Article Text

Abstract
Objective European ST-segment elevation myocardial infarction (STEMI) guidelines recommend prehospital diagnosis to facilitate early reperfusion in patients with STEMI, and they provide recommendations regarding optimal system delay (time from first medical contact (FMC) to the primary percutaneous coronary intervention (PPCI)). There are limited data on achievable system delays in an optimal STEMI system of care using prehospital diagnosis to triage patients with STEMI directly to percutaneous coronary intervention (PCI) centres. We examined the proportion of tentative prehospital STEMI diagnoses established by telemedicine confirmed on hospital arrival, and we determined system delay in patients diagnosed before hospital arrival and triaged directly to the catheterisation laboratory.
Methods Design: Population-based follow-up study. Setting: Central Denmark Region. Participants: 15 992 patients diagnosed using telemedicine.
Results During the study period, a tentative diagnosis of STEMI was established in 1061 patients, of whom 919 were triaged directly to the PCI centre. In 771 (84%) patients, a diagnosis of STEMI was confirmed. Patients transported <10 km had a mean system delay of 82 min; this delay rose to 103 min for patients transported 50–75 km. Data on system delay was achievable in 682 patients in whom 553 (81%) were treated within 120 min of the FMC, and a system delay of <120 min was achievable in 89% of patients living up to 95 km from the PCI centre. Even for patients living <10 km from the PCI centre, only 16 (14%) had a system delay of 60 min or less.
Conclusions The use of telemedicine for prehospital diagnosis and triage of patients directly to the catheter laboratory is feasible and allows 89% of patients living up to 95 km from the invasive centre to be treated with PPCI within 120 min of the emergency medical service call. The study confirms that a recommendation of a system delay <60 min is unachievable if the FMC is the emergency medical call.
- Electrocardiography
- Triage/methods
- Emergency Medical Services
- Coronary angiography
Statistics from Altmetric.com
Introduction
Early reperfusion is crucial in patients with ST-segment elevation myocardial infarction (STEMI).1 Primary percutaneous coronary intervention (PPCI) is the preferred reperfusion strategy.2 ,3 Several initiatives have been suggested to reduce system delay, which is defined as the total delay from the first medical contact (FMC) to PPCI.4 ,5
Prehospital diagnosis using telemedicine combined with field triage of patients directly to the catheterisation laboratory (cath lab) is associated with earlier reperfusion with PPCI. However, some patients suspected of having STEMI triaged for acute coronary angiography have no culprit lesion.
Inappropriate activation of the cath lab is inevitable,6 ,7 but we have little knowledge about the extent and the factors that cause it. This may best be clarified by sampling relevant data from an unselected cohort of patients in whom prehospital diagnosis is performed. In Denmark, we have a unique opportunity to evaluate inappropriate activation of the cath lab, because prehospital diagnoses made using telemedicine are registered in a national telemedicine database and can therefore be compared with subsequent diagnoses established at the hospital.
In Denmark, high-volume PCI centres have been established, and telemedicine for prehospital diagnosis and triage of patients directly to these PCI centres has been implemented whereby local hospitals are bypassed. This is in contrast with many other countries where a large number of low-volume PCI centres have been set up because it is assumed that this facilitates easy access to relevant therapy. There are limited data on the feasibility of using telemedicine for prehospital diagnosis as well as limited data on the associated system delay and acceptable catchment areas for large-volume PCI centres focusing on field triage of patients. Nor has it been established what is the maximum distance from the PCI centre in kilometres to ensure treatment within the 120 min treatment limit of the FMC recommended in clinical guidelines.
It has also been debated what is achievable in terms of system delay in an optimal STEMI system of care prioritising prehospital diagnosis and triage of patients directly to PCI centres.8
The objectives of this study were twofold: (1) to evaluate the proportion of tentative diagnoses of STEMI established by telemedicine that are confirmed on hospital arrival; (2) to determine the association between transport distance from the scene of the event to the PCI centre and system delay among patients field-triaged directly to PPCI.
Methods and data analysis
Study design
The study was a population-based follow-up study. It was approved by the Danish Health and Medicines Authority and the Danish Data Protection Agency. The study did not require approval from The National Committee on Health Research Ethics.
Setting
Aarhus University Hospital in Skejby, Denmark, provides 24 h PPCI service for the 1.2 million inhabitants in the Central Denmark Region. Four hospitals in the region have a 24 h manned telecentre. The physician on call at the telecentre interprets the ECG, interviews the patient and/or ambulance personnel, establishes a tentative diagnosis, and, if STEMI is suspected, recommends that the patient is field-triaged directly to the PCI centre.
Population
The study period was 22 May 2008 to 29 November 2011. The study population comprised patients who were transported by an ambulance or helicopter (implemented in the western part of the region from 1 June 2011), had a prehospital ECG acquired and transmitted to a telecentre, had a tentative diagnosis of STEMI established by telemedicine, and were triaged directly to the cath lab. Patients in whom STEMI or other cardiac-related conditions that required invasive therapy (cardiac arrest, bradycardia, cardiogenic shock) were not suspected were triaged to the local hospital. Data were stored in the Danish National Telemedicine Database. In uncertain cases or for equivocal diagnoses, the attending physician had the possibility to consult the PCI operator or a senior cardiologist on the ward. Baseline characteristics including demographic values and details on coronary angiographies were recorded in the Western Denmark Heart Registry. Patients self-presenting at the PCI centre or the local hospital were excluded.
Patients diagnosed before hospital arrival and triaged directly to the cath lab in whom the PCI operator found signs of STEMI in the ECG and treated a culprit lesion by PPCI were registered as ‘appropriate activation’ and assigned a STEMI diagnosis. Patients with cardiac arrest triaged to PPCI were classified as ‘appropriate activation’ regardless of the angiography or the ECG findings. To determine the final diagnosis and whether the ECG met the criteria for cath lab activation, two senior hospital cardiologists (LF and CJT) reviewed the prehospital ECG and records of patients without a culprit lesion, patients in whom the cath lab procedure was cancelled, and patients with incomplete recordings. Significant ST-segment elevation required ST-segment elevation in the J-point in two or more contiguous ECG leads of ≥0.2 mV for men or ≥0.15 mV for women in V2–3 and/or >0.1 mV in other leads for both genders.9 ,10 Left-bundle branch block with Sgarbossa criteria11 and de Winter ST/T wave complexes12 were acknowledged as STEMI-equivalent signs.
The time of the emergency medical service (EMS) call, the time of EMS arrival on the scene, the time of the EMS departure from the scene, and the time of arrival at the PCI centre were registered in an EMS database. The time of symptom onset, the time of arrival at the cath lab, the time of first catheterisation with a guiding catheter and baseline characteristics were registered in the Western Denmark Heart Registry. The system delay was defined as the time elapsed from the EMS call to the first catheterisation with a guiding catheter. The estimated transport distance was measured using a map service (http://maps.google.com) in which the address of the scene of the event and of the PCI centre were entered. Patients with incomplete EMS data were excluded.
Statistical methods
Statistical analyses were performed using Stata V.12.1. Categorical variables are presented as n (%), and continuous variables as mean (SD). Restricted cubic spline with three knots was performed to evaluate the association between transportation distance and five delay parameters according to distance from the scene of the event to the PCI centre.
Results
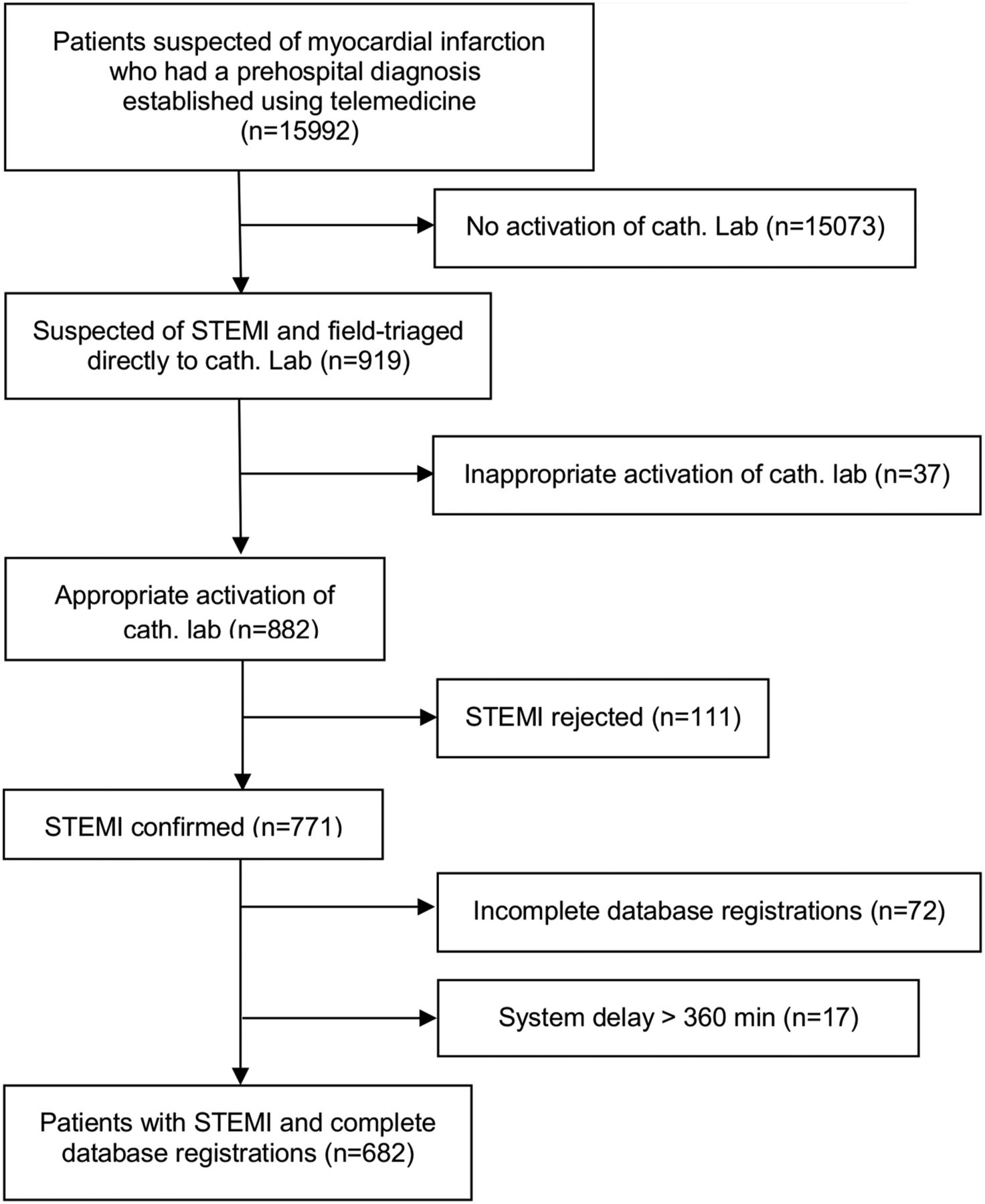
In the study period, 15 992 patients were diagnosed and triaged using telemedicine (figure 1). A tentative STEMI diagnosis was established in 1061 patients, of whom 919 were field-triaged to the cath lab. Of the 919 field-triaged patients, 901 (98%), 16 (1.7%) and 2 (0.3%) were triaged by the telecentre at Aarhus University Hospital in Skejby, Herning Regional Hospital and Viborg Regional Hospital, respectively. The cath lab activations were appropriate in 882 (96%) cases, and the STEMI diagnosis was confirmed in 771 (83.9%) of the cases.

Flowchart of actions with patients suspected of having ST-segment elevation myocardial infarction (STEMI) in the period 22 May 2008 to 29 November 2011 prehospital diagnosed using telemedicine and triaged directly to the catheterisation laboratory (cath lab) at Aarhus University Hospital in Skejby.
The final diagnoses for patients triaged directly to the cath lab are shown in table 1. Early repolarisation (n=27) was seen in the ECG in the majority of the cases in which the cath lab was appropriately activated, and angiography showed no culprit lesion. Inappropriate activation was most often caused by incorrect interpretation of ST-segment elevation in the ECG. In 23 cases (2.5%), the attending physician misjudged the ECG as showing ST-segment elevation and incorrectly activated the cath lab. The mean age of all participants was 64.6 (SD=13.3) years and the majority of the patients were male (table 2). There was no difference in age between patients with STEMI and those with other diagnoses, and no difference in age between patients in cases of appropriate and inappropriate activation (table 2).
Adjudicated diagnosis in patients diagnosed before hospital arrival and triaged directly to primary percutaneous coronary intervention in the period 22 May 2008 to 29 November 2011 (N=919)
Characteristics of patients with ST-segment elevation myocardial infarction (STEMI) as tentative diagnosis using telemedicine and triaged directly to the percutaneous coronary intervention centre in the period 22 May 2008–29 November 2011
In 682 cases, data on transport distance from the scene of the event to the PCI centre were available in the EMS database. The majority of the missing data were on the time and the address of the scene of the event, which made it impossible to calculate the distance to the PCI centre and the system delay, and these were thus excluded. The distance from the scene of the event to the PCI centre was <25 km in 213 (31%) of the cases (table 3). The majority (63%) of patients had to be transported <50 km (n=434), but a minority had to be transported >75 km (n=106). The mean system delay for the total cohort was 97 min (SD=30). A total of 553 patients (81%) were treated with PPCI within 120 min of the EMS call. The maximum distance from the scene of the event to the PCI centre was 160 km, and the longest system delay was 243 min.
Distance from the scene of the event to the percutaneous coronary intervention centre in patients with ST-segment elevation myocardial infarction diagnosed before arrival at hospital and triaged directly to the catheterisation laboratory for reperfusion using PPCI
Figure 2 presents the association between five intervals of delay to reperfusion and the distance from the scene of the event to the PCI centre using restricted cubic spline with three knots. This showed an approximate linearity, and the fit of the model was evaluated using residuals plots. R2, measuring the strength of the association, was 0.3286 for system delay, 0.5295 for EMS call to arrival at the PCI centre, 0.0068 for EMS call to acquisition of the ECG, 0.0024 for EMS call to departure to the scene, and 0.0003 for EMS call to departure from the scene. The response time (time from the EMS call to departure to the scene of the event) and the time from the EMS call to departure from the scene of the event were independent of the distance from the scene of the event to the PCI centre. The time from the EMS call until receiving the ECG at the telecentre rose when the distance to the invasive centre exceeded 100 km. The curves of system delay and EMS call to arrival at the PCI centre were parallel, as expected. The curve representing the association between the distance to the PCI centre and system delay exceeded the 120 min recommended system delay at 95 km. A total of 608 patients (89.1%) lived within 95 km of the PCI centre, and 539 (88.7%) of these were treated within 120 min of the EMS call. Even among patients living <10 km from the PCI centre, only 16 (14%) had a system delay of 60 min or less.

{kind=link}
{kind=link}
Fitted values of five delay parameters according to distance from the scene of the event to the percutaneous coronary intervention (PCI) centre for patients with ST-segment elevation myocardial infarction treated with primary PCI. System delay: delay from the emergency medical service (EMS) call to first catheterisation with a guiding catheter.
Discussion
This study evaluated the use of telemedicine for prehospital diagnosis and field triage of patients with suspected STEMI directly to the cath lab. The three main findings of the present study were: (1) 96% of cath lab activations were judged to be appropriate; (2) the STEMI diagnosis was confirmed in 84% of the cases; (3) 88.7% of patients living up to 95 km from the cath lab could be treated with a healthcare system delay of <120 min. The small number of inappropriate activations of the cath lab and the large number of confirmed STEMI diagnoses show that field triage of patients using telemedicine is feasible.
An acceptable threshold for inappropriate activations has not been defined, but it should obviously not be set at a level that compromises specificity or unduly strains available resources. We found 4% of all cath lab activations to be inappropriate, which would seem to be acceptable. This small percentage can partly be explained by the ease with which the judgement of the PCI operator or the attending cardiologist could be obtained before arrival of the patient at hospital. The attending physician at Aarhus University Hospital in Skejby has 24 h contact with either of these if he or she needs an opinion about a patient. The number of inappropriate activations is too small to determine whether the specificity was compromised. Whether the small number indicates that specificity is compromised requires further study, although the size of the cohort in this study seems sufficient to substantiate an opinion.
The small number of inappropriate activations indicates that the quality of the triage is high even though the decision to activate the cath lab is often made without a previous ECG available or little or no time to observe how changes in ECG and biomarkers evolve. Ongoing studies are currently evaluating the possible benefit of prehospital measurement of troponins and other biomarkers.13
Previously, patients suspected of having STEMI were transported to a local hospital for stabilisation and subsequently transferred to a PCI centre. Telemedicine, field triage and introduction of an anaesthetist as part of a mobile medical service has changed this procedure, and the majority of patients with STEMI are now diagnosed before arrival at hospital and triaged directly to the PCI centre.14 In the case of a long journey (>20–30 min) to the PCI centre, an anaesthetist meets the primary EMS vehicle by rendezvous, initiates relevant therapy, and accompanies the patient to the PCI centre. A few patients field-triaged with STEMI are still transported to a local hospital, but the number has a downward trend.14 In the present study, focus was on delay to reperfusion in an optimal STEMI system of care focusing on prehospital diagnosis and field triage directly to a PCI centre. We therefore excluded those transferred from non-PCI hospitals and those diagnosed before hospital arrival but transported to the local hospital before transfer.
System delay is associated with the distance from the scene of the event to the PCI centre, but it does, however, appear to be higher for patients transported <10 km than for patients transported 11–20 km. This may be because the PCI centre at Aarhus University Hospital in Skejby is located on the outskirts of a city where traffic may influence the system delay even though the distance transported seems short. Patients transported >11 km can bypass the city centre and save some transport time, and system delay may therefore be shorter for these patients. A recently published study15 using data from a prehospital setup that was nearly identical with the one used by us found a median system delay of 173 min in patients living >100 km from a PCI centre. We found a median system delay of 133 min in patients living >100 km from the PCI centre (table 3), which is considerably lower. This difference may be due to geographical differences, but further studies are required to explain this difference. Notably, the system delay for patients living more than 100 km from the PCI centre in our study was comparable to the system delay achieved for patients living 65–100 km from the PCI centre in a previous Danish study,15 which highlights the optimal setup in the present study.
The short time from the EMS call to PPCI indicates that using telemedicine with ECG is very effective. The European Guidelines call for PPCI within 120 min of the FMC if PPCI is to remain superior to fibrinolysis administration,16 and a recent Danish study evaluating the use of a helicopter for transport of patients with STEMI showed that patients living up to 150 km from the invasive centre can be treated within 120 min of the FMC.17 The addition of helicopter transport leaves little room for fibrinolysis in a country such as Denmark with maximum transport distances to a PCI centre of ∼150 km. However, the 2012 European Society of Cardiology (ESC) STEMI Guidelines also recommend fibrinolytic therapy within 30 min of the FMC if PPCI cannot be performed within 60 min of the FMC in patients presenting early and who are at serious risk of a myocardial incident. Only a few patients (4.1%) in our study had a system delay <60 min. Should they have been treated with fibrinolytic therapy at the scene of the event or at the local hospital instead of being transported to the PCI centre for PPCI treatment? As Terkelsen et al recently pointed out,8 the introduction of the 60 min window for PPCI is due to a misinterpretation of the terms ‘PCI-related delay’ and ‘FMC to PPCI’. In fact, the guidelines use publications addressing ‘PCI-related delay’ to give recommendations regarding ‘FMC to PPCI’ delay. ‘PCI-related delay’ is the extra time you may use to perform PPCI instead of administering fibrinolysis and still achieve a benefit from PPCI, whereas ‘FMC to PPCI’ delay is the delay from alarm call to PPCI in regions focusing on prehospital diagnosis and field triage.8 Our study has shown that, even when implementing prehospital diagnosis and field triage, it is impossible to achieve the ESC-recommended system delay of <60 min when the FMC is an EMS call. This does not mean that we should not focus on prehospital diagnosis and field triage to PCI centres. On the contrary, there is evidence that PPCI is superior to fibrinolysis as long as the extra delay used to perform PPCI instead of administering fibrinolysis —that is, the PCI-related delay—is <120 min. It is clear that, for future revisions, the guidelines should be careful not to misinterpret ‘PCI-related delay’ and ‘FMC to PPCI’. Moreover, recommendations on optimal ‘FMC to PCI’ delay should differ according to the diagnostic setup —that is, whether patients are diagnosed before arrival at hospital or whether they self-present at a hospital.
Strengths and limitations
The major strength of our study is the ability to combine prehospital and in-hospital databases to provide a detailed description of the association between the distance from the scene of the event to the PCI centre and system delay in patients treated with PPCI. Even though guidelines provide recommendations on optimal system delay, only a few population-based studies have documented achievable delays from the FMC to reperfusion in daily clinical practice.
As in any study, there is a risk of selection bias, but there is no reason to believe that patients were selected according to distance to the PCI centre, and, moreover, data were entered prospectively into the database. Data on the sensitivity of a prehospital diagnosis of STEMI cannot be derived from the present paper, but previous studies from the Central Denmark Region have documented that ∼80% of patients with STEMI are now identified in the prehospital phase.18 The present paper only evaluated the diagnostic performance of a prehospital diagnosis established using telemedicine. It would be of interest to compare diagnostic accuracies by telemedicine with diagnostic accuracies achieved when the prehospital diagnoses are established by paramedics or ambulance physicians.
The purpose of this study was to describe the association between elements in the system delay in relation to the distance from the scene of the event to the PCI centre. In future studies it may be relevant to adjust for confounders and consider interactions.
Conclusion
The use of telemedicine for prehospital diagnosis and triage of patients directly to the cath lab is feasible and allows 89% of patients living up to 95 km from the invasive centre to be treated with PPCI within 120 min of the EMS call. The study confirms that a recommendation of a system delay <60 min is not achievable if the FMC is the EMS call.
Key messages
What is already known about this subject?
-
Prehospital diagnosis using telemedicine combined with field triage of patients suspected of having ST-segment elevation myocardial infarction (STEMI) directly to the catheterisation laboratory (cath lab) has been proved to reduce system delay, defined as the total delay from the first medical contact to primary percutaneous coronary intervention (PPCI).
-
Little is known about the proportion of prehospital STEMI diagnoses confirmed on hospital arrival, and an acceptable cath lab activation threshold has not yet been defined. Furthermore, there are limited data on achievable system delays according to distance from the scene of the event to the percutaneous coronary intervention (PCI) centre.
How may this impact on clinical practice?
-
. The study promotes the increased use of prehospital diagnosis and triage of patients directly to PCI centres thereby bypassing local hospitals in the case of suspected STEMI.
What does this study add?
-
. This is one of the first studies to address optimal healthcare system delay in patients diagnosed before arrival at hospital and field-triaged directly to a PCI centre. Furthermore, it is the first report describing a detailed association between various components of system delay and transport distance in these patients. The study confirms the challenges in achieving system delays of <60 min even in areas with an optimal STEMI system using prehospital diagnosis where the first medical contact is the emergency medical service call.
References
Footnotes
-
Contributors MBR and CJT made the drafts of the manuscript, data analysis and performed the statistical analysis. All authors participated in data acquisition and critical revision of the manuscript.
-
Funding The National Telemedicine Database was supported by a grant from the Tryg Foundation (No 7822-07). The study was supported by the Riisfort Foundation.
-
Competing interests LF has received support for research, education and/or consultant fees from Astra Zeneca, Bayer, BMS, Boehringer Ingelheim, GSK, MSD, Pfizer, Roche, Sanofi, Servier, St Jude Medical and Takeda. CS has received lecture fees and support for research from Roche Diagnostics, Germany.
-
Ethics approval Danish Health and Medicines Authority and the Danish Data Protection Agency.
-
Provenance and peer review Not commissioned; externally peer reviewed.