Article Text

Abstract
Objective To estimate the risk of atrial fibrillation (AF) and stroke and the impact of closure in patients with atrial septal defect (ASD) compared with a general population cohort.
Methods All adult Danish patients (>18 years) diagnosed with ASD from 1977 to 2009 (N=1168) were identified through population-based registries. Using Cox regression, we compared ASD patients’ risk of AF and stroke with an age-matched and gender-matched comparison cohort. We computed prevalence proportions of anticoagulation and antiarrhythmic medicine use before and after closure and described stroke-related mortality.
Results Median follow-up was 9.6 years (range 1–33 years). Patients with ASD had a higher risk of first-time AF (adjusted HR 8.2; 95% CI 6.6 to 10.2) after closure than the comparison cohort, but with no difference between transcatheter and surgical closure (HR 1.5, 95% CI 0.6 to 3.5). Patients without prevalent AF had a 10-year cumulative incidence of AF of 11% (95% CI 9% to 14%) after closure compared with 2% (95% CI 1.8% to 2.5%) in the comparison cohort. Patients with ASD with prevalent AF continued to use anticoagulation medicine after closure/diagnosis. Patients with ASD had increased risk of stroke without closure (adjusted HR 2.6; 95% CI 1.4 to 3.0) and with closure (adjusted HR 2.0; 95% CI 1.4 to 2.7). Risk of stroke after closure was related to AF (HR adjusted for AF 1.3; 95% CI 0.9 to 1.9).
Conclusions Patients with ASD had a higher risk of first-time AF after closure than the comparison cohort. There was no effect of closure on the use of AF-related medicine in patients with prevalent AF.
- CONGENITAL HEART DISEASE
Statistics from Altmetric.com
Background
Atrial septal defect (ASD) is a common congenital heart disease often diagnosed in adulthood.1 The inter-atrial shunt gives rise to a volume overload of the right heart, resulting in dilatation and stretching of the myocardial fibres. Atrial interstitial fibrosis and electrophysiological remodelling may develop over time, causing atrial fibrillation (AF) and other arrhythmias.2
The AF incidence increases with age and is found in 9% of elderly above 80 years without ASD.3 AF in patients with ASD is rarely seen before the age of 40,4 but above 60 years, the incidence is as high as 50%.5 AF is associated with a twofold increase in mortality6 and, hence, is both very common and of major clinical importance. AF is a risk factor for stroke,1 ,7 accounting for 19–57% of late deaths in patients with ASD.1 ,5
While most studies agree that the closure of an ASD in adults is beneficial concerning subjective symptoms and regression of right heart dilatation,5 ,8–10 there is no consensus whether the closure of a defect has any effect on pre-existing AF or prevention of new-onset AF.11–15 It is unclear whether the regression of right atrial dilatation normalises the conductance disturbances in the atrium. Vecht et al2 suggest a beneficial effect of the closure on pre-existing AF on short-term (30 days) and medium-term follow-up (up to 5 years) in a review of the existing literature.2 It is unknown whether a small and haemodynamically insignificant ASD carries a higher risk of AF and stroke than the general population. We estimated the risk of new-onset AF following ASD closure (excluding patent foramen ovale (PFO)) compared with a general population cohort. In patients with prevalent AF at closure, we accounted for the use of antiarrhythmic and anticoagulation drugs before and after the closure of their defect as an indication of conversion to sinus rhythm. Finally, we investigated the incidence of stroke in patients with and without defect closure compared with a general population comparison cohort. Stroke was included in this study because stroke, either related to AF or to paradoxical embolism, might be an important cause of death in patients with ASD.
Materials and methods
Study cohort and design
This nationwide cohort, based on national public registries in Denmark, has previously been used in the analysis of risk of pneumonia in patients with ASD.16 The predominantly unified Danish healthcare system is publically funded. Data from hospitals are gathered in public registries linked with a unique personal identification number assigned to all inhabitants since 1968. Information on date of birth, immigration and/or death is identified in the Danish Civil Registration System.17
We used the Danish National Patient Registry (DNPR), established in 1977, to identify all patients born before 1993 and registered with an ASD (see online supplementary appendix 1) until 2009. Diagnoses given before 1977 were included. DNPR contains information on all hospital admissions in Denmark, dates of admissions and discharge, surgical procedures and discharge diagnoses according to the International Classification of Disease (ICD).18 The ICD 8th edition (ICD-8) was used until 1993 after which the 10th version was used. Only patients aged ≥18 at the time of diagnosis were included in the study, and follow-up was continued until 1 January 2011. Patients with concomitant congenital heart disease were excluded, except for those with unspecified congenital heart disease or patent ductus arteriosus (see online supplementary appendix 1).
All hospital records, identified by the identification number through DNPR, were reviewed by two reviewers, and a paediatric cardiologist was consulted in case of discrepancy. Only patients with a confirmed ASD were included, and a defect described as a persistent foramen ovale was excluded.16
As a comparison cohort, for every patient with ASD, 10 persons from the general population were matched on gender and birth year using the Danish Civil Registration System.
Clinical outcome
All hospital admissions or outpatient contacts due to arrhythmia since 1977 and up to 1 January 2011 were identified. Arrhythmia within 30 days after ASD closure was ignored.19 ,20 Outcomes included atrial flutter and AF of paroxysmal, persistent and permanent type (see online supplementary appendix 1). AF was analysed as one common group due to lack of differentiation of AF subtypes in ICD-8.
Anticoagulation use outside the hospitals was identified in the Danish National Prescription Registry containing data on redeemed prescriptions from all Danish pharmacies (see online supplementary appendix 2).21
We used redeemed prescriptions for anticoagulation and antiarrhythmic medicine as an indicator of AF treated outside the hospitals. Both types of medicine were not specific for AF; therefore, patients with a mechanical heart valve or deep venous thrombosis were excluded in these analyses. Patients with stroke are not routinely treated with anticoagulation medicine unless AF is present; therefore, they were not excluded. Stroke was identified in DNPR in the same time period. Outcomes included both stroke and transitory ischaemic attacks, but not cerebral haemorrhages.
Diabetes, pulmonary heart disease (pulmonary arterial hypertension, cor pulmonale, thromboembolic lung disease) and hypertension were identified in DNPR before or at the time of diagnosis using ICD codes (see online supplementary appendix 1) and described as baseline characteristics. These diseases may be related to ASD and play a role in either the incidence of AF or risk of hospitalisation due to arrhythmia.22–24
Statistical analysis
Follow-up of patients with ASD and the comparison cohort started on the date of diagnosis or closure (index date for comparison cohort members). Follow-up continued until first diagnosis with AF, death, emigration or the end of follow-up (1 January 2011), whichever came first. In analyses specific to patients with unclosed ASD, patients were censored at ASD closure.
First, we used Fine and Gray's25 competing risk regression analysis to compute 10-year and 20-year cumulative incidences (CI) of AF and stroke with time from closure or diagnosis as an underlying time scale and death as a competing risk.
Second, we used the Cox proportional hazards regression to compute HRs of time to first AF among patients with ASD beginning 30 days after closure, and compared them with the general population cohort, using age as an underlying time scale. Long-term effects of closure were analysed separately on patients without AF before closure starting at 5 years after closure. Patients were stratified by age group at closure and were adjusted for gender and hypertension. Separate analyses stratified by method of closure were performed. We graphically verified the assumption of proportional hazards with log minus log plots.
Third, the prevalence proportions of anticoagulation medicine and/or antiarrhythmic medicine use at 1 year intervals, starting at 5 years before closure or diagnosis and ending at 5 years after, were assessed and graphically illustrated. This analysis was performed on patients without closure, patients with prevalent AF before closure and patients with neither AF nor anticoagulation use before closure. Only patients diagnosed after year 2000 were included in these analyses as the Danish National Prescription Registry was established in 1995.
Fourth, the relative risk of stroke was analysed by Cox regression analysis with HRs of stroke after closure and after diagnosis (for those without closure) compared with the general population cohort.
Analyses were performed using Stata V.13 (StataCorp LP, Texas, USA).
Results
The inclusion criteria were met by 1168 patients diagnosed in one of 80 Danish hospitals since 1977 (inclusion of patients has previously been described).16 The majority of patients (74%) were diagnosed in one of the four Danish university hospitals. The median follow-up time was 9.6 years (range 1–33). Median follow-up was longer for patients with surgical closure (16.8 years) than those with transcatheter closure (5.2 years). The mean age at the time of diagnosis was 47.7 years (surgical patients: 42.6; transcatheter patients: 49.3 years) (figure 1). The majority (n=1078) had a secundum defect, 51 had a sinus venosus defect and 38 had a primum defect. Transcatheter closures (n=300) were all secundum types. Baseline characteristics are shown in table 1.
Baseline characteristics of patients with ASD with and without closure and the general comparison cohort.

Proportion of atrial septal defect closures, the distribution of transcatheter and surgical approaches and the mean age at time of closure.
Atrial fibrillation
The majority (89%) of patients with ASD with prevalent AF and 60% of those with new-onset AF after closure were above 40 years old at time of closure (table 2). No patients below the age of 25 (n=109) had AF before closure, but after closure, 23 (21%) in this age group developed AF during follow-up and the mean age at the time of first AF for these patients was 49.7±3.0 years. Of those patients, three had flutter and only two were closed by transcatheter approach. The mean age at closure for patients with no prevalent AF was 42.4 (95% CI 41.3 to 43.6), while it was 57.1 (95% CI 55.0 to 59.2) in patients with AF before closure. Of the patients with closure before the age of 40, only 14 (4%) had prevalent AF before closure and 92 (27%) had AF at end of follow-up. In patients >40 years at time of closure, 100 (19%) had prevalent AF before closure and 261 (50%) had AF at end of follow-up.
Number of patients with ASD with AF or stroke: the unclosed group consists of patients who did not undergo closure at any time during follow-up.
When postoperative AF within the first 30 days after closure was excluded, there was no difference between risk of first-time AF before compared with after closure (HR 0.93; 95% CI 0.68 to 1.26).
The risk of AF was not different for patients undergoing transcatheter treatment (HR 1.5; 95% CI 0.6 to 3.5) compared with those with surgical closure after the two first weeks after closure. There was, however, a larger share of flutter in the surgical group (12% of arrhythmias) compared with the transcatheter group (2% of arrhythmias).
Use of anticoagulation and antiarrhythmic medicine
No prevalent AF
The proportion of patients in anticoagulation treatment increased prior to closure compared with the control group. Approximately 10% of the patients with ASD without AF prior to closure were anticoagulated 5 years after closure (see online supplementary figure S1), and none of them had a previous stroke.
Antiarrhythmic medicine was used by only <2% before closure (see online supplementary figure S2). After 4–5 years, the proportion of patients using medicine was about the same as the controls due to a rise in drug use in the control group.
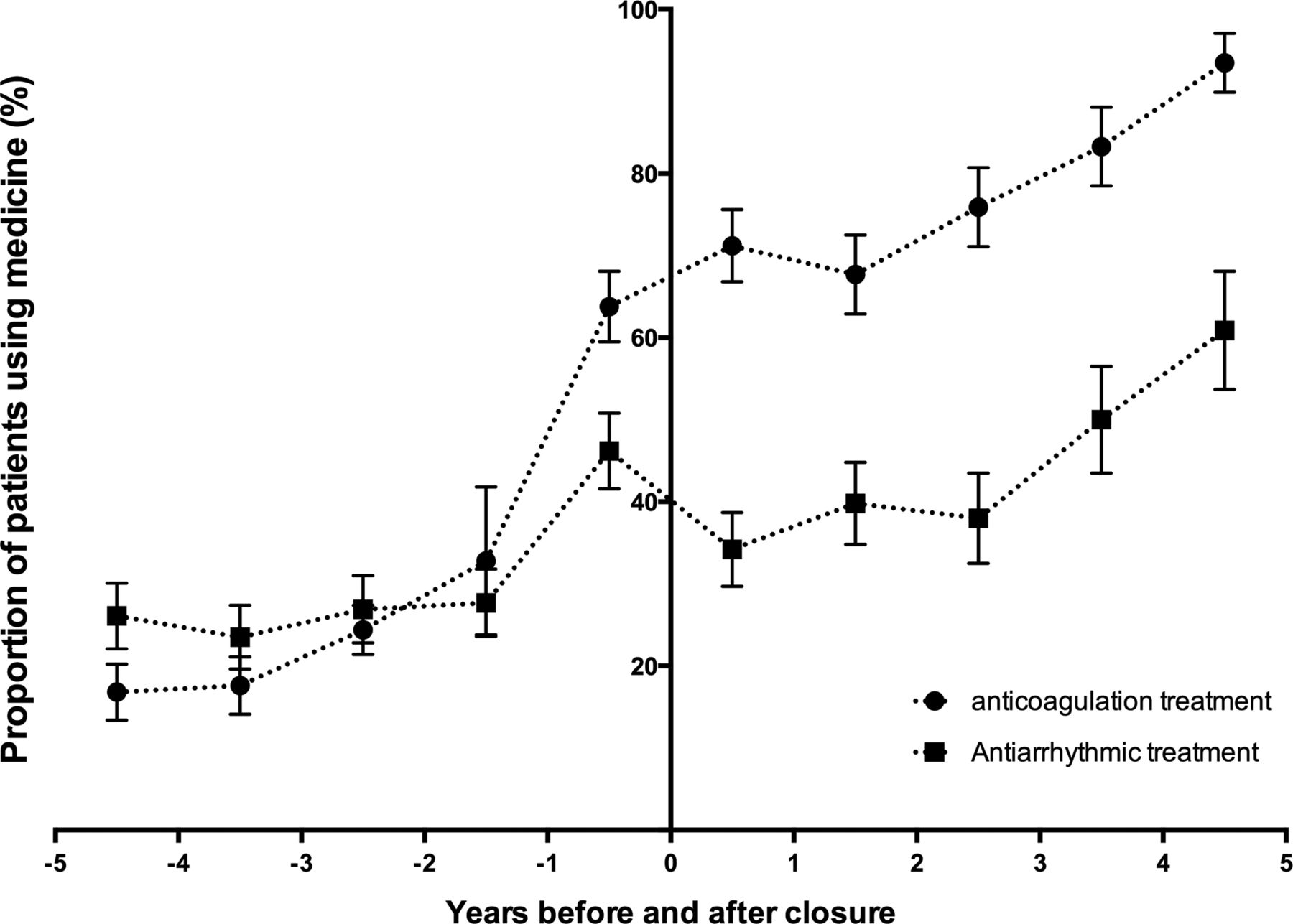
Prevalent AF before closure
The proportion of patients using anticoagulation and antiarrhythmic medicine increased before closure and continued to increase after closure (figure 2). Five years after closure, 93% were treated with anticoagulation medicine, and almost 60% were treated with antiarrhythmic medicine.

{kind=link}
{kind=link}
Proportion of patients with atrial septal defect with closure and prevalent atrial fibrillation using anticoagulation medicine and antiarrhythmic medicine per 100 patient-years from 5 years before closure to 5 years after closure.
Stroke
The risk of stroke was not higher without closure than with closure (tables 3 and 4). There was no difference in risk of stroke between those with closure before the age of 40 (adjusted HR 2.0; 95% CI 0.9 to 4.4) and after 40 (adjusted HR 1.2; 95% CI 0.8 to 1.8). Neither was there any difference in risk of stroke when comparing those who had transcatheter treatment with those with surgical closure (HR 1.2; 95% CI 0.5 to 2.5). The age at time of first stroke was, however, higher for those with surgical closure (mean 57.7±1.8) compared with those who had transcatheter closure (mean 46.8±1.5).
Incidence rates (per 1000 patient-years) and cumulative incidences of AF and stroke 10 and 20 years after diagnosis for those with no closure and after closure for those with closed defects.
Adjusted HR for AF and stroke in patients with ASD with and without closure and the comparison cohort.
Stroke-related mortality
Eight patients with ASD died within 30 days after the stroke diagnosis (0.7% of patients with ASD) compared with 27 patients (0.2%) in the comparison cohort; 1-year mortality following stroke was 7.8% and 16.8%, respectively. Mean age for first stroke in patients with ASD was 55.2 years (95% CI 53.0 to 57.5) and 68.2 years (95% CI 67.2 to 69.2) in the comparison cohort. Death within 30 days of stroke accounted for 3% of the late deaths in the ASD group and 1.5% in the control group during follow-up.
Discussion
In this nationwide cohort study, patients with ASD with prevalent AF did not normalise the use of anticoagulation or antiarrhythmic medicine after closure, and there was a persistent tendency for an increased number of patients using AF-related medication for those without closure. Patients with ASD had an increased risk of developing first-time AF and using anticoagulation drugs after closure compared with the general population cohort. The risk of stroke was higher for patients with ASD both before and after closure compared with the general population cohort. The results indicate that the increased stroke risk after closure was mediated by AF.
In contrast to our findings, Giardini et al11 did not find an increased risk of AF after closure, which was, however, found by Attie,26 who found 8% new-onset AF during follow-up (median 7.3 years), and Gatzoulis et al,4 who found new-onset AF in 7.4% of patients above the age of 40 (mean follow-up of 3.8 years) after closure. Thus, the incidence in a long follow-up period of 20 years remains substantially greater than that in the background population. We do not know, however, whether the risk would have been even higher if closure was not performed.
Changes in surgical techniques during the years of closure and implementation of transcatheter device closure might have had an impact on risk of arrhythmia. We have not found any long-term difference in risk of arrhythmia between patients with transcatheter and surgical closure. There has, however, been an increase in mean age at time of closure during the study period that could result in a higher risk of arrhythmia in patients during the recent decades.
In our study, AF-related medicine did not diminish after closure, and in agreement with Wi et al,13 we found no indication that closure cured prevalent AF. In a review, Vecht et al2 concluded that ASD closure decreases the development of AF within the first five years. After 5 years, the effect tailored off,2 which is in concordance with our study. Berger et al12 found that patients were likely to convert to sinus rhythm after closure if they had preoperative flutter but not if they had fibrillation, and Silversides et al27 found no conversion from preoperative AF to sinus rhythm. In our study, the majority of the arrhythmias were AF (table 2), supporting the observation that use of AF-related medicine remained high after closure. The use of anticoagulation medicine was much higher in patients with AF prior to closure than for those without AF prior to closure, supporting the fact that AF prior to closure increases the risk of AF after closure.27
Murphy et al1 found that closure before the age of 25 years protected against development of AF later in life. In our study, 21% of the patients with ASD, who had closure before the age of 25, developed AF after closure. Thus, changes in the conductance pathways and interstitial fibrosis could be irreversible much earlier than anticipated. Closure in childhood and young adulthood might possibly be protective against future arrhythmias; however, further studies are necessary to confirm these speculations.
Only 28% of the patients with ASD with a stroke prior to closure had known AF. This likely reflects the potential role of paradoxical embolism in the pathology of stroke in patients with ASD. In contrast, AF was seen in the majority (77%) of the patients with ASD with stroke after closure. This is similar to other studies demonstrating that AF is found in 75–83%4 ,12 of patients with ASD with stroke. The approximation of HR towards 1 when adjusted for AF indicated that the stroke risk was normalised in patients with no AF when ASD was closed, which was not the case for patients who continued to have an open passage between the atria.
In 1990, Murphy et al1 found that 22% of late deaths in patients with ASD were caused by stroke. In our study, only 3% of late deaths were within 30 days of stroke. The generally improved intensive care facilities and new treatment strategies in patients with stroke after the study by Murphy et al could have had a high impact on survival after stroke.
Mortality after stroke was higher in the comparison cohort than in the patients with ASD. The age at the time of stroke diagnosis was much younger in the patients with ASD than in those without ASD, and age-related risk factors likely contributed to the observed higher mortality in the comparison cohort. The mortality related to stroke was lower in this study compared with other studies investigating mortality and stroke.28 ,29 In this study, we included trans-ischaemic attacks and stroke. We excluded cerebral haemorrhages known to have higher mortality29 and a potential link to high doses of anticoagulation treatment.
This registry-based study is the largest ASD study with the longest follow-up to date. The use of the unique identification number permits identification of hospital records for several past decades. Classification of dates and diagnoses was re-examined to minimise error and all hospital records were validated for correct diagnosis, status and date of closure,16 which also enabled exclusion of patients with PFO. The following limitations should be considered when interpreting the results. Most patients with unclosed ASDs are asymptomatic, and the diagnosis is often given in relation to other hospital admittances. All adult patients with an ASD diagnosis in Denmark were included, but we can only speculate about the number of undiagnosed ASDs in the population. Patients in this study, especially those with unclosed ASDs, may therefore represent a subgroup with more baseline comorbidities and higher incidences of AF and stroke than the entire population with ASDs. In general, patients with unclosed ASDs likely have smaller defects and less RV strain than those in the group with closed defects. The AF diagnosis has previously been validated with a positive predictive value of 92.6% (95% CI 88.8% to 95.2%),30 and possible misclassifications of the stroke diagnosis are believed to be independent of the ASD diagnosis; therefore, this possibly led us to underestimate the reported associations. The use of medicine does not confirm an actual AF diagnosis and can only be used as an indicator of arrhythmia. Neither confirmation of a continued AF diagnosis or sinus rhythm nor documentation of a change in the nature of the arrhythmia (ie, from paroxysmal to permanent) was possible in this study.
Adults with ASD continue to carry an increased risk of AF despite closure of their defect. Further studies regarding adult patients with small and haemodynamically insignificant ASDs are warranted, and a second opinion after 5–10 years after diagnosis would be recommended.
Key messages
-
What is already known on this subject?
-
There is a link between atrial septal defect (ASD) and the risk of developing atrial fibrillation, and a large part of the patients with ASD develop atrial fibrillation with time. Closure of the defect could minimise the risk of development of atrial fibrillation, but this has not been investigated sufficiently. The risk of stroke in patients with ASD has only been described briefly previously.
What might this study add?
-
This study (n=1168) found that patients with ASD have an increased risk of atrial fibrillation (HR 6.7; 95% CI 5.1 to 8.7) compared with a comparison cohort after closure. In patients with closure before the age of 25, atrial fibrillation developed in 21% during follow-up. The increased risk of stroke after closure was only related to atrial fibrillation.
How might this impact on clinical practice?
-
Follow-up and regular medical exams are often scares in patients with ASD with no atrial fibrillation. A more thorough follow-up programme in these patients could possibly detect arrhythmias and any deterioration at a much earlier time. This also applies to those not offered closure.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online appendix
- Data supplement 2 - Online figure
Footnotes
-
Contributors All authors designed the study. CN, JEN-K and VEH carried out the literature search. CN and MSO obtained and analysed data. CN drafted the manuscript. All authors critically reviewed the manuscript, contributed to its revision and approved the final version submitted.
-
Funding This work was supported by Aarhus University and the Central Denmark Region.
-
Competing interests None.
-
Ethics approval Danish Data Protection Agency (j.nr. 2010-41-4649) and the National Board of Health (j.nr. 7-604-04-2/193/KWH).
-
Provenance and peer review Not commissioned; externally peer reviewed.