Article Text

Abstract
Objective Minimal data are available regarding the long-term mortality risk of subclinical atherosclerosis using coronary artery calcium (CAC) scoring among patients with a family history (FH) of coronary artery disease (CAD). The aim of the present analysis was to assess the prognostic utility of CAC scoring among cohorts of young and older patients with and without a FH of CAD.
Methods A total of 9715 consecutive asymptomatic patients, free of known CAD, underwent CAC scoring for cardiovascular risk assessment. The primary end point was all-cause mortality, with a median follow-up of 14.6 years. Unadjusted and risk-factor adjusted Cox proportional hazard modelling was employed. We calculated the area under the curve (AUC) from receiver operating characteristics analysis.
Results 15-year all-cause mortality rates ranged from 4.7% to 25.0% for FH patients and from 5.0% to 38.0% for non-FH patients with CAC scores of 0 to >400 (p<0.0001). Effect modification by age altered the mortality risk of CAC among FH patients. For patients aged >60 years with FH of CAD, there was a significant improvement in the AUC with CAC over CAD risk factors (AUC: 0.539 vs 0.725, p<0.001). No such improvement was observed in FH patients aged <60 years (AUC: 0.636 vs 0.626, p=0.67).
Conclusion CAC effectively stratified mortality risk of patients with and without FH of CAD. However, for younger and lower-risk FH cohorts, CAC screening did not provide additive prognostic information beyond that of the traditional cardiac risk factors.
Statistics from Altmetric.com
Introduction
Controversy exists as to the effectiveness of screening using measures of subclinical atherosclerosis among asymptomatic, apparently healthy individuals.1 In selected cohorts, observational evidence supports effective risk stratification among patient and population cohorts.2–4 However, a family history (FH) of premature coronary artery disease (CAD) is often not examined separately or included in global risk scores; as such its prognostic significance in long-term risk is often underappreciated.3 ,5
Given the often younger age of FH patients, the ability to understand the long-term outcome risk following index screening is of importance and may serve to guide screening strategies based on a threshold age for mortality risk. Critically important to the estimation of risk in this largely younger FH cohort is whether there is value in routinely screening cohorts of varying ages. Accordingly, the primary aim of this report was to examine the long-term prognostic significance of coronary artery calcium (CAC) scoring among young and older patients with and without a FH of CAD.
Methods
Eligibility criteria
A consecutive series of 9715 asymptomatic patients referred for CAD screening were prospectively enrolled in this single-site registry. The enrolment and follow-up procedures were approved by the institutional review board. A subset of patients included in this series was previously reported.6 ,7
Cardiac risk factor and CAC data
A detailed cardiac risk factor history was ascertained at the time of testing by experienced staff and supervised by a cardiologist. Details of data collection were previously described.6 In brief, a patient was classified as having a FH of CAD if a primary relative had been diagnosed with CAD prior to the age of 65 years (in a female relative) or before the age of 55 years (in a male relative). All patients underwent CAC imaging using either electron beam tomography or multislice CT.6 ,8–11 CAC scores were subset as 0, 1–10, 11–99, 100–399 and ≥400.
Follow-up methods
Median length (IQR) of follow-up was 14.6 years (12.9–16.8 years) (n=936 deaths). No patients were lost to follow-up.
Statistical analysis
The frequencies of cardiac risk factors and CAC score subsets were compared among patients with and without a FH of CAD using a likelihood ratio χ2 statistic. Framingham risk score (FRS) and CAC score were analysed as categorical variables using established clinical cut-points, in accordance with previous research and current guidelines.2 ,6 ,7 ,12 Comparisons of continuous measures with the FH variable were performed using t test.
The primary end point was time to death from all-causes. Univariable and multivariable Cox proportional hazard models were used to estimate the relationship and independent contribution of FH, FRS and CAC measurements to the risk associated with cardiac risk factors. From the Cox model, the HRs and 95% CI were calculated. A multivariable model included risk factor covariates and the FRS. Separate Cox models were developed for patients with and without a FH of CAD, including covariates (as stated above). The proportional hazards assumption was evaluated by assessing the constancy of the parallel plotted lines in the log-log graph. A first-order test for interaction of FH by CAC scores was performed.
Results
Prevalence of CAD risk factors and CAC subsets by FH status
Patients with a FH of CAD were generally younger, more often women, and with a greater prevalence of CAD risk factors. FH patients more often had lower risk CAC scores when compared with non-FH patients (p=0.031) (table 1).
Frequency of CAD risk factors in patients with and without a FH of CAD
Figure 1 plots the prevalence of CAC across age deciles of patients with and without a FH of CAD. For FH and non-FH patients, there was an increasing prevalence of more extensive CAC with advancing age. When comparing FH with non-FH patients, there was a similar prevalence of CAC scores from 0 to 10. By comparison, CAC scores >10 were less prevalent in the largely younger FH patients.
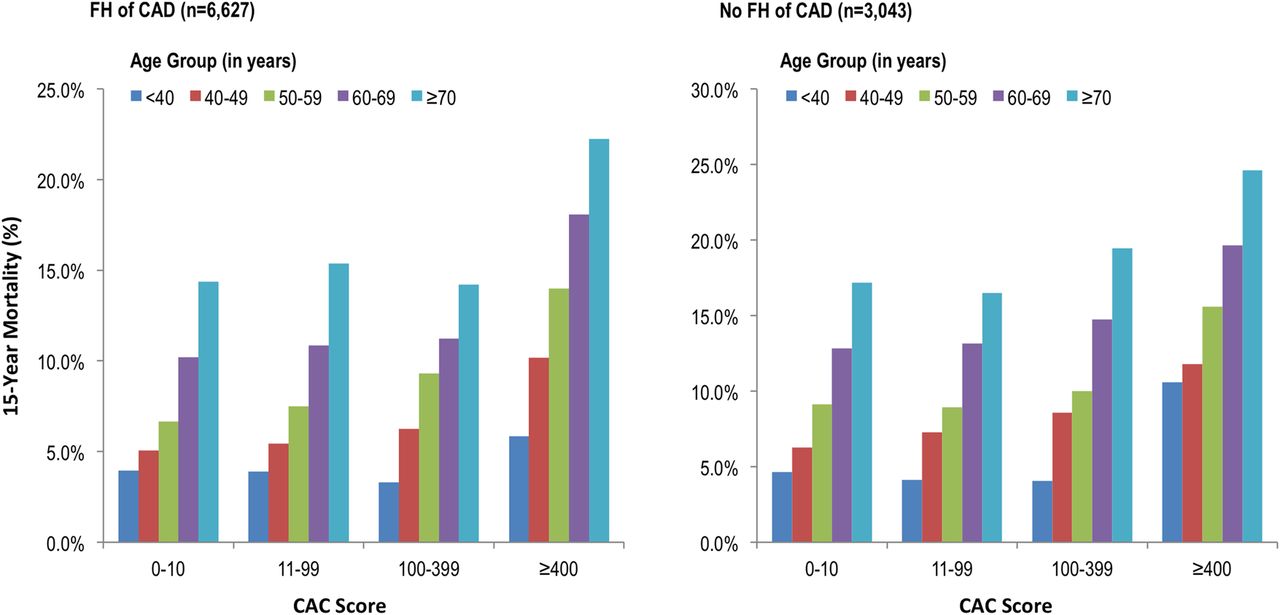
Adjusted 15-year mortality by CAC score and age group among patients with and without a family history of CAD is shown. There is a three-way interaction of the adjusted mortality rates by age×CAC×FH (p=0.033). *Adjusted (or predicted) mortality rates were derived from a multivariable Cox model that included age, CAC and other cardiac risk factor data. CAC, coronary artery calcium; CAD, coronary artery disease; FH, family history.
15-Year mortality by FH and CAC
Overall 15-year mortality was 9.0%. For FH patients, risk-factor adjusted survival ranged from 96% to 82% for CAC scores from 0–10 to ≥400 (p<0.0001) (figure 2). For non-FH patients, adjusted survival ranged from 95% to 79% for CAC scores from 0–10 to ≥400 (p<0.0001). Unadjusted and risk factor-adjusted mortality was significantly lower for FH patients (adjusted mortality 7.0%) than non-FH patients (9.2%). In adjusted models, FH patients had a HR for mortality of 0.77 (95% CI 0.67 to 0.88, p<0.0001).

{kind=link}
{kind=link}
Cumulative, long-term survival in patients with and without a family history of CAD by CAC score results is shown. Higher CAC scores are correlated with lower risk-factor adjusted cumulative survival in FH and non-FH patients (p<0.0001 for both groups). CAC, coronary artery calcium; CAD, coronary artery disease, FH, family history.
In separate Cox models, CAC scoring was highly predictive of 15-year mortality for patients with and without a FH of CAD (table 2, p<0.0001). In FH patients, the HR for death ranged from 1.6 to 3.5 for CAC scores of 1–10 to ≥400 (p<0.0001). For non-FH patients, the HR for death ranged from 1.6 to 6.3 for CAC scores of 1–10 to ≥400 (p<0.0001). A CAC score of 1–10 was predictive of death for FH patients (p=0.004) but not for patients without a FH of CAD (p=0.067).
Cox model estimating 15-year mortality for patients with and without a FH of CAD
In a subset analysis of FH patients, table 3 reports an interaction of age by CAC (p=0.002), suggesting an 8% increased mortality risk per category of CAC with increasing age (by decile). No interaction was identified for non-FH patients (p=0.624). Figure 2 plots the 15-year (risk factor-adjusted) mortality rates by age deciles and CAC score strata for FH and non-FH patients. This analysis revealed a significant interaction between FH and non-FH patients with regard to the adjusted mortality across CAC and age strata of patients (p=0.033).
Cox proportional hazards model estimating 15-year mortality examining a first-order interaction of age and CAC among 6672 patients with a family history (FH) of CAD*
Mortality classification with CAC
Table 4 examines the impact of age <60 and ≥60 years using receiver operating characteristics (ROC) curve analysis. For FH patients, there was no improvement in the area under the curve (AUC) for CAC when compared with the FRS in classifying mortality (p=0.674). By comparison, for FH patients aged ≥60 years and for non-FH patients, CAC significantly improved the AUC for CAC when compared with the FRS (p<0.01).
Receiver operating characteristics (ROC) curve analysis among younger (<60 years) and older (≥60 years) patients with and without a FH of CAD evaluating death classification based on the Framingham risk score (FRS) and CAC score
Discussion
Patients with a FH of CAD often seek guidance as to their need for CAD screening and do so at a younger age. In our observational cohort, FH patients were generally younger with a lower 15-year mortality (p<0.0001), similar to that reported in other international cohorts.13 Despite the younger age of FH patients, effective risk stratification was observed with low-risk to high-risk CAC scores with 15-year survival ranging from 96% to 82%. We further explored the potential for an age threshold whereby screening of FH patients was not associated with an improvement in risk reclassification. Our analyses revealed that CAC was not additive to CAD risk factors for the risk reclassification of mortality in FH patients <60 years of age. This likely represents the earlier referral and, perhaps, unselected nature of testing among FH patients.
Although there has been a traditionally low rate of CAD screening in individuals with a FH of CAD, as reported in the European Action on Secondary Prevention by Intervention to Reduce Events family survey,14 more recent data such as ours suggest that clinical practice may now be more all-inclusive as to their screening practices. This may reflect the state of the literature, which routinely identifies a higher risk of subclinical atherosclerosis in those with a FH of CAD.15 ,16 The literature is replete with reports noting that CAD risk associated with FH is often elevated by as much as twofold and independent of traditional cardiac risk factors.15 ,17 The available literature also supports that FH is often of borderline significance18–21 or not statistically significant in lower risk cohorts.18 ,22 In a recent report from the Glasgow Blood Pressure Clinic, the unadjusted, all-cause mortality risk of FH was 0.74 (95% CI 0.67 to 0.81); similar to the findings in our patient cohort.13
The studies not reporting an association between FH and subclinical atherosclerosis are often those screening individuals in their early 50s.19 ,23 We importantly refined our analysis by ferreting younger FH subsets that may not require additional CAD screening. In the current series, we identified a pattern where younger FH patients did not benefit from improved mortality reclassification with CAC. Prior American College of Cardiology/American Heart Association guidelines indicate a potential benefit for screening men ≥40 and women ≥55 years of age.5 Our data support that this stated threshold may be too young and encourage CAC screening where no clinical benefit may be observed in younger FH patients. Data support that screening of patients with a FH who are older and with a greater cumulative risk factor burden may improve the accuracy of CAC for estimating long-term mortality risk. In a related example from the Dallas Heart Study, a FH of myocardial infarction and the prevalence of CAD were not statistically significant in young subjects.12 Similarly, in our younger FH cohort, the AUC was similar for the FRS when compared with CAC score findings (p=0.674).
Limitations
Studies have indicated improved prognostic value with more complex FH scales24 and our binary FH variable may underestimate its utility in risk assessment. Prior research does support simple categorisation FH, employed herein, as prognostically informative.2 The availability of cause of death and other end points may have altered our prognostic findings, although misclassification related to causality is problematic. Data from this single site reflect a common referral pattern and inclusion of multiple centres would enhance the generalisability of our presented findings.
Conclusion
In this registry of 9715 patients, CAC effectively risk-stratified patients with and without a FH of premature CAD. However, for younger and lower-risk FH cohorts, CAC screening did not provide additive prognostic information beyond that of the traditional cardiac risk factors. Based on this single-site series, screening strategies should consider excluding younger and lower-risk FH cohorts.
Key messages
What is already known on this subject?
Although coronary artery calcium (CAC) scoring effectively risk stratifies across varied patient cohorts, the evidence is less developed for individuals with a family history of coronary artery disease (CAD). As patients with a family history of CAD have an increased risk of developing CAD, many may be referred for CAC scoring to better estimate their risk.
What might this study add?
In this large (>9000 patients) cohort, CAC scoring effectively stratified long-term (median follow-up 14.7 years) mortality risk in patients with and without a family history of CAD. However, for younger and lower-risk patients with a family history of CAD, CAC scoring did not provide additional prognostic information beyond that of traditional risk scoring systems.
How might this impact on clinical practice?
While current guidelines support the use of CAC scoring in low-risk subsets of patients with a family history of CAD, the results of this study argue that CAC screening does not provide additional mortality risk information for younger patients with a family history of CAD.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
Contributors All authors have contributed significantly to the manuscript. JTK's (first authors) particular contribution was in the drafting of the initial manuscript and its subsequent revisions.
Funding This registry was performed without any funding from equipment or pharmaceutical manufacturers.
Competing interests JKM has served on the medical advisory boards of GE Healthcare, Arineta, Astra Zeneca and Bristol-Myers Squibb; Speakers’ Bureau of GE Healthcare; received research support from GE Healthcare, Vital Images and Phillips Healthcare and serves as a consultant to Astra Zeneca and HeartFlow.
Ethics approval Emory University Institutional Review Board.
Provenance and peer review Not commissioned; externally peer reviewed.