Article Text

Abstract
Objective In paediatric pulmonary arterial hypertension (PAH), the effectiveness of add-on combination PAH-therapy has not yet been systematically studied. The purpose of this study was to determine the effect of sildenafil add-on therapy in paediatric PAH patients treated with bosentan.
Methods In this observational study within a national paediatric patient cohort, follow-up data of 24 consecutive paediatric PAH patients initially treated with bosentan monotherapy and prospectively followed at the Dutch national referral centre for paediatric PAH in 2007–2013, were reviewed. Patients received add-on sildenafil therapy in case of clinical worsening.
Results Fifteen children received add-on sildenafil therapy; nine remained on bosentan monotherapy. Patient characteristics, 6-minute walk distance (6MWD), WHO functional class (WHO-FC), N-terminal pro-Brain Natriuretic Peptide (NT-proBNP), and haemodynamic measurements at bosentan start were similar in both patient groups. In children with clinical worsening, sildenafil add-on therapy improved 6MWD at 5, 10, 15 and 21 months of follow-up, improved WHO-FC at 10, 15 and 21 months and stabilised NT-proBNP. Patients who received add-on sildenafil therapy had more advanced disease progression during bosentan monotherapy. Despite that, they had better or, at least, no worse survival compared to patients who remained on bosentan monotherapy.
Conclusions In children with PAH, sildenafil add-on therapy indicated by clinical deterioration on bosentan monotherapy, was associated with a significant improvement of WHO-functional class and 6MWD. Despite clinical deterioration on bosentan monotherapy, patients receiving sildenafil add-on therapy, had either better or, at least, no worse survival than patients remaining on bosentan monotherapy.
Statistics from Altmetric.com
Introduction
Pulmonary arterial hypertension (PAH) is a disease characterised by pulmonary arterial remodelling leading to an increased pulmonary vascular resistance and pressure, and eventually right ventricular failure. In children, PAH is a severe disease for which an estimated untreated survival of 10 months has been reported.1
In the past decades, three types of PAH-targeted therapies have been introduced, acting on three separate disease pathways: prostacyclin derivates, phosphodiesterase-5 inhibitors and endothelin receptor antagonists.2 Outcome in children with PAH has been reported to be improved since the introduction of PAH-targeted therapy.3
However, contemporary survival rates in the era of PAH-targeted therapy are still unfavourable with 1, 3 and 5-year survival ranging 86–100%, 71–88% and 66–72%, respectively, for idiopathic and heritable PAH (IPAH/HPAH), and 87–96%, 87% and 81%, respectively, for PAH associated with congenital heart disease (PAH-CHD).3–6 Furthermore, PAH-targeted monotherapy initially leads to clinical improvement in children, but this effect wears off over time.3 ,7 Therefore, more aggressive treatment may be necessary.
A combination of different types of PAH-targeted therapies, targeting more than one disease pathway, may improve outcome further.8 PAH-targeted add-on therapy has been demonstrated to be beneficial in adult PAH patients, improving WHO functional class (WHO-FC), 6-minute walk distance (6MWD), haemodynamics, N-terminal pro-Brain Natriuretic Peptide (NT-proBNP) and time to clinical worsening.9–12 However, the effect of add-on therapy has not yet been evaluated in children.
The current observational study evaluates the effect of sildenafil (a phosphodiesterase-5 inhibitor) add-on therapy to bosentan (an endothelin receptor antagonist) monotherapy in children.
Methods
In The Netherlands, all paediatric PAH patients are referred to the University Medical Centre Groningen, the national referral centre of the Dutch National Network for Paediatric Pulmonary Hypertension. Here, diagnosis of PAH is confirmed by heart catheterisation, treatment strategies have evolved according to the ‘ESC guidelines for the diagnosis and treatment of PAH’, and all patients are regularly seen on standardised follow-up visits. Our institutional human research committee approved the Dutch national paediatric PAH patient registry and its observational studies. Patients or their legal guardians provided written informed consent.
In The Netherlands, paediatric PAH patients in WHO-FC II-III who do not qualify for calcium channel blocker therapy are started on PAH-targeted therapy. All consecutive paediatric iPAH/HPAH and PAH-CHD patients seen at the Dutch national referral centre from 2007 to 2013 who were on, or were initiated on, bosentan monotherapy, were included in this observational study; including Down syndrome patients, judged able to reliably perform a 6MWD based on already performed tests. Before the introduction of the paediatric formulation, bosentan was dosed according to body weight: 31.25 mg (10–20 kg), 62.5 mg (20–40 kg), or 125 mg (>40 kg) twice daily, and at 2–4 mg/kg twice daily thereafter.7 ,13 Patients received add-on sildenafil therapy at clinical worsening despite bosentan monotherapy, defined as either a rise in WHO-FC to reach III-IV, or a sustained WHO-FC II-III and judged to have clinical deterioration including a sustained decrease in 6MWD (ca. 50 m or more; if patient's age allowed) or sustained rise of NT-proBNP (ca. 200 ng/L or more). Patients that did not meet these criteria, for instance patients that had a rise in NT-proBNP or a decrease in 6MWD but with an improving WHO-FC or WHO-FC I, or patients with a one-time drop in 6MWD that did not sustain, did not receive sildenafil add-on. Sildenafil was up-titrated within 1 month up to doses of 10 mg three times daily for patients <20 kg and 20 mg three times daily for patients of >20 kg.
All patients started on bosentan monotherapy (at baseline). During their disease course, part of the group remained clinically stable on bosentan monotherapy, and did not receive additional therapy, and part of the group developed clinical worsening during follow-up and received sildenafil add-on therapy (figure 1). Therefore, patients could be retrospectively separated into two groups: (1) patients who remained on bosentan monotherapy, and (2) patients who were initiated on bosentan monotherapy and later received add-on sildenafil therapy.

Study timeline. 1All patients were clinically evaluated before the start of bosentan therapy. 2Thereafter, all patients started on bosentan monotherapy. 3Patients showing no clinical worsening remained on bosentan monotherapy. 4,5Patients showing clinical worsening received add-on sildenafil therapy. 6Before the start of add-on sildenafil therapy WHO-FC, 6MWD and NT-proBNP were determined. 7Follow-up time (for survival analysis) was taken from the initiation of bosentan monotherapy to the end of follow-up (death, transplantation, or last follow-up visit)8 for all patients. All patients had 3–6 monthly follow-up visits during their follow-up period, at which WHO-FC, 6MWD and NT-proBNP were determined.
Baseline evaluation and standardised follow-up
PAH was diagnosed by cardiac catheterisation showing elevated mean pulmonary arterial pressure (mPAP) ≥25 mm Hg, pulmonary capillary wedge pressure (mPCWP) ≤15 mm Hg and elevated pulmonary vascular resistance (PVRi) ≥3 Woods Units·m2 in all but one patient. In this latter patient, PAH-CHD was confirmed by echocardiographic measurement of a right to left shunt through a cardiac defect, in the absence of LV-dysfunction.
Baseline parameters were evaluated before the start of bosentan therapy and included invasive haemodynamic measurements, WHO-FC, 6MWD and NT-proBNP. All patients had standardised follow-up visits every 3–6 months at the national referral centre, at which WHO-FC, 6MWD and NT-proBNP were determined.
Statistical analysis
Data are presented as mean ±SD, median (IQR) or number (percentage) of patients, as appropriate.
For analysis of the add-on sildenafil effect, follow-up visits were categorised within follow-up periods of 3–7, 8–13, and 13–18 months after sildenafil add-on, and at 6-month intervals thereafter. The last of multiple follow-up visits from within a period was chosen. Follow-up parameters were compared to their value measured before sildenafil add-on using paired samples t test or Wilcoxon Signed Rank Test.
Patient characteristics, haemodynamic and functional parameters before bosentan start, were compared between patients who received sildenafil add-on therapy and patients remaining on bosentan monotherapy, using t tests, Mann–Whitney U tests and χ2 tests.
The disease course of both groups while on bosentan monotherapy was depicted by plotting the mean WHO-FC, 6MWD and NT-proBNP before bosentan start, at their peak value during bosentan monotherapy (highest 6MWD, lowest WHO-FC and NT-proBNP) and at the end of bosentan monotherapy (for the patients who remained on bosentan monotherapy, ie, end of follow-up, for the patients who received sildenafil add-on therapy, ie, measurement before sildenafil add-on).
Survival from bosentan monotherapy initiation to the last follow-up visit or endpoint (death or (heart-) lung transplantation) was depicted with a Kaplan–Meier curve. Considering follow-up time and number of endpoints, the survival analysis was truncated at 7 years (75th percentile of follow-up time). Two-sided analyses were performed using SPSS V.18.0 (SPSS, Chicago, Illinois, USA). Level of significance was set to 0.05.
Results
Between 2007 and 2013, there were 59 children with IPAH/HPAH or PAH-CHD who were prospectively followed at the Dutch national referral centre; 11 IPAH/HPAH patients and 13 PAH-CHD patients had or were initiated on bosentan monotherapy and included in this study (figure 2). The latter included 12 patients with a shunt and one with a corrected post-tricuspid shunt (table 1). The patients had severe PAH, with high mPAP and PVRi, without signs of pulmonary venous congestion. WHO-FC was predominantly III before start of bosentan monotherapy (54%). Median follow-up time was 5.5 (3.6–7.2) years.
Baseline characteristics
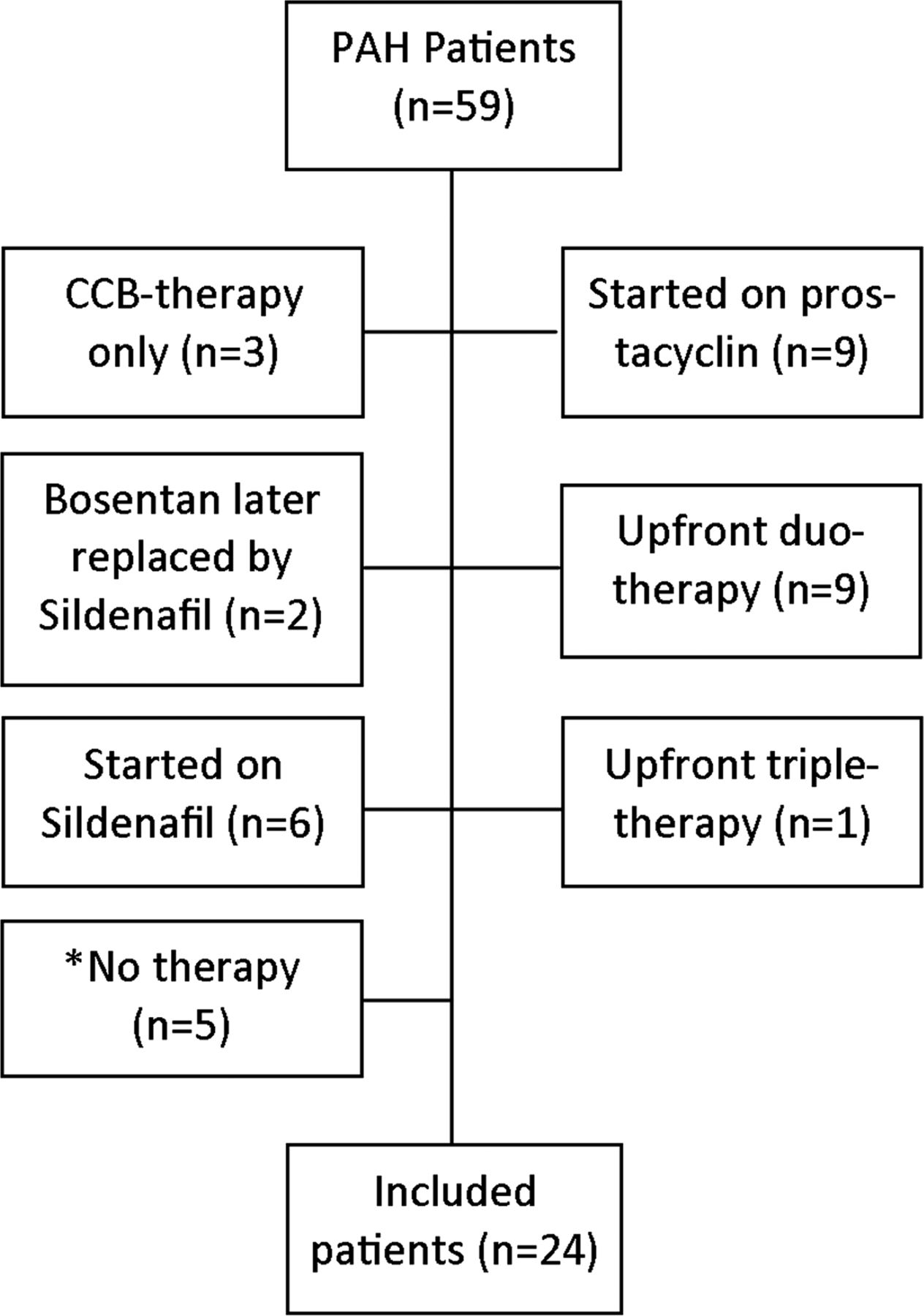
Patient inclusion. Flow chart describing patient inclusion. Within the study period (2007–2013) 59 PAH patients were seen at the Dutch national referral centre. Of these patients, 24 were initially on bosentan monotherapy and were included in this study. *Patients received no therapy due to early death or a less progressive disease not warranting PAH-targeted therapy according to contemporary treatment guidelines.
Of these 24 patients, 15 became eligible for sildenafil add-on therapy during follow-up, based on the criteria described in the methods. These received sildenafil add-on therapy after a median of 30.7 (10.3–77.2) months from initiation of bosentan monotherapy. The remaining nine patients remained on bosentan monotherapy.
Three patients with sildenafil add-on therapy received additional prostacyclin therapy later during follow-up: two because of sustaining WHO-FC IV despite sildenafil add-on therapy, respectively 8.0 and 39.7 months after the start of sildenafil add-on therapy, and one because of clinical deterioration to WHO-FC IV after 40.3 months of sildenafil add-on therapy. Eight of the nine patients remaining on bosentan monotherapy did not deteriorate to WHO-FC IV, not warranting additional prostacyclin therapy. One Eisenmenger patient had a rise in WHO-FC to IV during bosentan monotherapy but did not receive add-on sildenafil therapy nor additional prostacycline therapy while awaiting heart-lung transplantation.
Sildenafil add-on effect
The effect of sildenafil add-on therapy was determined in the 15 patients receiving sildenafil add-on therapy. Three patients received additional prostacyclin therapy (8.0, 39.7, and 40.3 months after sildenafil add-on, respectively) and were censored at that moment, to not influence the analysis of sildenafil add-on treatment effect.
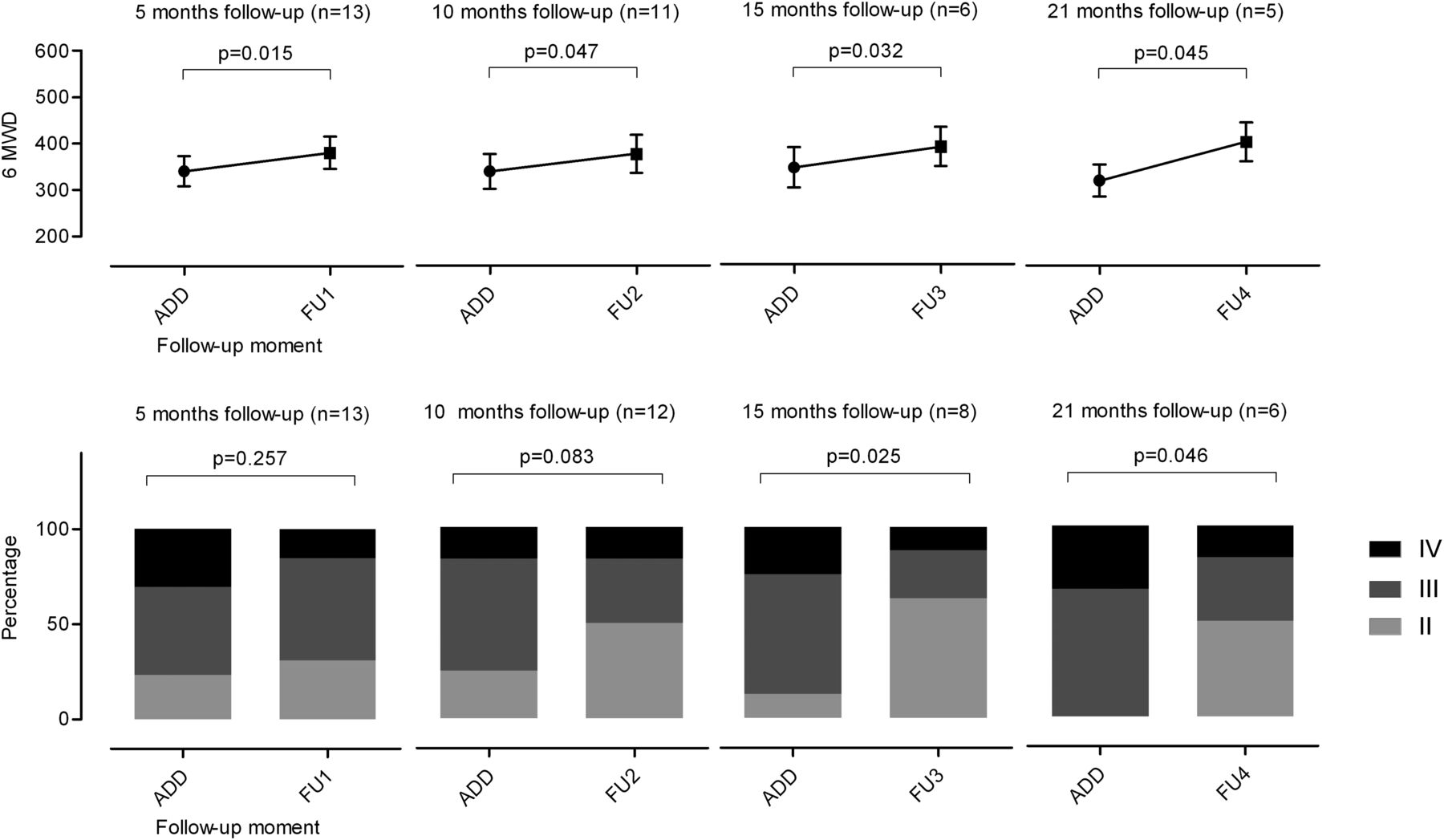
WHO-FC, 6MWD and log NT-proBNP at four follow-up moments, respectively 4.5 (3.5–5.1), 9.7 (9.0–11.7), 15.4 (15.0–16.0) and 21.3 (20.2–21.7) months after sildenafil add-on, were compared to their value before addition of sildenafil therapy. There was a significant improvement in 6MWD and WHO-FC after addition of sildenafil (figure 3). There was a slight decrease in NT-proBNP levels, not reaching statistical significance. After these four follow-up moments, seven patients remained in follow-up, however, there was insufficient data to perform this specific analysis during longer-term follow-up.
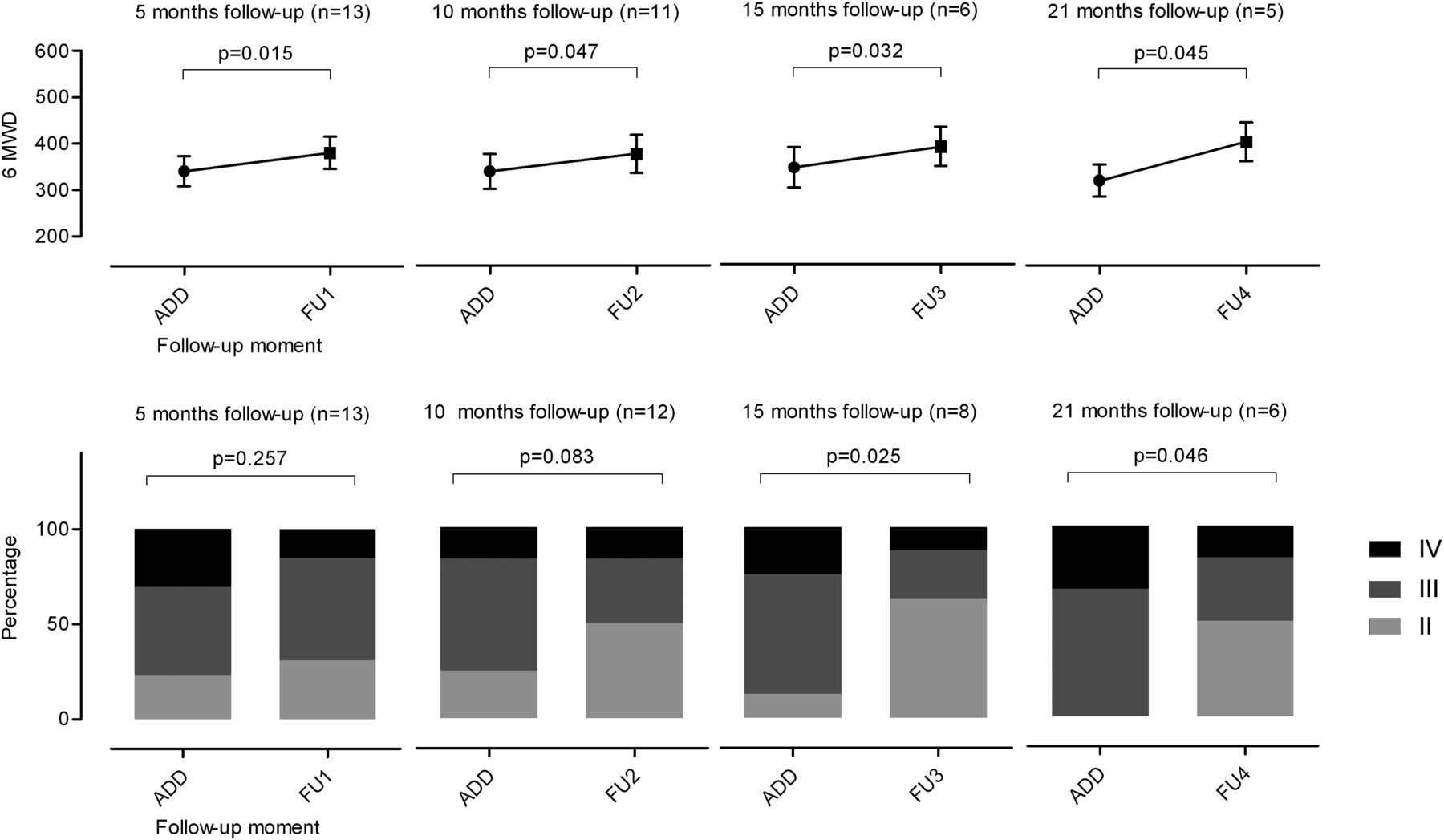
Treatment effect of sildenafil add-on therapy. The mean (SE) 6MWD and WHO-FC, respectively, at 5 (FU1), 10 (FU2), 15 (FU3) and 21 (FU4) months after sildenafil add-on, compared to their own baseline value, using paired samples t test (6MWD) and Wilcoxon signed rank test (WHO-FC). For each graph, the add moment includes only the patients for whom the respective follow-up data was available, in order to compare follow-up values to the patient's own baseline.
Comparison between treatment groups
The 15 patients receiving sildenafil add-on therapy were compared to the nine patients remaining on bosentan monotherapy. At the start of bosentan, there were no differences in disease characteristics and haemodynamic measurements between these two patient groups (table 1).
After initiation of bosentan monotherapy, WHO-FC, 6MWD and NT-proBNP significantly improved in both patient groups (figure 4). In patients who later qualified for sildenafil add-on, bosentan initiation seemed to be associated with less pronounced initial improvements of 6MWD, WHO-FC and NT-proBNP when compared to the improvements in patients who remained on bosentan monotherapy. These differences, however, did not reach statistical significance. After this initial improvement, the 6MWD decreased and NT-proBNP increased significantly during follow-up in both patient groups. These changes appeared to be more severe and more rapid in the patient group that later on received sildenafil add-on. WHO-FC increased significantly over time after the initial improvement in the patients who qualified for sildenafil add-on therapy. It did not increase significantly in the patients who remained on bosentan monotherapy, even though the mean time between WHO-FC improvement and the end of follow-up in these patients was significantly longer than the time between improvement and sildenafil add-on in the sildenafil add-on group (p=0.011).

Change in clinical parameters during bosentan monotherapy stratified for treatment group. The mean (SE) WHO-FC, 6MWD and 10Log NT-proBNP was determined for both treatment groups at three time points: * before bosentan treatment, # at their peak value, and $ at the end of bosentan monotherapy (= end of follow-up for the patients that remained on bosentan monotherapy [○], or moment of sildenafil add-on for the patients that received add-on sildenafil therapy [●]). These values were plotted to the mean follow-up time (months) at which these measurements took place. Expressed as mean (SE), error bars indicate SE of the mean, p-values from paired samples t test, or Wilcoxon signed rank test, as appropriate. ● Sildenafil add-on treated patients during the period of bosentan monotherapy, ○ bosentan monotherapy-treated patients.
Within the truncated follow-up period of 7 years, five patients reached a predefined endpoint. Within the group of patients remaining on bosentan monotherapy four patients died acutely; two patients (PAH-CHD, baseline WHO-FC IV; IPAH/HPAH, baseline WHO-FC II, respectively) died because of acute severe haemoptysis and one PAH-CHD patient (baseline WHO-FC II) due to convulsions followed by acute circulatory failure. Because of acute death, not preceded by a period of clinical deterioration, these three patients did not receive sildenafil add-on. Finally, one PAH-CHD patient (baseline WHO-FC IV) died during a complicated heart-lung transplantation procedure, and this Eisenmenger patient did not receive sildenafil add-on while awaiting transplantation. Of the patients receiving sildenafil add-on therapy, one PAH-CHD patient (baseline WHO-FC IV) had successful emergency heart-lung transplantation after life-threatening pulmonary haemoptysis.
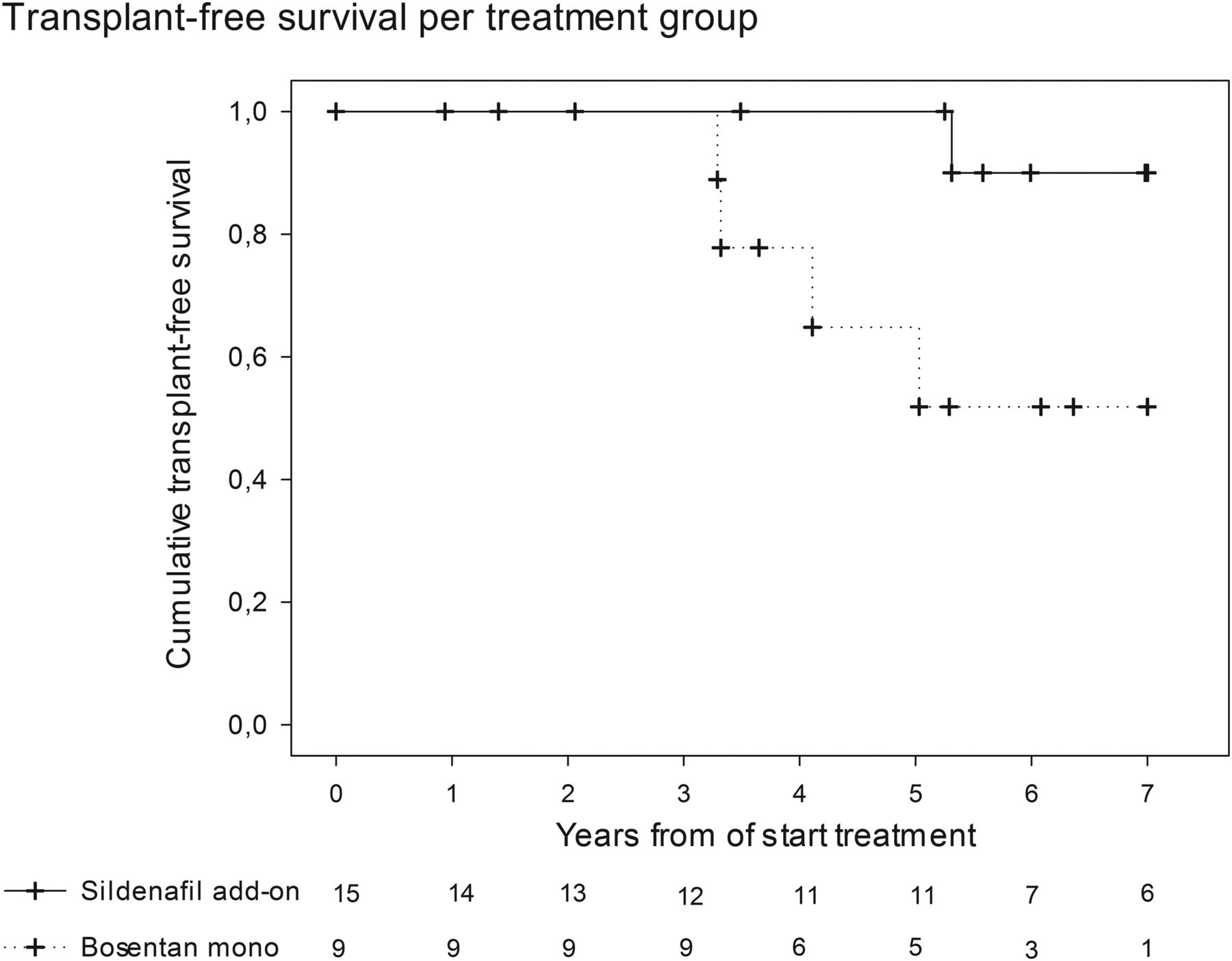
Transplant-free survival was plotted in figure 5, stratified for treatment group. Patients who needed sildenafil add-on therapy had better or at least did not have worse survival than patients who remained on bosentan monotherapy. Three add-on sildenafil patients received additional prostacyclin therapy which might additionally favour their survival. Excluding these three patients from the survival analysis did not change the curves.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Survival separated for treatment groups. Transplant-free survival from start of bosentan monotherapy to last follow-up visit or endpoint (death or transplantation).
Adverse drug reactions
There were no serious adverse drug reactions in this patient group. Bosentan use did not lead to significant elevations of liver enzymes (>3 times upper limit of normal). The additional sildenafil therapy was well tolerated. Discontinuation of bosentan or sildenafil therapy due to adverse effects did not occur in this patient group. Two patients reported dizziness during sildenafil treatment, however, not related to initiation or dosage changes of sildenafil.
Discussion
Addition of sildenafil therapy to bosentan monotherapy increased 6MWD, improved WHO-FC and led to NT-proBNP stabilisation in children with PAH. Despite significant clinical deterioration while on bosentan monotherapy, the paediatric PAH patients who received sildenafil add-on therapy had better or, at least not worse, transplant-free survival compared with those remaining on bosentan monotherapy.
Despite the introduction of PAH-targeted therapies, outcome of paediatric PAH remains poor.3–6 Goal-oriented treatment, commonly adopted in the treatment of adult PAH, has been hampered by the lack of well-defined treatment targets for paediatric patients. The paediatric Task Force of the World Symposium of PH in Nice, 2013, recently proposed paediatric treatment targets to adopt a goal-oriented, add-on treatment strategy in children. However, the effect of add-on treatment in children with PAH has not been systematically studied yet. The current study evaluated the effect of sildenafil add-on to bosentan therapy.
Sildenafil induces vasodilatation, exerts antiproliferative effects, and enhances systolic adaptation in the pressure-loaded RV.14–16 Sildenafil has been shown to improve 6MWD and haemodynamics in paediatric PAH.17 ,18 We now additionally show that sildenafil add-on to bosentan background therapy leads to clinical improvement in paediatric PAH, reflected by improvement of 6MWD and WHO-FC.
WHO-FC has been shown a predictor of survival in paediatric PAH in several studies.3 ,5 ,19 In adult PAH, 6MWD is frequently used as an endpoint in clinical trials, and was suggested to predict survival.20–23 Improvement of 6MWD is regarded a clinically meaningful effect in patients with PAH. In children from 6 to 8 years of age, 6MWD has been demonstrated to be reproducible. Also in patients with Down syndrome, the 6MWD was shown to be reproducible after two practice runs.24 Therefore, the improvement in 6MWD and WHO-FC, that we found in this study in children with PAH upon sildenafil add-on therapy, can be considered indicative for a beneficial effect on the patients’ disease course and long-term outcome.
In order to further evaluate sildenafil add-on therapy effect compared with bosentan monotherapy, we retrospectively compared two patient groups in this study. It should be emphasised that the group of patients that remained on bosentan monotherapy in the current study, represents a selection of patients who performed relatively well on bosentan monotherapy, with 67% patients who were not treatment-naive at the start of the study period and, therefore, may have a more favourable survival. Even so, despite more rapid clinical deterioration on bosentan monotherapy, the patients who received sildenafil add-on therapy had better or at least comparable and not worse survival compared with patients remaining on bosentan monotherapy.
Recently, a randomised, double-blind, placebo-controlled trial and open-label extension study, STARTS-1 and STARTS-2, studied the effects of sildenafil in paediatric PAH.18 Its follow-up data suggested that the use of high-dosed sildenafil was associated with less favourable survival compared to the use of lower-dosed sildenafil.25 Based on the results of both studies, the EMA has approved the use of sildenafil in children noting that the higher dosage is not recommended, whereas, the United States Food and Drug Administration (FDA) has issued a warning against the use of sildenafil in children for PAH.26 In the current study with a median follow-up time after sildenafil add-on of 1.5 (1.1–3.9) years, there were no adverse drug reactions to sildenafil given as add-on therapy to bosentan therapy and dosed according to the advice of the EMA, with no adverse effect on outcome in paediatric PAH. It is, however, important to realise that in STARTS-2 more deaths in the higher-dose groups occurred only after 2 years of follow-up.18
Initiation of bosentan monotherapy led to an initial improvement in 6MWD, WHO-FC and NT-proBNP in all patients. However, this improvement was followed by deterioration in both groups during longer-term follow-up, even in patients remaining on bosentan monotherapy (figure 4). This clinical deterioration at longer-term follow-up after initial improvement, has been shown before in paediatric and adult PAH.3 ,7 ,27 ,28 These results suggest that add-on therapy is often necessary after a period of treatment with PAH-targeted monotherapy, but also that earlier add-on treatment, preventing this longer-term deterioration, may improve its beneficial effects. For instance, the patients on bosentan monotherapy that eventually deteriorated, could either not receive sildenafil add-on because of acute deterioration and death, or did not meet all the criteria to add sildenafil treatment as used in this study. But given the outcome of these patients they might have benefitted from sildenafil add-on therapy at an earlier stage. This is supported by recent paediatric data and indicates that PAH patients on combination therapy show improved survival compared to patients on monotherapy.29 Therefore, the authors would recommend more aggressive treatment for paediatric PAH with more early add-on therapy, for instance, upon lack of clinical improvement instead of clinical deterioration. Such goal-oriented treatment strategy has been shown to improve outcome in adult PAH.8 Therefore, adopting the recently proposed treatment goals for paediatric PAH patients may help to accelerate treatment add-on, and improve current outcome in paediatric PAH.30
It should be addressed that the current study is limited by its retrospective character, not allowing for a controlled treatment efficacy analysis. Patients requiring sildenafil add-on therapy, based on defined clinical deterioration criteria, were compared to a selected group of patients, not meeting these criteria and thus remaining on bosentan monotherapy. This may seem a controversial study design. However, in the absence of randomised controlled trials in paediatric patients with PAH, this comparison provides unique insights in the disease course of patients with similar baseline characteristics treated with either bosentan monotherapy or sildenafil add-on therapy. This is despite the used control group seeming to be a selected group of patients doing well on monotherapy. Such bias might be expected to favour survival in this control group. Therefore, the observation that the sildenafil add-on patients did not have worse (or maybe even better) survival, than those on bosentan monotherapy, might be regarded an enforcement of the effect of add-on sildenafil. The relatively small patient numbers may have limited the analysis of NT-proBNP response to treatment. Furthermore, the effect of age on the treatment response could not be studied due to the small patient numbers. Plasma levels of sildenafil, potentially affected by coadministration with bosentan, were not available for this study. Nevertheless, we think the current data provide reasonable robust insights in current add-on therapy practice and the effects of sildenafil add-on therapy to bosentan background therapy in paediatric PAH patients, which is data that was lacking so far.
Sildenafil add-on to bosentan background therapy appears to be safe and beneficial in paediatric PAH. This treatment strategy, in children who clinically deteriorated on bosentan monotherapy, was associated with significant improvement of WHO-functional class and 6MWD. Despite their clinical deterioration on bosentan monotherapy, children who received sildenafil add-on therapy seemed to have a better or at least no worse survival compared to patients who, relatively stable, maintained bosentan monotherapy. Nevertheless, randomised, double-blind, placebo-controlled, add-on sildenafil studies are required to really prove its treatment efficacy, and also longer-term follow-up data for more robust safety analyses.
Key messages
What is already known about this subject?
-
In paediatric pulmonary arterial hypertension (PAH), the introduction of PAH-targeted therapies led to an improvement of outcome. However, contemporary survival rates for paediatric PAH are still unfavourable. PAH-targeted add-on therapy has been demonstrated to be beneficial in adult PAH patients, improving WHO functional class (WHO-FC), 6-minute walk distance (6MWD), haemodynamics, N-terminal pro-Brain Natriuretic Peptide (NT-proBNP) and time to clinical worsening. However, the effect of add-on therapy has not yet been evaluated in children.
What does this study add?
-
This study shows that in children with PAH, sildenafil add-on therapy to bosentan monotherapy is clinically beneficial. Sildenafil add-on therapy given because of clinical deterioration on bosentan monotherapy, was associated with a significant improvement of WHO-functional class and 6MWD. Furthermore, despite clinical deterioration on bosentan monotherapy, patients receiving sildenafil add-on therapy had either better or at least no worse survival than patients remaining on bosentan monotherapy.
References
Footnotes
-
Contributors All authors have contributed significantly to the analysis and interpretation of data. JM Douwes, HL Hillege and RMF Berger have drafted the manuscript, all other authors have revised it critically for important intellectual content. All the authors gave final approval of the version to be published.
-
Funding No, this research received no specific funding.
-
Competing interests JM Douwes, MTR Roofthooft, RLE van Loon, M Ploegstra, B Bartelds, and HL Hillege report no conflicts of interest. For his research and consultancy activities, RMF Berger's institution received grants and consultancy fees from Actelion Pharmaceuticals, GSK, Novartis, United Therapeutics, Pfizer and Lilly, outside the submitted work.
-
Ethics approval University Medical Center Groningen institutional review board.
-
Provenance and peer review Not commissioned; externally peer reviewed.