrombus prevalence between 8.5% and 12% in patients with AF.8–10 Thus, in order to target a sensitivity (Se) of 100%, an Sp of at least 50% and a negative predictive value (NPV) of 100%, with power set at 80% and a type 1 error at 5%, the study should include at least 131 patients.
To assess the various statistical parameters in relation to D-dimer cut-offs and LA thrombus before cardioversion, patients were categorised in two groups: (1) ‘group 1’, in which LA thrombus was not visualised by TOE and (2) ‘group 2’, which comprised patients manifesting LA thrombus on TOE. Statistical analyses were performed using SPSS V.25.0 (SPSS, Chicago, Illinois, USA). Continuous variables are expressed as the mean±SD and categorical variables as percentages.
Both groups were compared following D-dimer cut-offs based on the Se, Sp, positive predictive value (PPV) and NPV. Continuous (mean) variables were tested with analysis of variance, while a χ² test was used for discrete variables. When multiple testings were performed, results were corrected with a Bonferroni test.
Univariate logistic regression analysis was used to assess the association between clinical and laboratory variables and the presence of LA thrombus. A multivariate stepwise logistic regression analysis was applied to identify variables independently associated with the presence of LA thrombus. A p value <0.05 was considered statistically significant. Variables with a p value <0.2, according to univariate analysis, were included in the multivariate model.
A receiver operating characteristic curve (ROC) determined the diagnostic ability of D-dimer cut-offs for LA thrombus prediction. The area under the ROC curve was calculated with 95% CI. A Pearson’s test ruled out any potential overfitting in the dataset for the ROC curve and AUC calculation.
Patient and public involvement
This research was done without patient involvement. Patients were not invited to comment on the study design and were not consulted to develop patient relevant outcomes or interpret the results. Patients were not invited to contribute to the writing or editing of this document for readability or accuracy.
Results
One hundred and forty-two patients were included in this study, the mean age was 69.7±11.4 years, with females representing 35.9% of patients (table 1). The majority of the study population received anticoagulation therapy (58.5%) and were treated with at least beta-blockers (54.9%).
LA thrombus was excluded in 129 (90.8%) patients (group 1) and confirmed in 13 (9.2%) patients (group 2) with TOE (figure 1).
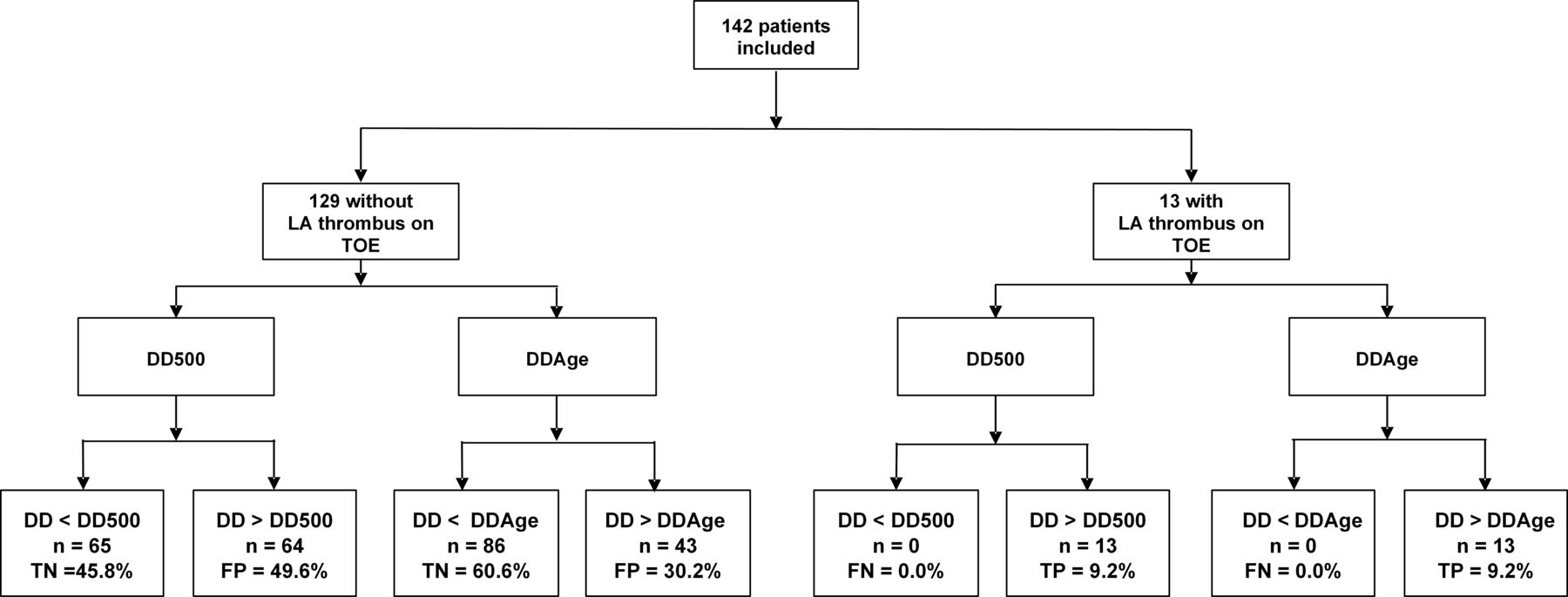
Study flow chart. DD500, D-dimer <500 ng/mL; DDAge, D-dimer <10×patient’s age; FN, false negative; FP, false positive; LA, left atrium; n, number; TN, true negative; TOE, transoesophageal echocardiography; TP, true positive.
D-dimer cut-offs to exclude left atrial thrombus
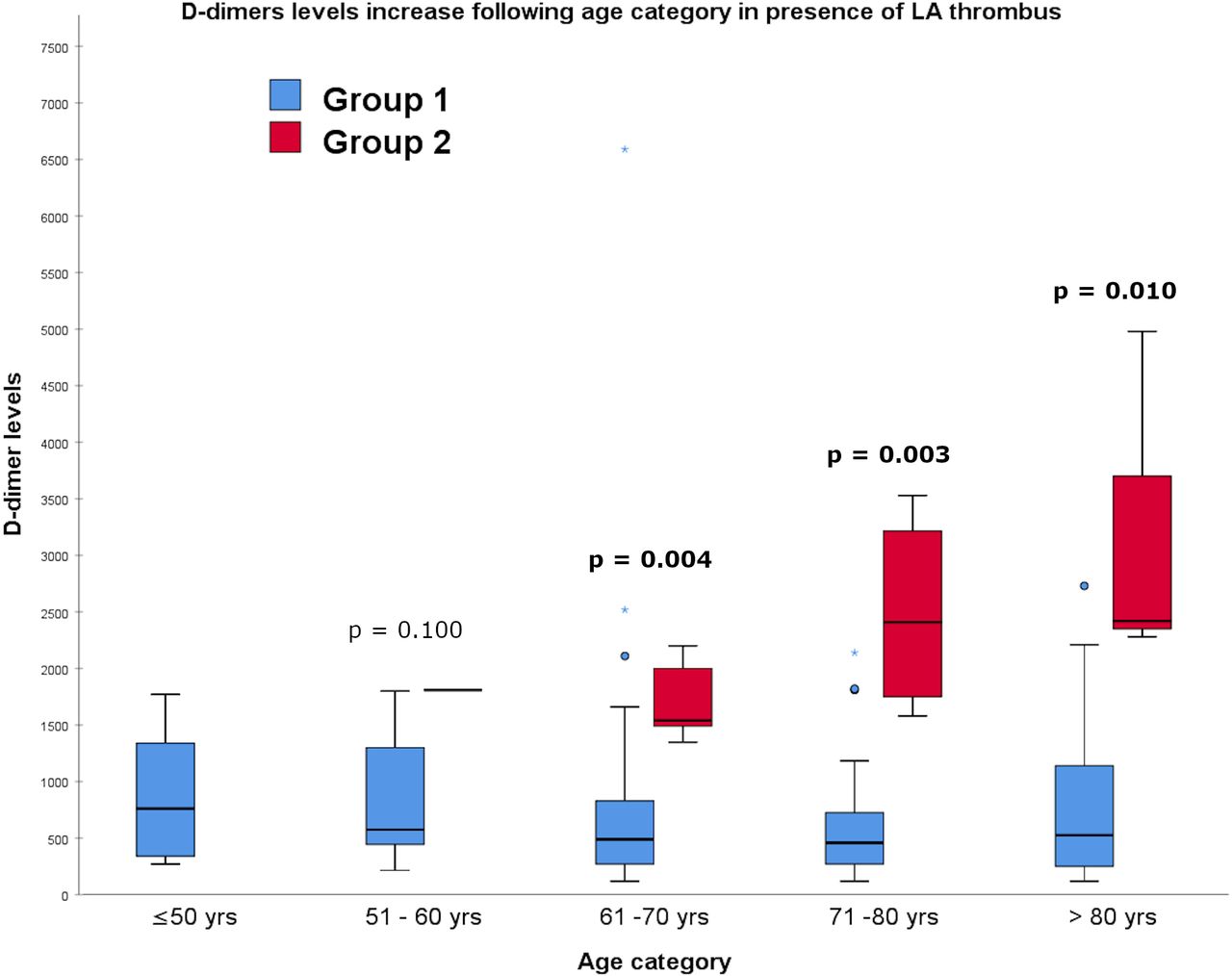
As shown in figure 2, at least one thrombus was assessed in each age category above 50 years. Moreover, for patients with LA thrombus, D-dimer values increase progressively with age. Ultimately, this leads to a significant difference between the two groups for patients above 60 years of age (p<0.05).

Evolution of D-dimer levels according to age category in the two groups with or without left atrial (LA) thrombus. Above 60 years, difference between the two groups becomes significant (p<0.05). Group 1, patients without LA thrombus on transoesophageal echocardiography (TOE); group 2, patients with LA thrombus on TOE; yrs, years.
LA thrombus was not visualised in patients with D-dimer values below DD500 or DDAge, thus true negative tests represent 45.8% (65/142) and 60.6% (86/142) of the total cohort, respectively (figure 1). This is emphasised by the NPV and Se of 100% of both cut-offs as shown in table 2 where the binary classifier’s evaluation is presented. The Sp of DDAge is significantly higher than that of DD500 (relative improvement of 24.3%, p<0.05). There was a significant increase in the PPV for DDAge compared with DD500 (relative improvement of 27.5, p<0.05).
Statistical parameters of D-dimer cut-offs
Univariate and multivariate analysis of baseline characteristics and left atrial thrombus groups
D-dimer values varied significantly between groups (p<0.05). Differences between the analysed cut-off values of DD500 and DDAge were also observed between the groups for the CHA2DS2-VASc score, history of stroke and TE, and left ventricular ejection fraction (LVEF) (p<0.05, table 3). There was no significant difference between the two groups with regard to LA volume, anticoagulation and antiarrhythmic therapy.
Characteristics of patients without (group 1) and with (group 2) thrombus and results of univariate and multivariate analyses
Based on the results of the univariate analysis, the following variables were introduced into the multivariate model: D-dimer values, including D-dimer cut-off values, CHA2DS2-VASc score, history of stroke and TE and LVEF. Independent predictors of the presence of LA thrombus are listed in table 3 (column multivariate p value). D-dimer values and the analysed cut-offs, CHA2DS2-VASc score, history of stroke and TE, LVEF and non-paroxysmal AF were identified as independent predictors for LA thrombus.
Diagnostic accuracy of D-dimer values to predict left atrial thrombus
The ROC analysis (figure 3) revealed the accuracy of high D-dimer values to predict the presence of LA thrombus (AUC 0.96; 95% CI 0.95). A value of 1344 ng/mL corresponds to an Se of 100% and an Sp of 86% for the prediction of LA thrombus.

{kind=link}
{kind=link}
{kind=link}
Receiver operating characteristic curve (ROC) curve for predicting left atrial (LA) thrombus as a function of plasma D-dimer levels. With an area under the curve of 0.96 (95% CI 0.91 to 0.98), the ROC analysis reveals the accuracy of high D-dimer values to predict the presence of LA thrombus. The value with the best sensibility/specificity (100%/86%) to predict LA thrombus presence was 1344 ng/mL.
Discussion
This study aimed at evaluating the diagnostic ability of age-adjusted D-dimer cut-off values to exclude the presence of LA thrombus in patients with AF. Our results showed that a D-dimer cut-off value defined as 10 times the patient’s age is highly efficient in excluding LA thrombus. In the patient cohort studied, 60% were found to have D-dimer levels below the defined age-adjusted cut-off value and could have safely avoided TOE prior to cardioversion. In contrast, increased D-dimer levels were associated with the presence of LA thrombus, in addition to the CHA2DS2-VASc score, history of stroke or TE, LVEF and non-paroxysmal AF.
Adjustment of D-dimer values
Patients with AF have an increased risk of thromboembolism and higher D-dimer levels compared with patients with sinus rhythm.19 The pathophysiology of thrombosis can be primarily explained by alterations in Virchow’s triad, namely, blood flow, vascular endothelial injury and hypercoagulability.19 In patients with AF, blood flow is interrupted by LA appendage stasis, with 90% of AF-related intracardiac thrombi localised in this region.20 Contrarily, LA fibrosis due to prolonged fibrillatory activity may lead to LA dilatation and dysfunction, with the latter associated with increased thromboembolic risk.21 22 Finally, AF is involved in a hypercoagulability state.19 23 24 Collectively, all three factors are reflected in the studied population (table 1).
To assess the presence of LA thrombus, TOE should be performed before cardioversion.4 Reports on TOE examinations positive for the presence of LA thrombus range from 8.5% to 12% prior to cardioversion for AF.8–10 These findings are comparable with the results in the present study, with 9.1% of patients with LA thrombus (group 2). We aimed to reduce the number of TOE examinations showing absence of LA thrombus by presenting the D-dimers as a useful predictive factor. In accordance with current literature, our results show elevated D-dimer levels in patients in AF, suggesting it as a strong discriminant between patient with and without LA thrombus (table 3).16 17 Based on similar observations, different studies suggested fixed D-dimer cut-offs alone or combined with other parameters to exclude the presence of LA thrombus, with values varying between 270 and >1000 ng/mL.14 17 25 However, selecting one definite value from these studies is challenging because of the lack of Sp of D-Dimers and their weak Sp and/or PPVs. Accordingly, on our ROC curve, the value with the best Se/Sp (100%/86%) to predict LA thrombus presence was 1344 ng/mL. This value is close to the one found by Habara et al in a large cohort where best cut-off was established at 1150 ng/mL with Se/Sp (76%/73%) and NPV of 100%.17 Nevertheless, because of its relatively high value, it would be of limited clinical use as a rule-out cut-off. Therefore, our study focused primarily on the NPV of D-dimer and the diagnostic ability to exclude LA thrombus.
In cases of suspected PE, D-dimer values <500 ng/mL exclude acute thromboembolism.18 Similarly, in our study population, no LA thrombus was visualised in patients with a D-dimer level <500 ng/mL (n=65, 45.8% of the study population, figure 1). Hence, TOE prior to cardioversion could have been avoided in almost half of the study population. However, DD500 was found to have a low Sp of 50.4% (table 2), which is mainly due to the age-dependent D-dimer values, particularly above 60 years of age.15
Clinical evaluation of age correction of D-dimer levels with a cut-off defined as 10 times the patient’s age has been performed in a randomised trial in patients with PE.26 The NPV remained remarkably high (99.7%), while the Sp increased to 46% (vs 34% for a fixed D-dimer cut-off at 500 ng/mL). In the present study, LA thrombus was not visualised in patients with a D-dimer value below this threshold, namely DDAge (figure 1). Maintaining the NPV at 100%, DDAge was shown to have a significantly higher Sp compared with DD500 (66.6% vs 50.4%; p<0.05; table 2). Therefore, TOE before cardioversion could have been safely avoided in 60.6% of the study cohort with DDAge and 45.8% with DD500 (figure 1). However, it remains necessary to exclude thrombus by imaging in the patients whose D-dimers are above the chosen threshold (D-dimers >DD500 or >DDAge). These findings confirm the safety and efficacy of DDAge in accurately excluding LA thrombus in patients with AF before cardioversion.
Clinical factors associated with left atrial thrombus
D-dimers are strongly associated with the presence of LA thrombus, showing significantly different values between groups (figure 2 and table 3). ROC curve analysis confirmed high D-dimer values to be strongly predictive of the presence of LA thrombus (AUC 0.96, figure 3). These findings are also in accordance with previous reports.16 17
In the present study, 109 patients (76.7%) had an elevated CHA2DS2-VASc score (≥2), of which 12 were diagnosed with LA thrombus by TOE (table 3). The difference in CHA2DS2-VASc score between patients with and without LA thrombus was significant (p<0.05). These results agree with previous findings showing a relationship between the a priori estimation of thromboembolic risk through CHA2DS2-VASc score and the actual presence of LA thrombus.27
Additional parameters associated with the presence of LA thrombus were a history of stroke or TE emphasising the weight of two of the stroke parameters in the CHA2DS2-VASc score.4 Furthermore, low LVEF was significantly more frequent in patients with LA thrombus. This is also consistent with the presence of heart failure in the calculation of the CHA2DS2-VASc score.28 Finally, as expected, in our cohort, non-paroxsymal patients with AF had higher risk of LA thrombus.29
Of the 83 patients (58.4%) receiving anticoagulation therapy, 5 had a LA thrombus (38.5% of group 2, table 3); however, the difference with patients without LA thrombus was found to be not significant. Regardless of the type and presence or absence of anticoagulation therapy, DD500 and DDAge accurately excluded LA thrombus in all anticoagulated patients reflecting an NPV of 100% in this category of patients. Regarding the type of AF, both thresholds prove to be robust. Whether in paroxysmal or non-paroxysmal AF, all patients with D-dimers below DD500 or DDAge are LA thrombus free (NPV=100%).
Clinical implications
The advantage of avoiding precardioversion TOE regarding clinical implications is non-negligible. First, risks inherent to performing a TOE, such as gastrointestinal tract injuries or transmission of nosocomial infections, can be avoided. This is of paramount importance in times of pandemics, such as COVID-19, where the use of TOE should be considered carefully to avoid contamination of personnel and equipment.30 Second, avoiding precardioversion TOE implies an important cost reduction, as a single D-dimer test is considerably more cost-efficient than a TOE examination. Finally, this will liberate more time to performing TOE for other indications.
Limitations
The present study had several limitations. First, a rapid ELISA test was used to measure D-dimer levels. However, with an Se of 95% and an NPV of 99%, the rapid ELISA test represents one of the most superior performing diagnostic tools available for D-dimer testing. Notwithstanding, data and conclusions could only be drawn for this specific assay and the cut-off values cannot be extrapolated to techniques other than ELISA. Second, to allow the study to be carried out, many clinical limitations have been included. Nevertheless, these clinical situations influence D-dimers upwards, which does not impact the NPVs of the selected thresholds and thus their safety. Third, a limited number of patients were included. A larger number of enrolled patients would have allowed a better definition of the best cut-off value of D-dimers to assess the risk of LA thrombus. However, the lack of Sp will always impede the interpretation of their value. As this study demonstrates, assessing LA thrombus risk with fixed value of D-dimers is clinically and statistically less relevant than adjusted cut-offs. In our cohort, age adjustment is as safe as the fixed value of 500 ng/mL and furthermore allows to avoid safely up to 60% of the total number of unnecessary TOE.
Conclusion
This study demonstrates the efficacy of D-dimer cut-offs to exclude the presence of a LA thrombus in patients with AF. Age adjustment greatly increases the proportion of patients in whom LA thrombus can be safely excluded, and consequently avoid TOE before cardioversion.
Key messages
What is already known on this subject?
The presence of left atrial thrombus in patients with atrial fibrillation is more important than in general population leading to an increase in the risk of stroke.
To assess that risk before electrical cardioversion, patients routinely undergo a transoesophageal echocardiography, which exclude thrombus in >80% of the patients.
D-dimers are considered strong biological markers of coagulation activation and fibrinolysis.
What might this study add?
No previous studies have reported the role of adjusted D-dimer cut-off levels in excluding left atrial thrombus.
Our study evaluated its role in patients with atrial fibrillation before electrical cardioversion.
D-dimer cut-offs fixed to 500 ng/mL as well as cut-offs adjusted to 10 times the age of the patient were compared.
How might this impact on clinical practice?
The present study demonstrated the efficacy of D-dimers cut-offs to exclude left atrial thrombus in patients with atrial fibrillation.
Age adjustment considerably increases the proportion of patients in whom left atrial thrombus can be safely excluded, consequently avoiding precardioversion transoesophageal echocardiography.
References
Footnotes
Contributors All authors have made a significant contribution to the findings in the paper. AA being responsible for the overall content as guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Ethics approval This study was approved by the CHU-Brugmann and AZ Sint Jan Ethics Committees. Written informed consent was obtained from all patients before participation.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request. NA.