Article Text

Abstract
Objective A high risk of morbidity and mortality is well documented in adults with a Fontan circulation. The difference in outcomes between those with and without significant morbidity at the time of transition to adult care has not been well characterised.
Methods We analysed clinical outcomes in patients enrolled in the Australian and New Zealand Fontan Registry ≥16 years of age. Low risk (LR) Fontan patients were defined as those without history of sustained arrhythmia, thromboembolic event, transplantation, Fontan conversion, protein-losing enteropathy, plastic bronchitis, New York Heart Association class III/IV and/or moderate/severe atrioventricular valve regurgitation or ventricular dysfunction. Increased risk (IR) patients had one or more risk factor.
Results Inclusion criteria were met in 822 patients; mean age 26±8 years, median follow-up from age 16 was 9 years, 203 had atriopulmonary connection (APC) and 619 had total cavopulmonary connection (TCPC). Survival at 30 years was higher in the LR versus IR; 94% versus 82% (p=0.005), 89% versus 77% (p=0.07) for APC and 96% versus 89% (p=0.05) for TCPC. LR patients experienced less Fontan failure (HR 0.34, 95% CI 0.23 to 0.49, p<0.001) and ventricular dysfunction (HR 0.46, 95% CI 0.29 to 0.71, p=0.001) compared with IR patients. For LR TCPC patients, modelled survival projections at 60 years were 49%–67%.
Conclusions Clinical outcomes for adolescents LR at transition to adult care are markedly superior to those who have established risk factors for Fontan failure, which is an important consideration when formulating individualised long-term risk estimates and counselling patients.
- Fontan physiology
- complex congenital heart disease
- health care delivery
Statistics from Altmetric.com
Introduction
Fontan surgical palliation has enabled the majority of children born with functionally single ventricle hearts to survive well into to adolescence and adulthood,1 although with reduced survival and high rates of morbidity compared with the general population.2 Although we have previously reported the mortality rates and clinical outcomes of people living with a Fontan circulation who survived to the age of transition to adult care followed by the Australian and New Zealand Fontan Registry (ANZFR),3 it is unclear how these estimates differ between adolescents who are relatively thriving compared with those who have risk factors for Fontan failure. Furthermore, the projected survival into middle age for the subgroup of young people, without high-risk features who had Fontan surgery in the modern era, is unknown, which makes counselling challenging.
We therefore sought to better describe the survival and risks for Fontan failure in young people living with a Fontan circulation who survive to the age of transition to adult care when categorised as low risk (LR) or increased risk (IR) according to the presence or absence of factors that increase risk for failure.
Methods
The ANZFR has been described in detail previously.4 In brief, since 2008, when the registry was commenced, all patients who had a Fontan procedure in Australia or New Zealand, or who had had their procedure overseas but are followed in our region, were included. All paediatric and adult congenital heart disease (ACHD) centres within Australia and New Zealand participate in the ANZFR. The study included patients who were alive without cardiac transplantation or Fontan takedown at or over the age of 16 years, had their Fontan procedure before 2019, did not have the date or type of Fontan missing, were eligible for inclusion in the ANZFR and had provided consent. This study uses data collected up to the end of 2018 and was extracted from the ANZFR REDCap database on 1 August 2019.
Definitions
Low risk
No history of a complicating event before the age of 16 years.
Increased risk
Before the age of 16 years, experienced one or more of the following: a sustained arrhythmia requiring treatment, thromboembolic event, Fontan conversion, plastic bronchitis, protein losing enteropathy, New York Heart Association (NYHA) class III or IV functional class moderate or worse ventricular dysfunction or atrioventricular valve regurgitation (AVVR).
Fontan failure
Death, heart transplantation, Fontan takedown or conversion, protein-losing enteropathy, plastic bronchitis or NYHA functional class III or IV at follow-up.
Total cavopulmonary connection
Incorporates both lateral tunnel and extracardiac conduit Fontan surgical techniques.
Arrhythmia
Any tachyarrhythmia or bradyarrhythmia; paroxysmal, persistent or permanent recorded in the clinical letter from the treating cardiologist.
Thromboembolic event
Cerebrovascular event, deep vein thrombosis, pulmonary embolism or any other thromboembolic event recorded in the clinical letter from the treating cardiologist.
Statistical analysis
Statistical analyses were performed using Stata (V.15) and R software (V.3.4.3, R Foundation, Vienna, Austria). Descriptive statistics for patient characteristics are described for all patients, risk category and Fontan type. For comparisons of continuous variables, the t-test was used if the distribution was approximately symmetrical; otherwise, the Wilcoxon rank-sum test was used. Fisher’s exact test was used for comparisons of categorical variables. The Kaplan-Meier method was used to analyse the time-to-event endpoints not subjected to competing risks, with 95% CIs being given when providing point estimates. The censoring distribution for deaths was used to estimate the median follow-up time with the Kaplan-Meier method. Time-to-events subjected to competing risks (namely, heart transplantation or death) were summarised using cumulative incidence curves. Cox regression models (cause-specific if competing risks present) and likelihood ratio tests were used to assess the effect of patient characteristics on the time-to-event endpoints. The proportional hazards assumption was assessed based on the method of Harrell and Lee and via diagnostic plots. Patients who underwent a Fontan procedure over the age of 16 years (n=44; 5.4%) were entered into the risk set at the age when the Fontan procedure was performed. All p values less than 0.05 were considered statistically significant, and where possible, estimates were provided with the corresponding 95% CI. Estimates of projected survival for LR patients were obtained by fitting a Weibull regression model using the Stata function ‘streg’ and ‘predict’. Parametric approaches are suitable when survival rates are relatively consistent5; however, there is uncertainty about how survival rates will change in later years. Several scenarios were therefore modelled, as per earlier work on Fontan projections.6 In the ‘optimistic’ scenario, Fontan mortality risks continue on current trends until reaching the all-cause wider population mortality risks that increase sharply in later years. In the ‘conservative’ scenario, the ratio of mortality risk between Fontan survivors and the wider population, as measured by the Australian life tables,7 was maintained from the last point of follow-up. A further ‘pessimistic’ scenario was modelled to explicitly consider the possibility that the total cavopulmonary connection (TCPC) cohort may experience significant deterioration in survival, as observed in the atriopulmonary connection (APC) cohort; in this worst case scenario, the mortality risks for the LR TCPC cohort was increased to match the APC mortality risk from age 55 years.
Patient and public involvement
Patients and the public were not involved in the research process for this manuscript.
Results
A total of 822 patients met inclusion criteria for the study. Subject characteristics are shown in table 1.
Patient characteristics
Risk classification
Of the entire cohort, 610 (74.2%) patients were classified as LR and 212 (25.8%) patients as IR, with an identical proportion seen among APC and TCPC patients. The most common reasons for exclusion from the LR group were prior arrhythmia (60%), thromboembolic event (23%) and moderate or greater AVVR (16%) (online supplemental table 1). Among patients at IR, those with APC compared with TCPC were more likely to have had prior arrhythmia (96% vs 48%, p<0.001) and less likely to have had prior thromboembolic event (8% vs 28%, p=0.002) or moderate/severe AVVR (0% vs 21%, p<0.001). The majority of IR patients met only a single exclusion criterion (83%). Patients deemed at IR had higher rates of male sex, hypoplastic left heart syndrome, systemic ventricle of non-left morphology, isomerism and previous cardiac procedures.
Supplemental material
Survival and/or heart transplantation
There were 71 deaths over a median follow-up time of 9.2 years. Overall survival was higher in the LR group compared with the IR group; 85% versus 76% at 40 years (HR 0.49 (95% CI 0.29 to 0.81), p=0.004) (figure 1A). Irrespective of Fontan type, LR patients had greater survival compared with IR patients (figure 1B). On univariable analysis, a history of prior cardiac procedures was predictive of survival. Male sex did not reach significance (HR 1.51 (95% CI 0.94 to 2.45), p=0.09). There was no difference observed between patients with a lateral tunnel (LT) or extra-cardiac conduit (ECC), within the TCPC cohort (online supplemental figure 1).
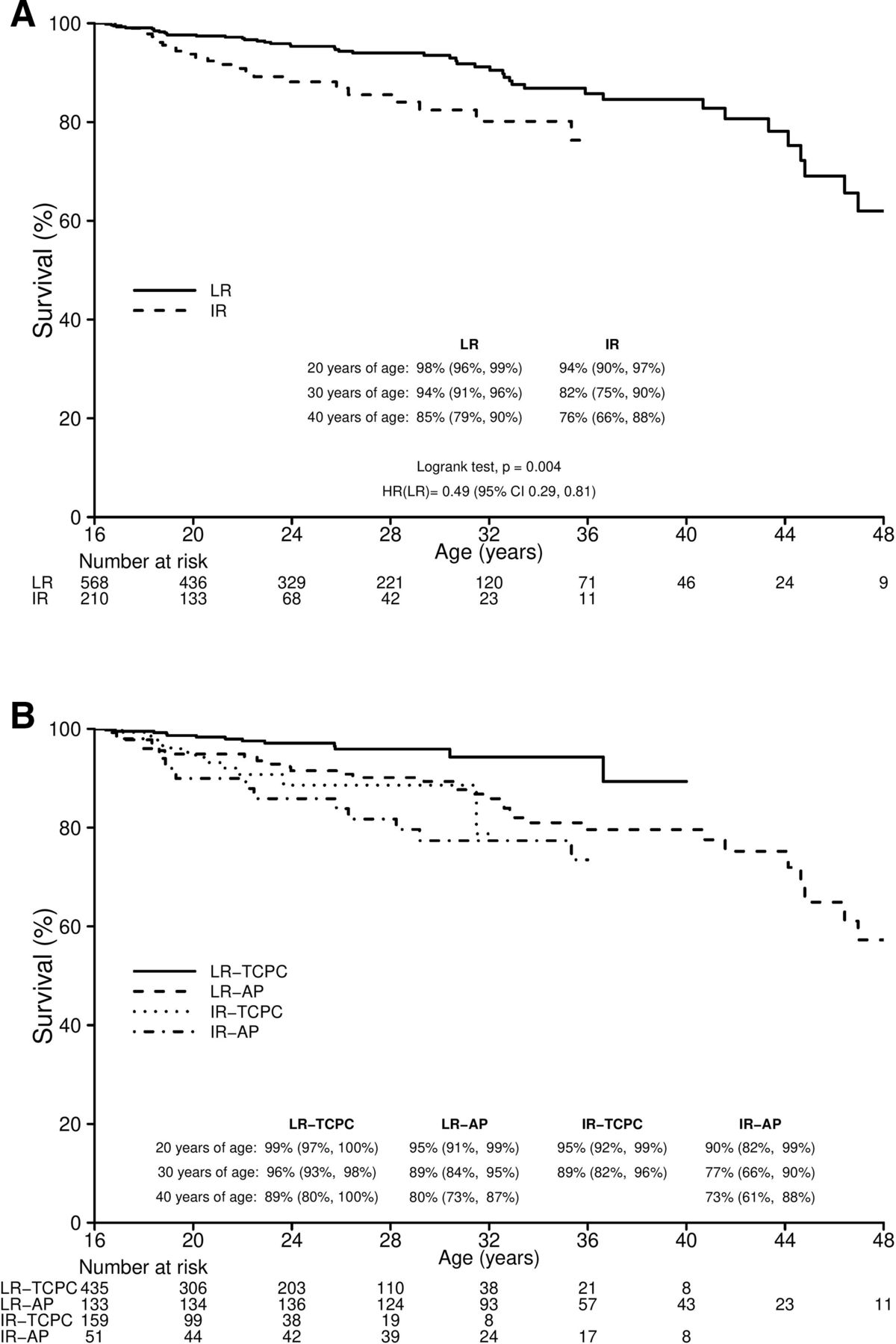
Kaplan-Meier curves plotting survival for low-risk versus increased risk patients as a whole (A) and by Fontan type (B). AP, atriopulmonary; IR, increased risk; LR, low risk; TCPC, total cavopulmonary connection.
Freedom from death or heart transplantation was similarly higher in the LR group; 83% versus 67% at 40 years (HR 0.44 (95% CI 0.28 to 0.69), p=0.001). Within the IR group, on multivariable analysis, the presence of a concomitant procedure (HR 2.51 (95% CI 1.22 to 5.15), p=0.012) at time of Fontan was predictive of death or heart transplantation. In the LR group, multivariable analysis was not achievable due to non-significance.
Fontan failure
Fontan failure was identified in 126 patients after 16 years of age. The LR group had significantly less Fontan failure than the IR group (HR 0.34 (95% CI 0.23 to 0.49), p<0.001) (figure 2A). For both APC and TCPC, the LR group was significantly less likely to suffer Fontan failure (APC: HR 0.35 (95% CI 0.22 to 0.55), TCPC: HR 0.35 (95% CI 0.19 to 0.65), interaction p=0.93) (figure 2B). The presence of an APC predicted Fontan failure on univariable analysis, while multivariable analysis was not achievable due to non-significance.

{kind=link}
{kind=link}
Kaplan-Meier curves plotting freedom from Fontan failure for low-risk versus increased risk patients as a whole (A) and by Fontan type (B). The cumulative incidence of ventricular dysfunction by risk category is shown in panel C. AP, atriopulmonary; IR, increased risk; LR, low risk; TCPC, total cavopulmonary connection.
Ventricular systolic dysfunction
Moderate or greater ventricular systolic dysfunction was identified in 91 patients. The LR group experienced significantly less than the IR group (HR 0.46 (95% CI 0.29 to 0.71), p<0.001) (figure 2C). There was no association between type of Fontan and ventricular dysfunction. The cumulative incidence of ventricular dysfunction increased with age and time from Fontan procedure was significant, even in the LR group. On multivariable analysis, male sex, hypoplastic left heart syndrome (HLHS) and the presence of a bilateral bidirectional cavopulmonary shunt (BCPS) were predictive of subsequent development of ventricular dysfunction in the LR group. Male sex and right isomerism were predictive in the IR group.
Survival modelling by Fontan type
Modelled survival estimates beyond the follow-up period were calculated using a Weibull distribution for LR patients. Three different scenarios (see Methods) of projected mortality risk are shown in table 2.
Modelled survival estimates for low-risk patients
Discussion
The number of patients who have undergone a Fontan procedure surviving to young adulthood and transitioning into adult congenital care is increasing.8 Cohorts of Fontan patients are highly heterogeneous and their survival expectations are likely to differ substantially depending on their clinical phenotype. We present the first study describing the survival expectations of two cohorts of patients—LR and IR—using the comprehensive data collected over the last 10 years in the ANZFR. The significant proportion of LR patients surviving well into middle age should inform future resource allocations and aid patient counselling.
Overall survival and freedom from Fontan failure
Medium-term survival of Fontan patients has increased over time,4 9 and it is now expected the majority will survive well into adulthood.6 10 We found almost three-quarters of adolescents were free from important risk factors at the age of transition and not surprisingly demonstrated that survival and other clinical outcomes were superior in this group. Using childhood outcomes as a tool to predict trajectory into adulthood is both simple and effective and a concept used daily by clinicians: that past events predict future ones. These results highlight the importance of optimising early outcomes and encourage further research into early prevention and intervention strategies (both pre-Fontan and post-Fontan repair). Although this may seem obvious, formal data are scant when counselling patients, to help us appropriately advise them about future risks. Our data suggest that an LR TCPC Fontan adolescent has a 76% chance of being free from Fontan failure at 40 years of age, an 89% chance of being alive and, based on our modelled scenarios, a 49%–67% chance of surviving into their seventh decade. These estimates are far more optimistic than figures derived from an entire Fontan cohort or even in those who survive to the age of transition.3
Ventricular dysfunction
Somewhat concerningly, the onset of systemic ventricular systolic dysfunction increased with age in both cohorts. Although higher rates were observed in the IR cohort, almost 10% of LR patients went on to develop significant ventricular dysfunction. Although not fully understood, there are likely a myriad of reasons the ventricle develops systolic dysfunction in the setting of Fontan physiology including innate morphological and haemodynamic substrates, volume loading during first and second stage palliation, chronic cyanosis, valvular regurgitation, mass to volume mismatch and chronic volume deprivation. It has been shown, compared with healthy controls, Fontan patients exhibit impaired contractility and ventricular efficiency, even in those considered ‘clinically stable’ and in those with an ejection fraction >50%.11
In this study, male sex is a consistent risk factor on multivariable analysis between groups. Male sex in univentricular patients has been associated with a higher risk of cardiovascular complications including overall mortality and perioperative mortality following Fontan conversion.12 13 Although male sex is a well-recognised risk factor for late mortality post-Fontan,4 12 this is the first to report, to our knowledge, an increased risk of ventricular systolic dysfunction in male adult Fontan patients. How or why sex plays a role is not immediately identifiable. In generalised ACHD populations, male sex has been linked with increased arrhythmic complications, but this has not been demonstrated in the Fontan population, nor has it been linked to ventricular dysfunction.14 Further research into the underlying mechanisms of sex disparity in Fontan is required.
Other predictors identified in this study, such as HLHS, bilateral BCPS in the LR and right atrial isomerism in the IR, likely reflect either the presence of a systemic right ventricle or more complex congenital heart lesions. We have previously demonstrated worse outcomes post-Fontan in HLHS patients15 and long-term evaluation of systemic right ventricles demonstrates almost universal ventricular dysfunction over time.16 17 Recent studies have shown patients with bilateral BCPS are more likely to have systemic right ventricles and heterotaxy with worse outcomes following Fontan completion.18 19
The implications for health systems
Even if you consider the pessimistic scenario to be true, we should expect to be looking after a significant proportion of our Fontan population well into middle age—a prospect that clinicians and health systems once considered impossible. The relative resource deficit affecting this population is already well recognised20 and appropriate specialised care has been shown to improve patient outcomes including survival, especially in severe congenital heart disease such as those with a Fontan.21 22
Improved survival of this complex patient group will come at the cost of increased morbidity and a large burden on the health workforce. Though we can expect reduced rates of complications in TCPC versus APC and LR versus IR, it remains that only 43% of all adult Fontan patients are free from a serious adverse event at 40 years of age3; long-term complications include arrhythmia, thromboembolic disease and heart failure as well as non-cardiac complications such as Fontan-associated liver disease, hepatocellular carcinoma, nephropathy, lymphatic dysfunction and impaired bone health. It is likely that the numbers of reinterventions, percutaneous and surgical, will also increase with the growing and ageing Fontan population, as will the need for heart transplantation, for which there is already a shortage of donors.23 Appropriate funding and resource allocation will be required to ensure patient outcomes are optimised.
Patients’ mental health and future uncertainties
Uncertainty and fear about the future is a well-recognised concern for young people living with a Fontan circulation and is a major driver of anxiety.24 Mental health problems including anxiety, depression and medical non-adherence are common in patients with ACHD; adolescent Fontan patients are estimated to have a fivefold increased risk for an anxiety disorder.25 This study allows clinicians to better educate patients and caregivers with individualised estimates of prognosis which, for many LR patients, are likely to be superior to what they estimated or had previously been advised.
Study limitations
The ANZFR is the largest database of Fontan patients in the world but as with all registry data, some information is collected retrospectively and may be incomplete for certain patients and centres. The data rely on letters from treating cardiologists for ongoing data collection. Although survival and Fontan failure are the most important measures of outcomes, other causes of late morbidity, including non-cardiac complications and medication burden, were not assessed. Our cohort consists of a relatively low proportion of patients with HLHS, and results may therefore be more favourable and less generalisable to cohorts with a higher proportion of this high-risk congenital lesion. Management decisions for patients were not uniform but at individual physician’s discretion. In regards to the projected survival, although we have provided a range of scenarios, there are inherent limitations of accuracy due to future unknowns such as medical and surgical innovations or late complications of the TCPC.
Conclusions
Long-term survival following Fontan repair has improved due to enhanced surgical and medical care, leading to an ever-growing and ageing adult Fontan population. Despite this, significant morbidity and reduced life-expectancy remains. This report demonstrates improved survival and morbidity in patients free from adverse clinical outcomes before transition to adult care compared with those who have suffered previous adverse events. The majority of LR patients are surviving into middle age without significant comorbidity. This along with our modelled estimates should warn of a growing need for enhanced resources in the future. When discussing long-term outlook, this more detailed and tailored prognostic advice will benefit patients, caregivers and clinicians.
Key messages
What is already known on this subject?
Medical and surgical innovations have led to improved outcomes for Fontan patients.
The growing Fontan population is living well into adulthood but still has reduced survival and high rates of morbidity compared with the general population.
What might this study add?
Further characterisation of expected outcomes for Fontan populations based on risk categorisation at transition.
Adolescent Fontan patients deemed low risk have a far better prognosis than previously reported for a Fontan population.
Modelled projections of survival are encouraging well into middle age.
How might this impact on clinical practice?
Provides novel information that will assist clinicians, patients and caregivers when discussing individualised long-term risk estimates.
Forewarns of a growing and ageing population of Fontan patients that will require appropriate funding and resource allocation.
Acknowledgments
The authors acknowledge support provided by the National Health and Medical Research Council (NHMRC) of Australia to the Australian and New Zealand Fontan Registry and the support provided to the Murdoch Children’s Research Institute by the Victorian Government’s Operational Infrastructure Support Program. We also acknowledge assistance provided through the National Death Index linkage and Australian Institute of Health and Welfare in compiling data.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
DWB and MRD are joint first authors.
Contributors All authors meet criteria for authorship based on ICMJE guidelines and contributed in the following way; conception (RC) and design of the work (all authors), data collection (DWB, MRD, DZ, CS and DPM), data analysis and interpretation (DZ, CS, DWB, MRD and RC), drafting the article (DWB, MRD and RC), critical revision of the article (all authors) and final approval of the version to be published (all authors). The lead author (RC) accepts responsibility of overall content as guarantor.
Funding This work was supported by an NHMRC Partnership Grant (1076849). YdU is a Clinician Practitioner Fellow of the NHMRC (1082186).
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request. Data are available from the Australian and New Zealand Fontan registry. Written application will be reviewed by the Fontan Registry Steering Committee. Please contact info@fontanregistry.com or visit fontanregistry.com.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.