Article Text

Abstract
Objective To provide insight into professionals’ perceptions of and experiences with shared decision-making (SDM) in the treatment of symptomatic patients with severe aortic stenosis (AS).
Methods A semistructured interview study was performed in the heart centres of academic and large teaching hospitals in the Netherlands between June and December 2020. Cardiothoracic surgeons, interventional cardiologists, nurse practitioners and physician assistants (n=21) involved in the decision-making process for treatment of severe AS were interviewed. An inductive thematic analysis was used to identify, analyse and report patterns in the data.
Results Four primary themes were generated: (1) the concept of SDM, (2) knowledge, (3) communication and interaction, and (4) implementation of SDM. Not all respondents considered patient participation as an element of SDM. They experienced a discrepancy between patients’ wishes and treatment options. Respondents explained that not knowing patient preferences for health improvement hinders SDM and complicating patient characteristics for patient participation were perceived. A shared responsibility for improving SDM was suggested for patients and all professionals involved in the decision-making process for severe AS.
Conclusions Professionals struggle to make highly complex treatment decisions part of SDM and to embed patients’ expectations of treatment and patients’ preferences. Additionally, organisational constraints complicate the SDM process. To ensure sustainable high-quality care, professionals should increase their awareness of patient participation in SDM, and collaboration in the pathway for decision-making in severe AS is required to support the documentation and availability of information according to the principles of SDM.
- heart valve prosthesis implantation
- transcatheter aortic valve replacement
- aortic valve stenosis
- quality of health care
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Statistics from Altmetric.com
- heart valve prosthesis implantation
- transcatheter aortic valve replacement
- aortic valve stenosis
- quality of health care
Introduction
Incorporating shared decision-making (SDM) in the treatment of symptomatic patients with severe aortic stenosis (AS) is challenging. Multiple treatment options, certain patient characteristics, including multimorbidity, frailty and impaired cognition, and patient expectations regarding participation emphasise the importance of thoughtful decision-making (DM).1 2 Treatment options for severe AS include conservative treatment (CT), transcatheter aortic valve replacement (TAVR) and surgical aortic valve replacement (SAVR).
SDM is a well-defined process in which professionals and patients discuss care and cure decisions, thereby using the best available evidence and patients’ personal preferences and goals. The result of this process is a thoroughly considered decision.3 SDM increases patients’ knowledge of treatment options, initiates accurate risk perception, and creates participation and comfort with decisions.4 SDM also improves patient satisfaction and reduces undesired care in certain categories of patients.5
Implementing the SDM process in daily practice is influenced by various barriers and facilitators. Barriers in non-cardiological healthcare settings are professionals’ lack of knowledge of and a negative attitude towards SDM.6 7 Despite multiple reasonable treatment options for severe AS and recommendations for SDM in AS guidelines,8–11 SDM is still not common practice.12–14 Thus far, professionals’ perceptions of and experiences with SDM in cardiological and cardiac surgical practice are not well known.12 14–16 To optimise SDM in the care process of symptomatic patients with severe AS, it is essential to enhance the proposed understanding of professionals’ views on SDM.17
Therefore, this study aims to provide insight into professionals’ perceptions of and experiences with SDM in the treatment of symptomatic patients with severe AS.
Methods
Design
We used a semistructured interview to explore indepth perceptions and experiences. Questions and topics were based on critical issues in prior interviews.18 Standards for reporting qualitative research (COnsolidated criteria for REporting Qualitative research) have been used for transparent reporting.19
Setting and participants
The study was conducted in nine heart centres of academic hospitals and large teaching hospitals in the Netherlands between June and December 2020. We purposively invited cardiothoracic surgeons, interventional cardiologists, nurse practitioners and physician assistants who were involved in the DM process for treatment of severe AS and evaluated the patient at least 2 days before the treatment (figure 1).

Flow chart of study design.
Data collection
We invited professionals by email to participate. If a professional agreed to participate, we sent the information letter and informed consent form.
The topic list of the interview drew on Fishbein and Ajzen’s Integrative Model of Behaviour Prediction.20 This model implies that behaviour is a product of attitude, perceived social norms and self-efficacy related to behaviour. Topics included the definition of SDM, opinions about SDM, approach to discussing risks and benefits of treatment of severe AS, the use of decision aids, patient and informal caregiver involvement in DM, knowledge of SDM research, and barriers and facilitators of SDM.6 7 17 A panel of three professional experts evaluated the construct validity of the topic list. Topics were included when the majority of the experts agreed. After piloting the interview guide, several minor improvements were made.
Two trained researchers (JJAMvB-P and JBLvdM) conducted the interviews. Due to the COVID-19 pandemic, participants were offered a choice for face-to-face or online interviews. The interviews were arranged at a time and place that suited the participants. The interviews were audiotaped with the participants’ permission and transcribed verbatim and anonymously.
We used the findings that emerged from the first interviews to improve the subquestions for subsequent interviews (online supplemental 1).
Supplemental material
Data analysis
To identify, analyse and report patterns in the data, we performed an inductive thematic analysis. We used an essentialist analysis method to ensure that participants’ true meanings were reported. Also, we used a rich thematic description to maximise insight into all important concepts.21 ATLAS-ti V.9.0 (computer software) was used to analyse the data.
The development of the coding structure was an iterative process. First, JJAMvB-P and JBLvdM read and coded four transcripts using the principle of open coding of data. Next, we discussed the results in the research team and determined the final codes and code groups. The remaining transcripts were coded independently (JJAMvB-P and JBLvdM), and new codes were added when data did not fit an existing code. In regular meetings, JJAMvB-P, JBLvdM, MCF and AJBMdV discussed data saturation and the refinement of codes and code groups. Respondents were included until consensus was reached that no new codes emerged from the data. Finally, we merged the identified code groups into themes based on similarities (online supplemental 2). Discrepancies were resolved by discussion and consensus within the research team. To maximise the reliability and integrity of the results, we performed a member check,22 which established the trustworthiness of the results.
Supplemental material
To relate the identified themes to a previous taxonomy of the SDM process, we mapped the themes to the adapted taxonomy of barriers and facilitators to SDM.7 In this taxonomy, barriers and facilitators can be structured in seven categories: predisposing factors (patient and decision characteristics), interactional context factors (social factors regarding the relation between patients and health professionals), preparation for the SDM encounter (perceived need for preparation by patients and expectations about involvement), preparation for the SDM process (providing information about options, decision support and terminology used), organisational factors (healthcare organisations), social factors (healthcare settings, interdisciplinary team) and policy factors (healthcare system, health government).7
Patient and public involvement
Patients or the public were not involved in the design, or conduct, or reporting or dissemination plans of our research.
Results
Data saturation was reached after 21 interviews (figure 1). We included eight cardiothoracic surgeons, seven interventional cardiologists, five nurse practitioners and one physician assistant (table 1). The 21 professionals represented 9 out of 16 heart centres in the Netherlands, of which all heart centres corresponded to approximately 4200 SAVR and TAVR in 2019.23
Characteristics of the interviewed professionals
The 9 face-to face and 12 online interviews lasted 34 min on average.
Data analysis generated four primary themes: (1) the concept of SDM, (2) knowledge, (3) communication and interaction, and (4) implementation of SDM (figure 2). Respondents were numbered to allow identification of quotations.
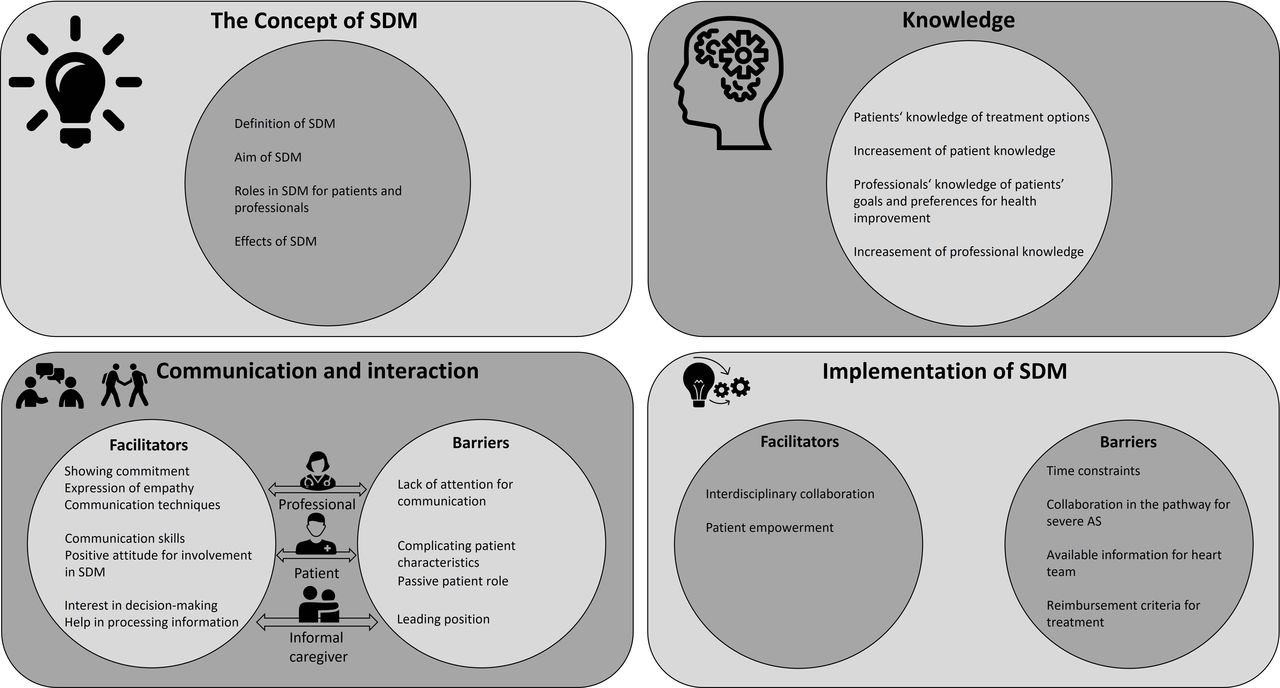
Themes generated from the data. AS, aortic stenosis; SDM, shared decision-making.
The concept of SDM
Most respondents defined SDM as an interaction between the patient and the professional, in which they discussed the pros and cons of the treatment and made decisions together. Other respondents characterised SDM as a multidisciplinary activity without mentioning patient participation.
I would define SDM as looking at a patient’s problem with multiple disciplines together, where you offer a type of custom-made solution for each patient. (Respondent 006, cardiothoracic surgeon, 6 years in practice)
Respondents regarded informed consent as consent for treatment after a decision for treatment was made. Ten respondents indicated that SDM is broader and different from informed consent. Five respondents noted that SDM and informed consent were similar. Respondents explained that SDM aims to facilitate an informed decision for best treatment and includes patient support for this decision.
SDM is informing the patient, and based on this informed patient, SDM is actually making a decision together with the patient. (Respondent 021, interventional cardiologist, 10 years in practice)
Respondents considered SDM to be a DM process with roles for both the professional and the patient, but most respondents were not aware of how SDM was described in the AS guidelines. Some emphasised that patients have to make the final treatment decision, while six of them added that professionals can direct the decision during the consultation. Nearly all cardiothoracic surgeons and a minority of the interventional cardiologists and nurse practitioners were convinced that professionals in particular have expertise about treatment options.
However, as a physician you have to try to explain why you make that choice for a patient, and finally based on this, the patient can decide whether he agrees with that choice.
(Respondent 016, cardiothoracic surgeon, 15 years in practice)
Respondents believed that SDM leads to appropriate care and cure and increases patients’ motivation and acceptance for treatment. Some mentioned the importance of SDM for every patient and highlighted that SDM guides patients towards empowerment of their own health situation.
I think that in most cases, SDM is working well because the patient also participates in decisions and is partly in the lead. This makes it easier for patients to support a decision. (Respondent 019, interventional cardiologist, 10 years in practice)
Knowledge
Patients’ knowledge regarding treatment options enhances SDM, according to the respondents.
They valued patients’ own ideas about the treatment options. However, they also expressed concerns about patients’ lack of sufficient knowledge for making treatment choices and patients’ inability to consider the consequences of decisions. Ten respondents described a discrepancy between patients’ treatment wishes and real treatment options.
The patient may have different expectations of the treatment than we can actually provide. (Respondent 013, cardiothoracic surgeon, 7 years in practice)
Respondents explained that written and digital information regarding treatment options increases patients’ knowledge, although it takes time for patients to process the information. Respondents used verbal strategies during the consultation to improve patients’ knowledge (eg, they clarified the aim and the risks of the treatment and asked for patients’ knowledge and opinion about treatment of severe AS). Most of the respondents were not familiar with decision aids to improve patients’ knowledge.
Professionals’ knowledge of patients’ goals and preferences for health improvement is also essential for SDM, according to the respondents. However, four of them highlighted the absence of this knowledge prior to consultations.
And so those goals and motives…usually only come up during the conversation…maybe it has been discussed before, but anyway, not known. (Respondent 004, cardiothoracic surgeon, 2 years in practice)
To increase their familiarity with patients’ goals and preferences, most respondents explained that they asked for patients’ preferences regarding health improvement and managed expectations about treatment outcomes during the consultation. One cardiothoracic surgeon and one nurse practitioner mentioned that they specifically discussed health improvement.
I always check with patients: …what do you hope this will bring you? Is this a realistic expectation of valve replacement? (Respondent 018, nurse practitioner, 11 years in practice)
Communication and interaction
Respondents described facilitators for patients, informal caregivers and professionals regarding their communication and interaction in SDM.
They emphasised the importance of patients having good communication skills and a positive attitude for being involved in SDM. Additionally, they reported their expectations regarding patient roles for SDM, such as patients’ awareness of having a treatment choice, insight into their own illness and willingness to participate in conversations.
Respondents also noted that the informal caregiver’s interest and awareness facilitate SDM. Informal caregivers help patients process the information and clarify patients’ symptoms and situation.
When someone is sitting next to the patient, the partner, or the daughter, you notice that things are happening, that someone says, ‘But, Mum, you actually have this and that’. (Respondent 014, nurse practitioner, 4 years in practice)
Additionally, respondents explained that patients’ trust in professionals and professionals’ commitment to patients support SDM. They described their expression of empathy and interest and noted communication techniques for SDM (eg, directing the conversation and moderating). Three cardiothoracic surgeons explicitly introduced SDM during the consultation.
And then I explain all the pros and cons and I say, ‘And now we are going to decide together’. (Respondent 004, cardiothoracic surgeon, 2 years in practice)
Most respondents mentioned complicating patient characteristics for SDM, such as a low level of education, cognitive impairment and difficulties in communication. They suggested that most older patients have difficulty explaining their health situation and processing information. Additionally, respondents perceived that younger patients prefer SDM, while older patients prefer a more passive role in DM.
Older people from a completely different generation…they are much more like…if you say so, we will do so, and that is a shame because it is not necessary. (Respondent 020, nurse practitioner, 15 years in practice)
Others added that a passive patient role complicates SDM when patients do not want to know about treatment options or leave the decision to the professional.
Because apparently, they do not want that responsibility at all. So, yes, to what extent does a patient truly want an important role…some do not want that at all. (Respondent 003, cardiothoracic surgeon, 10 years in practice)
Respondents also perceived difficulties when informal caregivers take a leading position and draw attention to themselves.
And then you really notice that the family pushes a lot more for the operation than the patient himself. (Respondent 012, cardiothoracic surgeon, 22 years in practice)
In particular, physicians explained being trained in communication skills and SDM during their medical education, while some respondents noted the lack of further attention for communication skills in daily practice. One interventional cardiologist and one nurse practitioner suggested that professionals should learn from each other to improve communication skills.
It would be good that every now and then the communication is checked and, if necessary, adjusted and discussed. (Respondent 001, interventional cardiologist, 23 years in practice)
Implementation of SDM
All respondents experienced social and organisational barriers to the implementation of SDM.
They mentioned that implementing SDM is time-consuming and that time for consultations is limited. Respondents also explained that they are often dependent on the information about treatment options provided in the referring hospital. One cardiothoracic surgeon and one nurse practitioner added that information regarding the previous communication process between the patient and the referring cardiologist is often lacking. However, this information could facilitate SDM in the heart centre.
And you are very dependent on the referring cardiologist; thus, what did he say, how did he say it, how did it get to the patient? (Respondent 008, physician assistant, 10 years in practice)
In particular, physicians explained that the treatment advice of the heart team aims for quality of life for patients, but this advice is provided before live consultation of the patient in the heart centre. One cardiothoracic surgeon noticed the lack of information regarding the patient’s personal situation during heart team discussions.
Sometimes, the heart team’s decision doesn’t quite match the real patient. (Respondent 004, cardiothoracic surgeon, 2 years in practice)
Although the respondents clearly stated that SDM includes considering treatment options in patients’ best interest, nearly half of them experienced economic constraints. For example, SDM is limited due to stringent criteria for reimbursement of treatment of severe AS.
TAVR is much more expensive. (Respondent 005, interventional cardiologist, 8 years in practice)
Collaboration with other disciplines is a facilitator of SDM, according to the respondents, and provides a more complete evaluation for tailoring treatment options to patient needs.
Overall, respondents believed that SDM is an improvement for clinical practice. Conversely, most were not aware of the results and the implementation of SDM research. Respondents suggested that informing patients about SDM in advance will improve patients’ preparation for the SDM process.
Often, people are not aware that they have a choice, are even overwhelmed that they have to decide…; thus, I think this is still something to pay attention to. (Respondent 020, nurse practitioner, 15 years in practice)
Relationship with taxonomy of the SDM process
All elements of the four primary themes (figure 2) were structured into the seven categories of the adapted taxonomy of barriers and facilitators to SDM (figure 3). We found no elements relating to decision characteristics, terminology used by health professionals, decision support, view of colleagues, culture of network and capacities (online supplemental 3).
Supplemental material

Identified themes structured in taxonomy. Adapted from the adapted taxonomy for barriers of and facilitators to shared decision-making.7 AS, aortic stenosis; SDM, shared decision-making.
Discussion
This study provided insight into professionals’ perceptions of and experiences with SDM in the treatment of symptomatic patients with severe AS. The results show that not all professionals consider patient participation as an element of SDM: some valued and even expected patient participation in deciding on the treatment, while others did not attribute a very active role to the patient. Generally, professionals considered patient knowledge and their opinion of treatment to be essential for SDM. However, a discrepancy between patients’ wishes and realistic treatment options could be a limiting factor. Also, professionals explained that not knowing the patient’s goals and preferences for health improvement hinders SDM. While an active patient role for SDM was valued, professionals perceived that patients’ characteristics (eg, age and ability to process information) and patients’ unawareness of SDM complicate patient participation. Overall, it was suggested that improving the SDM process is a shared responsibility for patients and all professionals involved in the DM process for severe AS.
Although knowledge about SDM in cardiology is expanding,3 13 24–26 the results of this study demonstrate that not all professionals are familiar with patient participation in SDM. Some professionals perceived SDM as the multidisciplinary process for best treatment without a specified patient role, while others stressed the importance of patient participation in electing treatment options. These results are in line with those of previous studies which indicate that some core principles of SDM are not always met.6 16 17 Subsequently, patients are often not regarded as part of the healthcare team.27 28
Agreeing with previous research,16 the results of this study show that professionals consider patient education to be sufficient for empowering patients in SDM. Conversely, professionals struggle to make highly complex treatment decisions part of SDM and to embed patients’ goals and expectations for health improvement. However, to empower patients in their DM role, other factors do play a role. For example, patients undervalue their ability to comprehend complex medical information and undervalue the complementary expertise that they can bring to the SDM process.7 29
Consistent with previous studies, we found that professionals have doubts about older patients’ willingness and ability to participate in SDM.6 However, while the challenges of SDM with older patients are known, older patients in cardiology and other domains have been shown to have good insight into their own condition, and preferences and views on SDM.2 7 24–26 Therefore, the participation of older patients in SDM and SDM research is possible and relevant.
Professionals perceived that previous communication and information about patient preferences were not available for DM in heart teams or prior to consultations in heart centres. Other studies also indicated that in many heart centres the treatment plan is developed without the presence of the referring cardiologist and without meeting the patient in the outpatient clinic beforehand.27 28 The absence of this important patient information complicates the SDM process. Additionally, knowledge on patients’ background and health status guides both the total SDM process and the discussion of tailor-made goals and decisions during consultations.7
To our knowledge, this is the first study that provides broad insight into the perceptions and experiences of professionals regarding SDM in severe AS. This study was strengthened by using a structured interview guide, two independent coders and a member check to maximise the reliability and integrity of the results. However, the results of this study should be interpreted in light of some limitations. First, patients were not involved in the design or analysis of this study. However, this study is part of a comprehensive research project on SDM that involves professionals’ views and patients’ and informal caregivers’ views of SDM, which will be addressed in a later study. Second, to direct the interviews regardless of the professionals’ personal definition of SDM, we mentioned the definition of SDM that was proposed by Elwyn et al.3 13 Third, this study is applicable to the Dutch practice setting; thus, extrapolation to other international practice settings for treatment of severe AS may not be possible.
This study highlights the increasing need for further integration of SDM at the patient, professional and organisational levels (figure 4). Treatment options for symptomatic AS are evolving, and patients are willing to be involved in DM.30 Recommendations in guidelines are also driven by the growing evidence that SDM improves clinical practice and patient care pathways.2 This study highlights the need for training to increase professionals’ familiarity with SDM and to emphasise the utility of SDM in severe AS. The embedding of SDM in medical and nursing curricula will contribute to the necessary skills. Collaboration initiatives in cardiology are also necessary to review SDM in current practice and to develop a common view on SDM and patient participation in the treatment of severe AS. To further integrate SDM in daily practice, decision aids for severe AS (https://sharedcardiology.org/tools/) should be considered, while question prompts can help to improve patient participation.2 Additionally, integrating information in the pathway for severe AS according to the principles of SDM requires a change in current pathways (eg, the documentation and availability of information regarding patient preference and goals earlier in the referring process). This integration will frame the goal-and-decision talk during consultations. To combine both the patient and the professional views for improvement of SDM, future research should incorporate attention for patient and informal caregiver preferences for the SDM process. Observational studies must provide insight into eliciting patient goals and exploring how to tailor the SDM process in the treatment of severe AS to patient needs. Implementation research must focus particularly on interventions to facilitate SDM (eg, the combination of inpatient and outpatient decision aids and the incorporation of patient-reported outcomes). Additionally, increasing awareness of and addressing organisational barriers to the implementation of personalised care in the DM process of severe AS are important for SDM research.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Recommendations for SDM improvement in the treatment of severe AS. AS, aortic stenosis; SDM, shared decision-making.
Despite professionals’ willingness to incorporate SDM in DM for severe AS, professionals perceive the implementation of SDM to be challenging. Professionals struggle to make highly complex treatment decisions part of SDM and to embed patients’ expectations of treatment and patients’ preferences. Additionally, organisational constraints complicate the SDM process. To ensure sustainable high-quality care, professionals should increase their awareness of patient participation in SDM. Collaboration in the pathway for DM in severe AS is required to support the documentation and availability of information according to the principles of SDM.
Key messages
What is already known on this subject?
Professional guidelines for the treatment of symptomatic patients with severe aortic stenosis (AS) recommend shared decision-making (SDM) for the integration of preferences and values of those involved.
The implementation of SDM in daily practice is influenced by various barriers and facilitators.
What might this study add?
Not all professionals consider patient participation to be an element of SDM.
Professionals struggle to make highly complex treatment decisions in patients with severe AS part of SDM and to embed patients’ expectations of treatment and patients’ preferences.
How might this impact on clinical practice?
Results highlight the need for training and education to increase professionals’ familiarity with SDM and to emphasise the utility of SDM in severe AS.
Multidisciplinary collaboration in the pathway for decision-making in severe AS is required to support the documentation and availability of patient information according to the principles of SDM.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants but the Medical Ethics Research Committees United (MEC-U) confirmed that the Dutch Medical Research Involving Human Subjects Act did not apply to the research project (W20.039). Therefore, approval by the committee was not required and exempted this study. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors acknowledge the interview participants for their time and input.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors JJAMvB-P, MMNM, NJMvdM, MCF and AJBMdV conceived the idea for the study and participated in the design. JJAMvB-P and JBLvdM performed the interviews and the analysis of data. JJAMvB-P, JBLvdM, MCF and AJBMdV contributed to interpretation of data. JJAMvB-P drafted the initial draft of the manuscript, which was revised based on the input of all authors. All authors reviewed and approved the final draft. JJAMvB-P is responsible for the overall content as the guarantor.
Funding This work was funded by the Amphia Hospital Science Funding (grant 2020-1-010 DiMAS-2).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.