Article Text

Abstract
Objective Late gadolinium enhancement cardiac magnetic resonance (LGE-CMR) imaging is the reference standard for non-invasive assessment of fibrosis. In hypertrophic cardiomyopathy (HCM) patients the histological substrate for LGE is still unknown. The aim of this study was to assess the ability of LGE and strain echocardiography to detect type and extent of myocardial fibrosis in obstructive HCM patients undergoing septal myectomy.
Methods Thirty-two HCM patients (age 60±10) were included in this cross-sectional study and preoperatively examined by speckle-tracking strain echocardiography and LGE-CMR (n=21). Histological fibrosis was classified as interstitial, replacement and total.
Results Histological fibrosis was present in 31 patients. The percentage of total, interstitial and replacement fibrosis was 15(7, 31)%, 11(5, 24)% and 3(1, 6)%, respectively. Reduced longitudinal septal strain correlated with total (r=0.50, p=0.01) and interstitial (r=0.40, p=0.03), but not with replacement fibrosis (r=0.28, p=0.14). Septal LGE was detected in 13/21 (62%), but percentage LGE did not correlate with total fibrosis (r=0.25, p=0.28). Extent of fibrosis did not differ between patients with and without septal LGE (20(9, 58)% versus 14(5, 19)% p=0.41). Patients with ventricular arrhythmias (n=8) had lower septal longitudinal strain and increased extent total and interstitial fibrosis in myectomy specimens, but no differences were demonstrated in LGE. Reduced longitudinal septal strain and increased extent of interstitial fibrosis predicted ventricular arrhythmias independently of age and gender.
Conclusions In myectomised HCM patients, reduced longitudinal septal strain correlated better with interstitial and total fibrosis in myectomy specimens, and was a more powerful tool to predict arrhythmias than LGE.
- Imaging and Diagnostics
Statistics from Altmetric.com
Introduction
Myocardial fibrosis is associated with adverse outcome in patients with hypertrophic cardiomyopathy (HCM)1 ,2 Different histological types of fibrosis are identified3 ,4 Increased synthesis of collagen and remodelling of extracellular matrix components result in an interstitial type of fibrosis which is regarded as an early and disease-specific process in HCM.5 ,6 By contrast, replacement fibrosis may be a result of remodelling of longstanding disease, including ischaemia, induced by small vessel disease.4 ,7
Late gadolinium enhancement cardiac magnetic resonance (LGE-CMR) imaging has become the reference standard for noninvasive assessment of myocardial scarring. Several studies indicate that LGE is associated with ventricular arrhythmia and deterioration of myocardial function in HCM patients.8–11 Furthermore, progression of LGE over time is accompanied by a worsening in New York Heart Association (NYHA) functional class, but the histological substrate of LGE in HCM patients is not finally determined.8 ,12 ,13 A recent study investigated the association between histopathological fibrosis and different LGE-CMR quantification techniques indicating that replacement and also interstitial fibrosis were detectable.14
Strain by speckle-tracking echocardiography measures global and regional myocardial function, and has the ability to detect reduced myocardial function in HCM despite normal LV EF.15–18 LGE is associated with reduced myocardial function, but in HCM patients also regions without LGE have reduced function.19 ,20
To our knowledge, there are no published studies that use histopathology as a standard to compare the ability of the two non-invasive imaging methods to detect myocardial fibrosis. The aim of this study was to investigate the ability of preoperatively performed echocardiographic strain and LGE-CMR to detect type and extent of histological fibrosis in myectomised HCM patients, and relate this to occurrence of ventricular arrhythmias.
Methods
Patient population
One hundred and four HCM patients, with a non-dilated LV with preserved EF and hypertrophy ≥15 mm, referred to Oslo University Hospital, Rikshospitalet, Norway, between November 2001 and September 2009, were evaluated for gradient reduction therapy, and included in this cross-sectional study. Eighty-four patients met the intervention criteria with drug-refractory symptoms, basal septal hypertrophy ≥16 mm, and a resting LV outflow tract gradient (LVOTG) ≥30 mm Hg, or an exercised LVOTG ≥50 mm Hg.20–22 Data from a subgroup of this population have been reported previously.23 ,24 Patients with concomitant coronary artery disease (CAD) or valvular heart disease were considered for basal septal myectomy, and patients without concomitant diseases were considered for percutaneous transluminal septal myocardial ablation (PTSMA).24 Exclusion criteria were prior intervention with PTSMA (n=1) or myectomy (n=0), and myocardial infarction in the basal septal region (n=0). Thirty-seven patients were operated with either isolated myectomy or combined surgery with additional coronary artery bypass graft surgery, and/or heart valvular surgery. Myectomy specimens were available in 32 patients. The myectomy procedures were performed as previously described.21 ,22 LGE-CMRs before myectomy were available in 21 patients. Patients with CAD (coronary artery stenosis ≥50% evaluated at coronary angiography and/or myocardial infarction in another region than basal septum), mild or moderate valvular heart disease unrelated to HCM, patients on antihypertensive therapy, patients with diabetes mellitus without organ complications, and patients with other additional diseases were not excluded. The study complies with the Declaration of Helsinki, and was approved by the Regional Committee for Medical Research Ethics. Written informed consent was obtained from all patients.
Definition of ventricular arrhythmias
Ventricular arrhythmias prior to intervention were registered if patients had (1) previous cardiac arrest with documented ventricular arrhythmias, (2) non-sustained ventricular tachycardia at Holter monitoring and/or (3) unexplained syncope (suspected arrhythmogenic syncope or syncope during exercise).23
Histopathology of myectomy specimens
The specimens were fixed in formalin, and stained with hematoxylin-eosin-saffron and acid fucsin orange-G (AFOG) as previously described.23 A proportion of each specimen fixed in glutaraldehyd was examined with electron microscopy to exclude storage disease. Perivascular fibrosis and myocyte disarray were assessed as present or not, and subendocardial fibrosis was excluded from the analyses. Visual estimates of the areas affected (%area) by interstitial or replacement fibrosis (figure 1) were assessed as previously described.23 The observers (EHS and HS), blinded for clinical data, analysed the AFOG-stained sections in parallel.
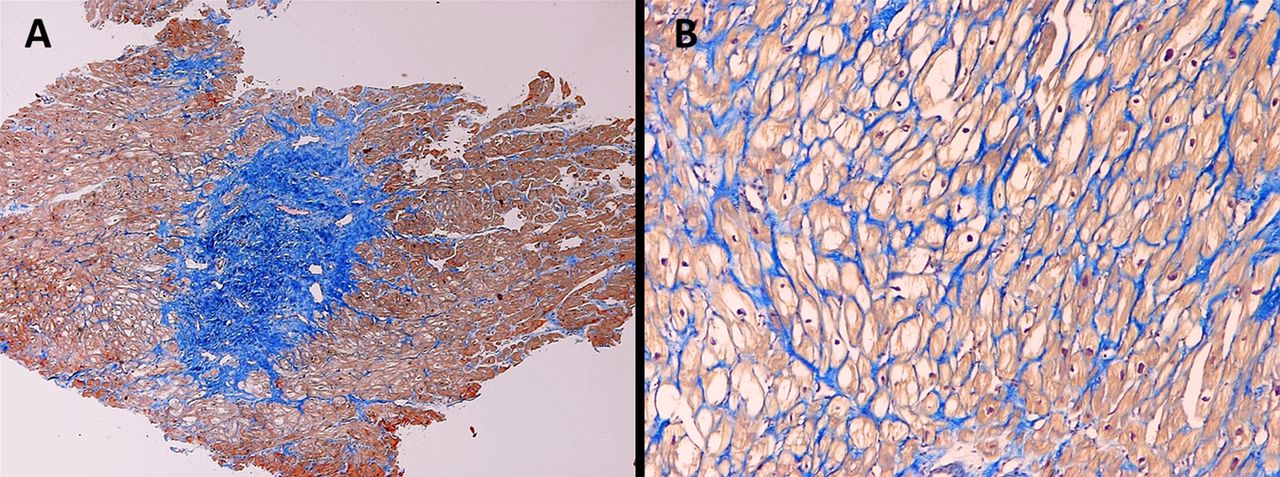
The specimen is taken from the basal part of the ventricular septum in a patient with obstructive hypertrophic cardiomyopathy undergoing myocardial septal myectomy. The sections are stained with acid fucsin orange-G. Blue colour indicates fibrosis/connective tissue. Panel (A) shows replacement fibrosis (×200), and panel (B) shows interstitial fibrosis (×400).
Echocardiography
Transthoracic echocardiography, using Vivid 7 (GE Healthcare, Horten, Norway), was performed 111 (62, 184) days prior to myectomy. The standard echocardiographic measurements were analysed by a single observer, (VMA) and the strain measurements by two observers (KHH and VMA), both blinded for clinical data. 2D and Doppler echocardiographic measurements were performed according to current standards.25 When appropriate, peak resting and/or exercise-induced LVOTG, were measured by continuous-wave Doppler at rest and/or during exercise (bicycle). Maximal wall thickness (MWT) was assessed from parasternal short-axis view, primarily at the level of papillary muscle. The extent of hypertrophy was assessed by Spirito–Maron index and Wigle’s score.
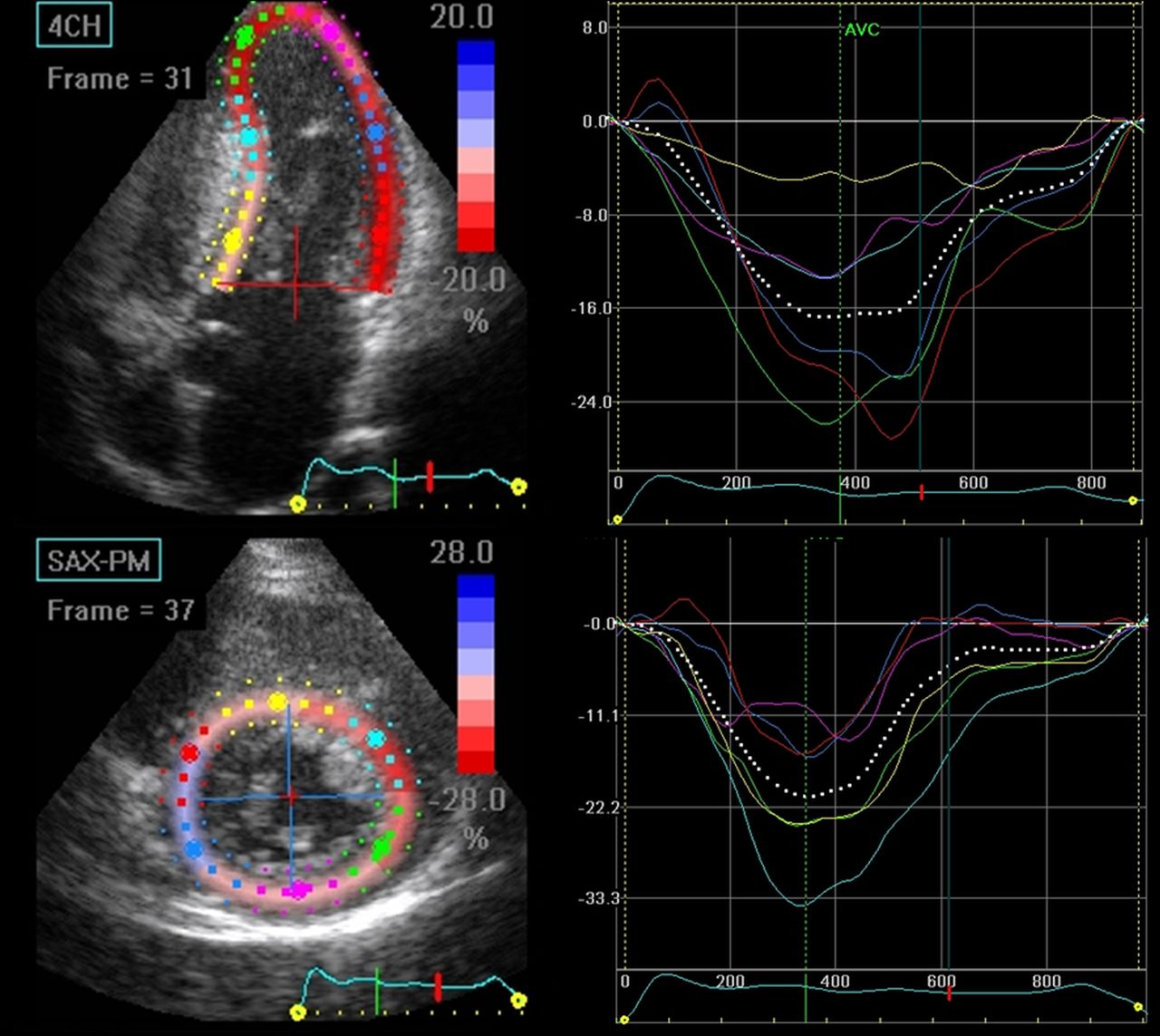
2D strain was measured by speckle-tracking echocardiography as previously described.18 The endocardial contour was traced on an end-diastolic frame, and the software automatically tracked the contour on subsequent frames. Adequate tracking was verified in real time, and to ensure optimal tracking, the endocardial contour and width of region of interest (ROI) was adjusted to fit the average of the myocardial thickness. If segments were automatically excluded by the software, the width of ROI and/or the endocardial contour were manually adjusted to achieve an optimal speckle tracking. Global longitudinal strain was defined as average peak systolic percentage strain in a 16-segments model with 67±24 frames/s. Septal longitudinal strain was defined as mean of peak systolic strain of basal and mid-septal segments from the apical long axis and apical 4-chamber view (figure 2). Global circumferential strain was obtained from papillary muscle level, averaging peak strain in six segments. Septal circumferential strain was defined as mean of peak strain from the anteroseptal and septal segments. A subset of patients (n=18) was additionally investigated with tissue Doppler imaging-derived strain as previously described.17

Strain by speckle-tracking echocardiography taken from a patient with obstructive hypertrophic cardiomyopathy. The upper picture shows longitudinal strain from apical 4-chamber view, and the lower shows circumferential strain from parasternal short-axis view.
CMR
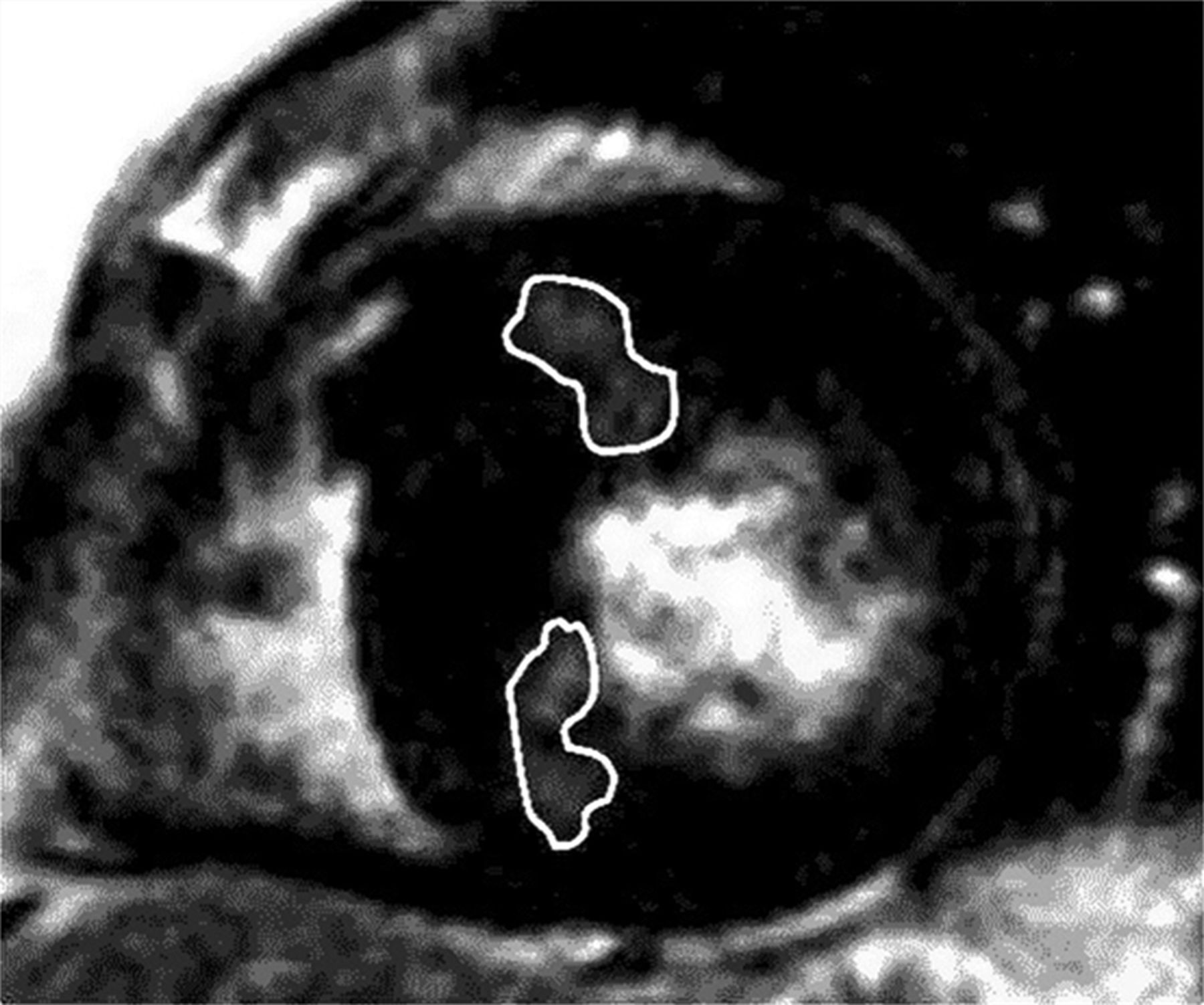
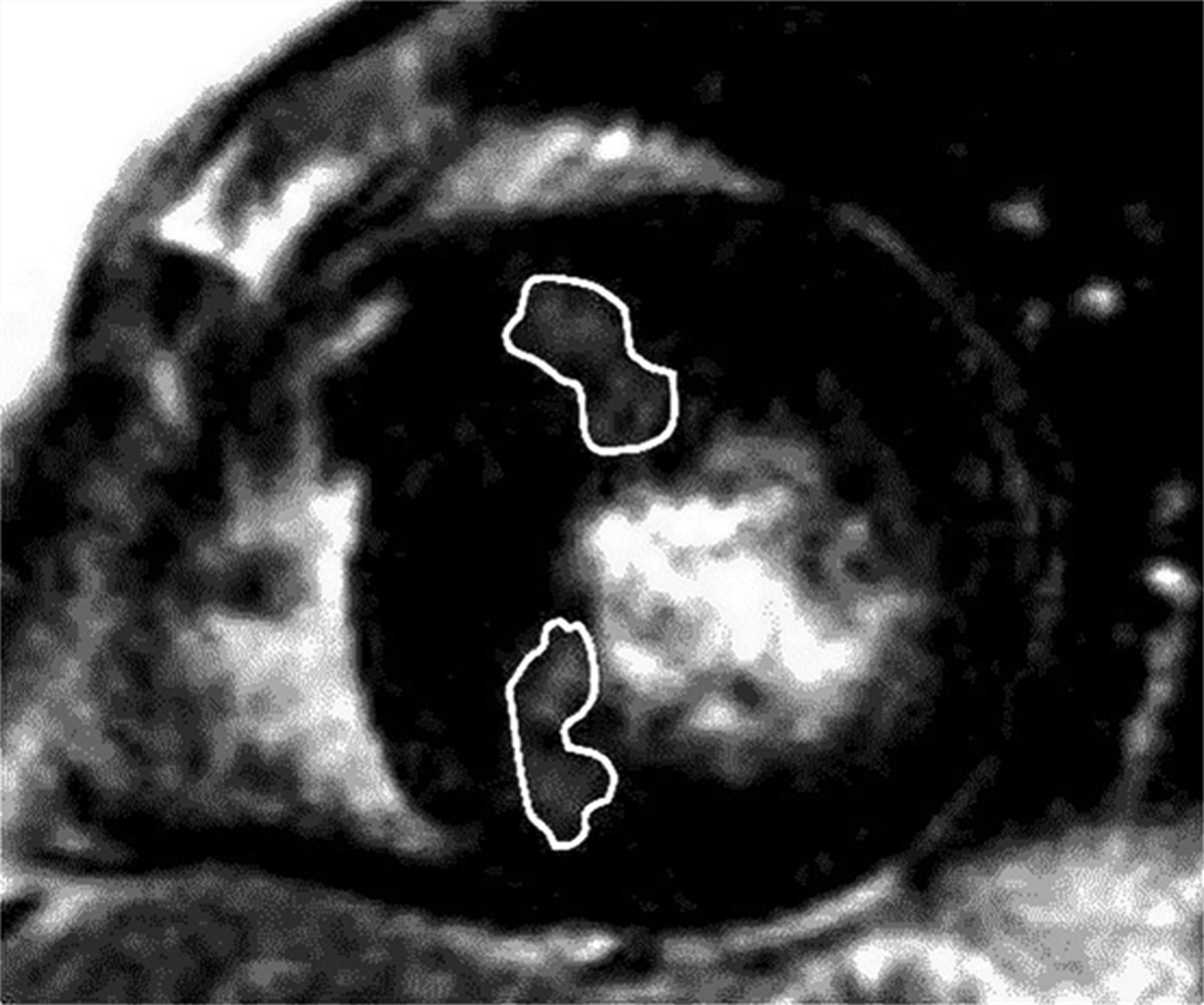
LGE-CMR was performed 6 (2, 60) days prior to myectomy using a 1.5 tesla scanner (Siemens, Erlangen, Germany) and a phased-array body coil. Breath-hold long-axis and short-axis cine images were acquired using an ECG-triggered segmented balanced gradient echo technique. LGE was obtained with multiple short-axis slices covering the entire LV with a slice thickness of 7 mm and an interslice gap of 3 mm, 10–20 min after intravenous injection of 0.2 mmol/kg gadopentetate dimeglumine. A breath-hold segmented magnetisation-prepared turbo gradient echo sequence was used with an inversion time of 210–260 ms. The extent of global LGE was assessed by a visual estimate, using a 17-segment LV model. For each segment, total myocardial area, and areas of LGE were manually drawn (figure 3). The area of LGE was calculated as percentage of the actual segment. CMR examinations 1 year after the procedure to localise the resected area after myectomy (n=13) revealed affection of the basal anteroseptal and inferoseptal segments. Septal LGE was defined as the percentage LGE area of the basal and mid-ventricular anteroseptal and inferoseptal segments. The LV mass was calculated by adding the total myocardial areas of all 17 segments and multiplying by 1.04 g/cm3.26 CMR analyses were performed by an experienced radiologist blinded to clinical data.
{kind=link}
{kind=link}
{kind=link}
LGE-CMR image of a patient with obstructive hypertrophic cardiomyopathy. Upper indicated area demonstrates LGE in the basal anteroseptal segment, and lower indicated area demonstrates LGE in the basal inferoseptal segment. LGE, late gadolinium enhancement; LGE-CMR, LGE cardiac magnetic resonance.
Genetic analyses
Patients were tested for the following mutations: myosin-binding protein C (MYBPC3), β myosin heavy chain (MYH7), regulatory and essential light chains of myosin (MYL2 and MYL3), cardiac troponin T (TNNT2) and I (TNNI3), as previously described.23
Statistics
Data are presented as mean±(SD) or median (25%, 75% percentiles). Comparisons of two groups were performed using unpaired Student t test, or Mann–Whitney U test. Proportions were compared by the Pearson χ2 or Fischer's Exact test. Non-parametric correlation test (Spearman's r) was used to analyse the relation of %area of fibrosis, %LGE and strain. Univariable logistic regression analyses were used to identify predictors of histological fibrosis ≥15% (median value) and of ventricular arrhythmias. Multivariable analyses were performed including variables with p values <0.15 from the univariable analyses, and for the histology analyses CAD, MWT and peak LVOTG were forced in, and for the arrhythmia analyses, age at intervention and gender were forced in. Two-sided p values <0.05 were considered statistically significant. Reproducibility was expressed by intraclass correlation coefficient. All statistical analyses were performed with SPSS (V.18, SPSS, Chicago, Illinois, USA).
Results
Patient characteristics
Characteristics of the study population are presented in table 1. Twenty-three (72%) patients had additional diseases with either CAD (n=17), myocardial infarction (n=4), hypertension (n=14), diabetes mellitus (n=2), and/or other diseases (n=2). Isolated myectomy was performed in 13 patients, and combined surgery in 19 (additional coronary artery bypass graft surgery (n=13) and/or additional valvular heart surgery (n=8)). The patients were treated with β-blockers (n=27), calcium-channel blockers (n=10), disopyramide (n=1), angiotensin-converting enzyme inhibitors (n=3), angiotensin II receptor blockers (n=10) and/or diuretics (n=10). In the total population (n=32), four patients had confirmed HCM disease-causing mutations.
Clinical, echocardiographic and histological characteristics of 32 obstructive HCM patients undergoing myocardial septal myectomy, and of the 21 patients with LGE-CMR imaging available
Histological fibrosis
Thirty-one of 32 patients (97%) had replacement, and 30 (94%) had interstitial fibrosis. The amount of total fibrosis in the myectomy specimens was 15(7, 31)%, of which 11(5, 24)% was interstitial and 3(1, 6)% replacement (table 1). There were no significant differences between patients with (n=23) or without (n=8) additional diseases with respect to total (p=0.57), interstitial (p=0.31), or replacement fibrosis (p=0.25).
A 61-year-old genotype-negative female had no global or septal LGE and no fibrosis in the myectomy specimen. Prior to myectomy, there were no ventricular arrhythmias registered, MWT was 18 mm, peak LVOTG 85 mm Hg, myocardial mass 208 gram, and she had no other diseases capable of producing such hypertrophy. Longitudinal strain analysis showed normal values for global (−19.1%) and septal strain (−22.3%).
A blinded quantification of replacement fibrosis was repeated after 12 weeks. Retest reproducibility, expressed as intraclass correlation, was 0.98.
Echocardiography
All the patients had asymmetrical septal hypertrophy, and 29 patients (91%) had a resting peak LVOTG ≥30 mm Hg. Three (9%) was labile obstructive HCM patients with an exercise-induced gradient ≥50 mm Hg. Global and septal longitudinal and circumferential strain parameters could be assessed in 92% and 78% of the patients, respectively, and the longitudinal and circumferential strain values are shown in table 1.
There were no differences between patients with (n=23) or without (n=9) additional diseases with respect to MWT, peak LVOTG, global or septal longitudinal strain, and global or septal circumferential strain (data not shown).
Interobserver intraclass correlation for longitudinal strain measurements in 10 patients was 0.91. Comparison between longitudinal strain by speckle-tracking echocardiography and by tissue Doppler imaging (n=18) showed excellent correlation with an intraclass correlation of 0.98.
LGE-CMR
LGE was detected in 13/21 patients (62%), affecting 81/357 segments (table 1). There were no differences between patients with (n=13) or without presence of septal-LGE (n=8) with respect to extent of total, interstitial, or replacement fibrosis (table 2).
Comparisons of LGE-CMR, histological and echocardiographic findings in 13 obstructive HCM patients with and 8 patients without septal LGE
Patients with additional diseases (n=13) did not differ from those without (n=8), with respect to presence of global or septal LGE, and there were no differences in the amount of %global or %septal LGE (data not shown).
Histological fibrosis—relations to CMR and echocardiography
No correlations were found between %septal LGE and total (r=0.25, p=0.28), interstitial (r=0.37, p=0.10), or replacement fibrosis (r=−0.03, p=0.90) (n=21). By contrast, septal longitudinal strain correlated with total (r=0.50, p=0.01), and interstitial (r=0.40 p=0.03), but not with replacement fibrosis (r=0.28 p=0.14) (n=30). EF, MWT, global and septal circumferential strain did not correlate with total, interstitial, or replacement fibrosis (data not shown).
Univariable logistic regression analyses showed that only septal longitudinal strain significantly predicted histological fibrosis ≥15% (median value), and in the multivariable analysis, septal strain was an independent predictor of histological fibrosis ≥15% (table 3).
Univariable and multivariable logistic regression analyses for predictors of histological fibrosis ≥15% (median value) in operation specimens from 32 obstructive HCM patients undergoing basal septal myectomy
Ventricular arrhythmias
Eight patients (25%) experienced ventricular arrhythmias, and these patients had lower septal longitudinal strain (−12±4% vs −16±3%, p=0.01) and higher amount of total (34(14, 63)% vs 13(6, 21)%, p=0.03) and interstitial fibrosis (28 (10, 59)% vs 9 (3, 18)%, p=0.04) compared to patients without ventricular arrhythmias (n=24). In the 13 patients with LGE present, no significant differences were demonstrated between patients with (n=4) and without (n=9) ventricular arrhythmias in %global or %septal LGE (3.4 (1.7, 7.6)% vs 2.9 (0.8, 7.7)%, p=0.70 and 9.6 (5.2, 10.3)% vs 4.6 (1.5, 13.0)% p=0.28, respectively). Longitudinal septal strain and extent of interstitial fibrosis predicted ventricular arrhythmias independently of age and gender (table 4). Due to a significant interaction between interstitial fibrosis and longitudinal septal strain (r=0.40, p=0.03), these parameters were not included in the same model.
Univariable and multivariable logistic regression analyses for predictors of ventricular arrhythmias (n=8) in 32 obstructive HCM patients undergoing basal septal myectomy
Discussion
We demonstrate that patients with fibrosis in myectomy specimens have reduced myocardial function. Septal longitudinal strain correlated significantly with septal fibrosis, and tracked with amount of interstitial type of fibrosis, but not with replacement type of fibrosis. LGE by CMR imaging did not correlate with the quantity of fibrosis. A substantial part of the patients with significant fibrosis in their myectomy specimen had no visible septal-LGE by CMR, indicating that visual assessment of septal-LGE is suboptimal.
Until recently, a few autopsy reports have been the basis for the assumption that LGE represents fibrosis in HCM.8 ,12 However, HCM patients included in autopsy studies represent those with advanced or end-stage disease and, thus, the patient population differs from the population in studies of myectomy specimens. Moravsky et al14 recently published an association between extent of septal LGE and extent of total fibrosis from myectomy specimens in HCM patients. By contrast, we did not find a significant correlation between extent of total histological fibrosis and septal LGE. While the extent of septal LGE and the amount of fibrosis were at the same levels, several other factors may explain the different results. The studies included somewhat different populations as patients with CAD were excluded in Moravsky's study, but not in the current one. On the other hand CAD was not identified as an explanatory factor for fibrosis. Moreover, Moravsky et al used two segments (basal and mid-ventricular anteroseptal segments) and we recorded LGE from four segments (basal and mid-ventricular anteroseptal and inferoseptal segments). Our basis for selecting these segments was the findings of CMR performed after the procedure that demonstrated the site of the myectomy. The studies also differed in the use of CMR processing techniques. Current techniques for detection and quantification of LGE include visual inspection, and semiautomatic grey-scale techniques.14 ,27 In the current study, LGE was demonstrated in 23% of the segments, similar to the findings of Saito et al20 which used the 2-SD semiautomatic technique. Compared with visual estimation, the 2-SD grey-scale technique has been demonstrated to overestimate the extent of LGE-related fibrosis.27 In our study, myocardial LGE was demonstrated in 62% of the patients, but 97% had fibrosis in the myectomy specimen, indicating that LGE-CMR does not visualise all the myocardial fibrosis. Whether this is specific for the visual estimate method or is a more general feature of LGE-CMR is unknown. Visual estimation of LGE correlate best with the 6-SD threshold.27 Moravsky et al used 2-, 4-, 5-, 6- and 10-SD, and full-width-at-half-maximum-techniques to assess LGE. The relation between fibrosis and LGE was highly dependent on the grey-scale technique used, but none of the methods discriminated between interstitial and replacement fibrosis. The optimal LGE-CMR method for correct detection of fibrosis in HCM is yet to be determined.28 CMR with T1 measurements estimates interstitial fibrosis as an increased volume of distribution of gadolinium reflecting increased myocardial extracellular volume. T1 measurements might be a useful tool for characterising fibrosis in these patients.29
The prognostic value of LGE for adverse events in the natural history of HCM is well recognised, as is the progression of LGE along with disease progression.8–11 ,13 In the current study, LGE did not predict ventricular arrhythmias, and patients with arrhythmias did not have significantly higher LGE. This may be explained by the limited number of patients with arrhythmic events that had available LGE-CMR. However, longitudinal septal strain in the same patients significantly predicted arrhythmias. Thus, myocardial function assessed by strain was a more robust and powerful tool to assess fibrosis and predict ventricular arrhythmias.
We have shown that longitudinal septal strain was reduced in patients having arrhythmia, while circumferential septal strain did not predict arrhythmias. This indicates that reduced longitudinal function may play a special role in arrhythmogenesis and might be more related to increased levels of disarray in patients with HCM. The presence of disarray is associated with more severe prognosis, and we have recently published that genotype-positive patients have reduced longitudinal myocardial function, and increased risk of arrhythmias compared to genotype-negative patients.21 ,23 HCM patients have increased level of septal fibrosis at the time of myectomy, and interstitial fibrosis constitutes the major part.6 ,7 ,14 ,23 The distinction between replacement and interstitial fibrosis is important as interstitial fibrosis better predicts reduced longitudinal myocardial function and arrhythmias. Whether this is due to a specific quality associated with the type of fibrosis or is merely due to the fact that interstitial fibrosis constitutes the major part of fibrosis remains an open question. Possibly, regions with interstitial fibrosis, where the connective tissue intertwines the myocytes in contrast with areas with replacement fibrosis where the myocytes are replaced by connective tissue, may be more vulnerable for mechanical and electrical disturbances than regions with replacement fibrosis.23
Limitations
This study included a limited number of obstructive HCM patients referred to a tertiary centre. Obstructive HCM patients constitute about 25% of the general HCM population, and our results may not be representative for a general HCM population. While some studies exclude patients with comorbidities, we included patients with additional CAD, hypertension and diabetes mellitus as these patients constitute an important part of the HCM population. Despite the similarities of pathological findings to patients in other HCM studies,7 ,11 ,14 ,30 one might argue that septal fibrosis could originate from CAD and not solely from HCM. However, no differences were observed in patients with and without CAD regarding myocardial function, extent of LGE and amount of fibrosis. Furthermore, septal strain predicted histological fibrosis ≥15% independently of CAD. Hypertrophy in patients with HCM is often asymmetrically distributed. Future studies may include software with the possibility of adjusting ROI to determine if this might further improve strain measurements in these patients.
Conclusions
Reduced septal myocardial function by echocardiographic longitudinal strain was closely related to septal fibrosis in patients with HCM, did specifically relate to interstitial type of fibrosis, and predicted ventricular arrhythmias. Myocardial strain adds valuable prognostic information in HCM patients, and was a more powerful tool than LGE in detecting septal fibrosis and predicting arrhythmias.
Key messages
-
What is already known on this subject
-
Myocardial fibrosis is associated with adverse outcome in patients with hypertrophic cardiomyopathy (HCM). Late gadolinium enhancement (LGE) by cardiac magnetic resonance (CMR) has been the reference standard for non-invasive assessment of fibrosis, but the histological substrate for LGE-related fibrosis in HCM patients is still debated. HCM patients have reduced myocardial function evaluated by strain echocardiography. It has been shown that reduced myocardial function is associated with regions with and without LGE-related fibrosis.
-
What this study adds
-
This study uses a histopathology as a standard to compare the ability of echocardiographic strain and LGE-CMR to detect myocardial fibrosis in myectomised obstructive HCM patients. Echocardiographic longitudinal septal strain correlated significantly with histological fibrosis in myectomy specimens, and tracked with amount of interstitial type of fibrosis, but not with replacement type of fibrosis. In myectomised HCM patients, reduced longitudinal septal strain correlated better with interstitial and total fibrosis in myectomy specimens, and was a more powerful tool in predicting arrhythmias than LGE.
Acknowledgments
We appreciate the help from Maj-Britt Skaale, Department of Cardiology, Oslo University Hospital, Rikshospitalet, for processing rhythm registration data.
References
Footnotes
-
Contributors VMA, KHH, EHS, HS, H-JS, JPA, TE: conception and design, data analysis, interpretation, drafting and final approval; CPD, ORG, KE, SA: conception and design, review and final approval.
-
Funding Parts of the study were sponsored by Inger and John Fredriksen's Heart Foundation which had no involvement in the study design, in the collection, analysis and interpretation of data, in writing the report, or in the decision to submit the paper for publication.
-
Competing interests None.
-
Ethics approval The study complies with the Declaration of Helsinki, and was approved by the Regional Committee for Medical Research Ethics. Written informed consent was obtained from all patients.
-
Provenance and peer review Not commissioned; externally peer reviewed.