Article Text

Abstract
Objective Our objective is to gain a better understanding of the efficacy and safety of therapeutic hypothermia (TH) in patients with acute ST elevation myocardial infarction (STEMI) through an analysis of randomised controlled trials (RCTs).
Background Several RCTs have suggested a positive outcome with the use of TH in the prevention of myocardial injury in the setting of an acute STEMI. However, there are currently no clinical trials that have conclusively shown any significant benefit.
Methods Electronic databases were used to identify RCTs of TH in the patient population with STEMI. The primary efficacy end point was major adverse cardiovascular event (MACE). Secondary efficacy end points included all-cause mortality, infarct size, new myocardial infarction and heart failure/pulmonary oedema (HF/PO). All-bleeding, ventricular arrhythmias and bradycardias were recorded as the safety end points.
Results Six RCTs were included in this meta-analysis, enrolling a total of 819 patients. There was no significant benefit from TH in preventing MACE (OR, 01.04; 95% CI 0.37 to 2.89), all-cause mortality (OR, 1.48; 95% CI 0.68 to 3.19), new myocardial infarction (OR, 0.99; 95% CI 0.20 to 4.94), HF/PO (OR, 0.52; 95% CI 0.15 to 1.77) or infarct size (standard difference of the mean (SDM), −0.1; 95% CI −0.23 to 0.04). However, a significant reduction of infarct size was observed with TH utilisation in anterior wall myocardial infarction (SDM, −0.23; 95% CI −0.45 to −0.02). There was no significant difference seen for the safety end points all-bleeding (OR 1.32; 95% CI 0.77 to 2.24), ventricular arrhythmias (OR, 0.85; 95% CI 0.54 to 1.36) or bradycardias (OR, 1.16; 95% CI 0.74 to 1.83).
Conclusions Although TH appears to be safe in patients with STEMI, meta-analysis of published RCTs indicates that benefit is limited to reduction of infarct size in patients with anterior wall involvement with no demonstrable effect on all-cause mortality, recurrent myocardial infarction or HF/PO.
Statistics from Altmetric.com
Introduction
To reduce the complications associated with ST segment elevation myocardial infarction (STEMI), early reperfusion remains the mainstay for myocardial salvage either with thrombolytics or percutaneous coronary intervention (PCI).1 ,2 However, despite these contemporary reperfusion therapies, many patients continue to suffer myocardial tissue damage and go on to develop typical STEMI sequelae.3
Therapeutic hypothermia (TH) has been shown to offer neurological benefits in patients who have had a cardiac arrest, corroborating its establishment as a standard therapeutic intervention.4 It has been postulated that the mechanisms of TH involved in neuroprotection may also contribute to the protection of ischaemic myocardium.5 Several clinical trials have investigated the impact of inhospital TH in the STEMI population, yet it has failed to reduce complications. Nevertheless, the case series and randomised controlled trials (RCTs) that have been carried out to investigate the role of TH in the STEMI population were underpowered and consequently, incapable of drawing firm conclusions of this intervention.
Therefore, we performed a systematic review and meta-analysis of RCTs to assess the efficacy and safety of TH in patients with STEMI.
Methods
Search strategy
We conducted a literature search of PubMed CENTRAL, EMBASE, The Cochrane Central Register of Controlled Trials, ClinicalTrials.gov, Google Scholar databases, the scientific session abstracts in Circulation, Journal of the American College of Cardiology, European Heart Journal and American Journal of Cardiology from 1 January 1990 to 30 June 2015. Oral presentations and/or expert slide presentations were included by using TCT (http://www.tctmd.com), EuroPCR (http://www.europcr.com), ACC (http://www.acc.org), AHA (http://www.aha.org) and ESC (http://www.escardio.org). We also performed manual searches of the reference lists of studies, reviews, editorials and letters, as well as related conference proceedings.
Search term keywords included: hypothermia, therapeutic hypothermia, mild hypothermia protocol, cardiac arrest, cardiogenic shock, acute myocardial infarction, myocardial infarction, randomised controlled trials. Only adult human trials were included.
Inclusion criteria
The PRISMA statement for reporting systematic reviews and meta-analyses of RCTs was applied to the method of this study.
Included studies met the following specifications: (1) RCT design (2) evaluation of patients with STEMI (age >18 years old) (3) TH administered in the setting of acute STEMI (4) studies that provided outcome data on major adverse cardiovascular events (MACEs), infarct size and/or mortality.
Exclusion criteria were patients who were non-STEMI, unstable angina, and chronic ischaemic heart disease or did not meet the above-mentioned criteria.
Two reviewers (PAV and DFB) independently extracted data from identified RCTs. Disagreements were resolved by consensus or if necessary, by a third party.
Study end points
The primary efficacy end point was MACE. The definition of MACE differed across studies; trial-specific definitions of MACE were used. Secondary efficacy end points included all-cause mortality, new myocardial infarction, heart failure/pulmonary oedema (HF/PO), and infarct size. For infarct size, we performed a subgroup analysis based on the location of the STEMI, dividing the patient population as those who experienced either anterior or non-anterior wall myocardial infarction. Safety end points were all-bleeding, ventricular tachycardia and/or ventricular fibrillation, and bradycardias.
Statistical analysis
Data were summarised across treatment arms using the one-step (Peto) OR for dichotomous data and standardised difference in mean (SDM) for continuous data with fixed-effects models. We evaluated heterogeneity of effects with the I2 statistic. In cases of heterogeneity (I2 >40%), a random-effects model was used. To address publication bias, we used four methods: funnel plots, Begg-Mazumdar test, Egger test, and Duval and Tweedie’s test. Sensitivity analyses were performed using the one-study-out method, chronological cumulative analyses and random-effects model. The statistical analysis was performed by the Comprehensive Meta-analysis V.2.0 software (Biostat, New Jersey, USA). Two authors independently assessed the risk of bias using standard criteria defined in the Cochrane Handbook for Systematic Reviews of Interventions.
Results
Study selection and characteristics
Our search strategy identified a total of 785 articles (see online supplementary figure S1). After removing duplicates and articles not meeting inclusion criteria, we screened 132 titles and abstracts. Of these, 14 were selected for further review of eligibility. Finally, six RCTs satisfied inclusion criteria, all of which were published in English.6–11 Baseline characteristics of studies are presented in tables 1 and 2. The final six RCTs enrolled a total of 819 patients. Included trials compared intervention groups that were treated with standard STEMI guideline-based therapy and TH versus those treated with standard STEMI guideline-based therapy alone. All but the Prospective, Multicenter, Randomised, Controlled Pilot Trial of Peritoneal Hypothermia in Patients With ST Segment Elevation Myocardial Infarction (VELOCITY)11 used endovascular catheter cooling to achieve hypothermia, with variable cooling times ranging from 1 h to 6 h. Infarct size was assessed using cardiac MRI (CMR) in half of the studies. The other half of the studies used nuclear tomographic imaging with technetium sestamibi single photon emission CT (SPECT). All studies reported outcomes at 30 days except for the Intravascular Cooling Adjunctive to Percutaneous Coronary Intervention (ICE-IT)8 and Efficacy of Endovascular Catheter Cooling Combined with Cold Saline for the Treatment of Acute Myocardial Infarction (CHILL-MI)10 trials. These two trials instead followed up to 1 year and 45 days, respectively.
Baseline characteristics of studies investigating the efficacy of TH
Design of studies investigating the efficacy of TH
Quantitative data synthesis
Primary end point
A total of 58 MACEs was observed for the primary efficacy end point with no significant difference between the TH group (7.5% (31/410 patients)) versus the control group (6.6% (27/409 patients)) (OR, 01.04; 95% CI 0.37 to 2.89). There was no MACE in either group in the Rapid Intravascular Cooling in Myocardial Infarction as Adjunctive to Percutaneous Coronary Intervention study (RAPID MI-ICE).9 There were a total of 27 deaths reported in all patients that suffered a STEMI: 3.9% (16/410 patients) in the TH group and 2.6% (11/409 patients) in the control group; neither CHILL-MI10 nor RAPID MI-ICE9 had fatal events. There was no significant difference in all-cause mortality between the two groups (OR, 1.48; 95% CI 0.68 to 3.19). There was no difference in new myocardial infarction (OR, 0.99; 95% CI 0.20 to 4.94) and HF/PO (OR, 0.52; 95% CI 0.15 to 1.77) between the TH and the control arms (figure 1). A total of 6 new myocardial infarctions were reported; 1% (3/296 patients) in the TH group and 1% in the control group (3/295 patients); and 31 new HF/PO cases were reported, 3.7% in the TH group (11/296 patients) and 6.7% (20/295 patients) in the control arm. Neither Dixon6 nor RAPID MI-ICE9 had new myocardial infarctions in either groups and ICE-IT8 did not report the data for recurrent myocardial infarction and HF/PO.

Forest plot of the OR of MACE, all-cause mortality, new myocardial infarction and heart failure between patients with STEMI treated with therapeutic hypothermia compared with the control group. Diamond indicates overall summary estimate for the analysis (width of the diamond represents 95% CI, width of the shaded square indicates population size). MACE, major adverse cardiovascular events; STEMI, ST elevation myocardial infarction.
No difference was observed overall in infarct size (SDM, −0.1; 95% CI −0.23 to 0.04) between the groups. However, in the subgroup analysis for infarct size, there was a significant difference favouring hypothermia for anterior wall myocardial infarction (SDM, -0.23; 95% CI -0.45 to −0.02) as compared with non-anterior wall myocardial infarction (SDM, −0.18; 95% CI -0.44 to 0.09); see figure 2. Only four trials7 ,8 ,10 ,11 provided information for anterior wall STEMI and three trials8 ,10 ,11 for non-anterior wall STEMI.
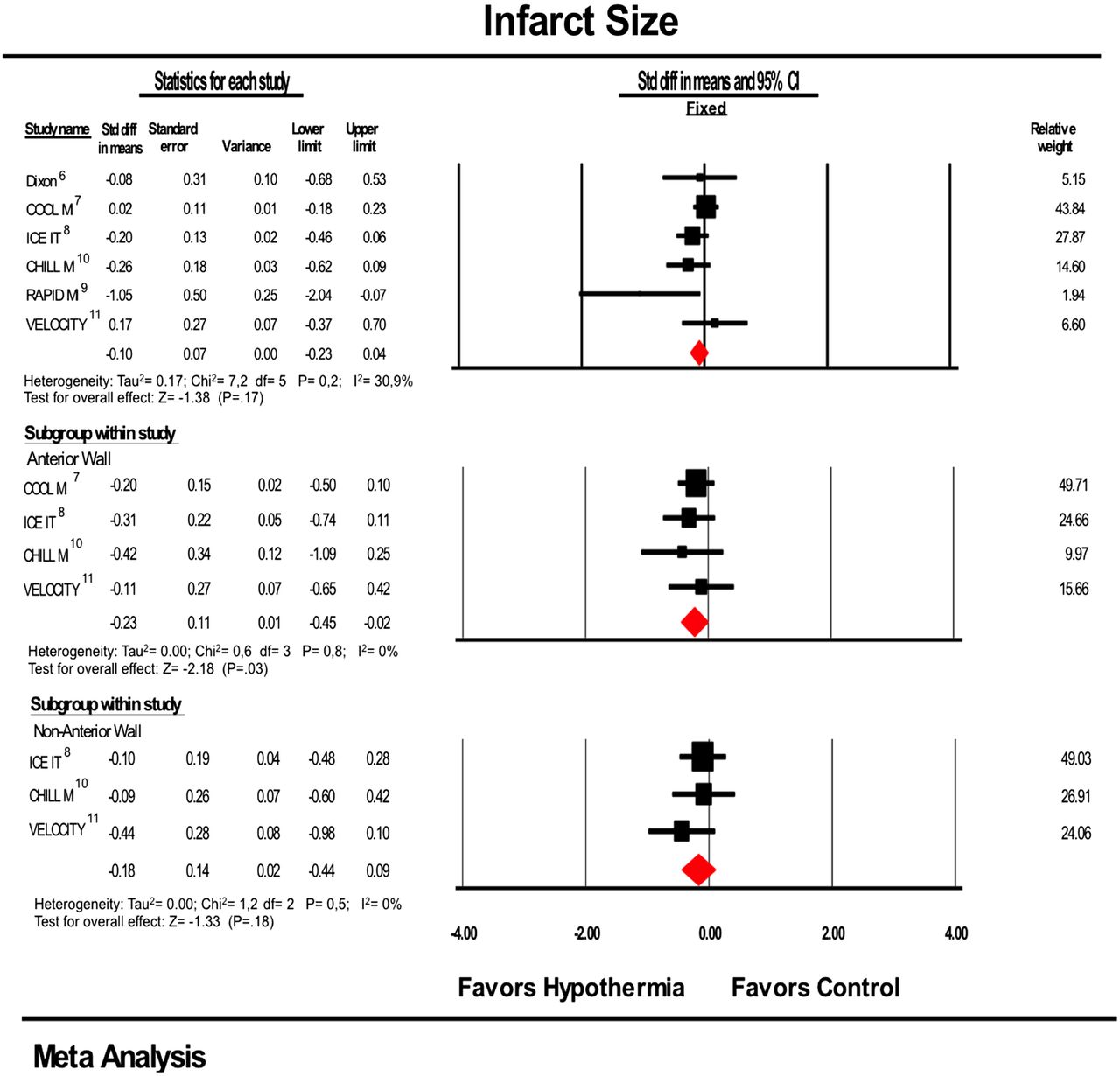
Forest plot of the standardised difference in mean of infarct size including subgroups (anterior wall and non-anterior wall STEMI) between patients with STEMI treated with therapeutic hypothermia compared with the control group. Diamond indicates overall summary estimate for the analysis (width of the diamond represents 95% CI, width of the shaded square indicates population size). STEMI, ST elevation myocardial infarction.
Safety end points
Among trials reporting ventricular arrhythmias, a total of 86 events were observed. No significant difference in events was observed (OR, 0.85; 95% CI 0.54 to 1.36) between the TH group 13.5% (40/296 patients) and the control group 15.5% (46/295 patients); ICE-IT8 did not report the data for ventricular arrhythmias. No significant difference was observed (OR, 1.16; 95% CI 0.74 to 1.83) for bradycardias between the TH group 19% (51/268 patients) and the control group 17.1% (46/269 patients). No events were observed in the RAPID MI-ICE9 trial and neither ICE-IT8 nor VELOCITY11 reported the measured outcome. A similar result was observed for all-bleeding events between TH and control groups (OR, 1.32; 95% CI 0.77 to 2.24). A total of 65 bleeding events were observed, 11.3% in the TH group (36/317 patients) and 9.1% in the control group (29/316 patients); see figure 3. No bleeding events were observed in RAPID MI-ICE9 and ICE-IT8 did not report the measured outcome.

{kind=link}
{kind=link}
{kind=link}
Forest plot of the OR of ventricular arrhythmias, bradycardia and all-bleeding between patients with STEMI treated with therapeutic hypothermia compared with control group using. Diamond indicates overall summary estimate for the analysis (width of the diamond represents 95% CI, width of the shaded square indicates population size). STEMI, ST elevation myocardial infarction.
Sensitivity analysis
Sensitivity analysis whereby each RCT was removed individually did not demonstrate significant difference or change in the overall efficacy and safety outcomes, except in the analyses of HF/PO and infarct size. When the COOL-MI, Cooling as an Adjunctive Therapy to Percutaneous Intervention in Patients with Acute Myocardial Infarction (COOL-MI)7 trial was removed for the HF/PO outcome, a significant effect favouring the use of TH was observed (OR, 0.29; 95% CI 0.11 to 0.77). The same change in summary effect favouring TH was observed when the COOL-MI7 was removed for the outcome infarct size (SDM, −19; 95% CI −0.37 to −0.01). For anterior wall myocardial infarction infarct size, the final effect becomes insignificant if one of the following studies is removed: COOL-MI, ICE-IT, CHILL-MI7 ,8 ,10 (see online supplementary figure S2). Chronological cumulative analysis for each outcome did not find a significant change in the overall final effect outcomes, except for infarct size for anterior wall myocardial infarction, where the effect summary becomes significant with CHILL-MI10 (see online supplementary figure S3).
Bias
Funnel plot analysis did not show bias for all outcomes except for all-cause mortality, ventricular arrhythmias, bradycardias and HF/PO (see online supplementary figure S4). However, after quantifying the observed bias with others methods (Begg-Mazumdar, Egger, and Duval and Tweedie’s test) there was no evidence of publication bias (see online supplementary figure S5). The individual study quality appraisal and the risk of bias for the six included RCTs are summarised in the online supplementary table S1.
Discussion
Our meta-analysis is designed to evaluate the efficacy of TH in reducing infarct size, MACE, new myocardial infarctions and all-cause mortality in patient populations with STEMI that have been included in randomised studies. To our knowledge, this is the first meta-analysis that examines this patient population and provides a comprehensive review of RCTs available to date. The pooled analysis of RCTs included in this meta-analysis did not show a reduction in MACE, all-cause mortality, HF/PO, new myocardial infarctions and infarct size when compared with control. However, the use of TH did show benefit when used to treat anterior wall STEMI. Similar to prior studies, our results also suggest that TH is a safe intervention as there was no significant difference between both groups with regards to adverse effect outcomes.12
These results indicate that the same benefits of TH observed in early RCTs in patients with cardiac arrest13 ,14 are not applicable to the STEMI population. However they concur with the conclusions of a recent large randomised study in patients with cardiac arrest where no benefit was seen among survivors exposed to TH.15 It is unclear why these results are observed; it is possible that the neutral effect of this therapy extends to the patient population with STEMI and more research is needed before any conclusions can be made.
Several putative explanations may be invoked as to why TH has not been shown to be effective in the management of acute STEMI. Earlier RCTs investigating TH as an adjunct therapy in patients with STEMI used partial cooling of patients prior to reperfusion. As suggested by the post hoc analysis of RAPID MI-ICE9 and ICE-IT trials,8 an important determinant of significant reduction of infarct size after hypothermia was seen when cooling temperature reached ≤35°C. This was achieved in only a minority of patients.17 Patients who did not achieve the target cooling temperature did not show a significant reduction in infarct size. Based on this finding, the CHILL-MI trial10 was undertaken and showed that even in patients randomised to hypothermia that achieved the target temperature (76% reached ≤35°C while 91% reached ≤35.4°C) no significant difference was observed in infarct size when compared with the control group. Though the target temperature was not achieved by all subjects, subgroup analysis of the selected studies suggests that the target temperature should be <35°C and above 32°C to avoid potential adverse reactions of the intervention.
TH may have a more robust effect based on infarct location. The COOL-MI7 trial showed no difference between the two groups with respect to the primary end point of left ventricular infarct size at 30 days by SPECT imaging (13.8% control group vs 14.1% hypothermic group, p=0.83). However, most patients did not reach the target temperature (≤35°C). In patients with an anterior myocardial infarction who did reach the target temperature, there was a significant reduction in infarct size by SPECT imaging. Like the COOL-MI,10 the ICE-IT8 trial also showed a trend towards significant reduction of infarct size in the subgroup of patients with an anterior myocardial infarction who were cooled adequately, despite the fact that both trials are negative for the overall primary outcomes. The later CHILL-MI trial also found a 33% significant reduction of infarct size in the anterior STEMI subgroup. The pooled analysis of the RCTs in this meta-analysis supports the favourable effects of TH in patients with anterior wall involvement. A possible explanation may be that anterior wall infarctions are larger and more consistent in size, and mixing anterior and non-anterior infarcts without determination of myocardium at risk entails more variability and consequently substantial SD in infarct size. To properly answer this inquiry, larger and more powered studies are needed to detect a significant difference. This finding should not be surprising because in small uncomplicated inferior myocardial infarction, the benefit of thrombolytics too is unclear, while in larger anterior or complicated inferior myocardial infarction the benefits are clear.18
Cardioprotective strategies in TH may additionally be dependent on ischaemic time or duration of symptoms prior to reperfusion. Longer periods of ischaemia may lead to larger transmural infarction than do shorter periods of ischaemia. Animal studies correlate shorter ischaemic duration (<45 min) with reduced infarct size in rats exposed to hypothermic intervention after coronary occlusion.19 All the RCTs included to date in this meta-analysis included patients with ischaemia time of less than 6 h in order to optimise the efficacy of cardioprotective therapy. Additionally, in a pooled analysis patients with less than a 4-h duration of ischaemia prior to cooling from the CHILL-MI10 and ICE-IT8trials, showed a trend towards benefit in this population (p=0.15).17
It is important to note that hypothermia is not without complications. Despite the observed benefits of TH in out-of-hospital cardiac arrest in earlier trials,13 ,20 the physiological changes in the circulatory and metabolic systems caused by hypothermia can cause harm.21 Therapeutic cooling to core temperatures of 32–34°C results in shivering, which can be uncomfortable for awake, non-sedated patients and increases systemic oxygen consumption which in turn can perpetuate the cycle of ischaemia.22 In addition, therapeutic cooling also increases platelet activation, which directly contributes to thrombosis23 and may attenuate the efficacy of ADP antagonists,24 ,25 as seen in the VELOCITY11 trial where an increased rate of stent thrombosis was observed in patients who received TH. These potential adverse effects must be taken into consideration along with the potential benefits of TH.
TH entails important financial implications as well. A cost-effectiveness analysis of its use in out-of-hospital cardiac arrest showed an incremental cost of $31 254 compared with those treated conventionally.26
Future hypothermia trials in STEMI should investigate its utility in patients with anterior wall involvement. The rationale for this is based on current meta-analysis results, and because it well known that patients with anterior wall myocardial infarction demonstrate a lower left ventricular ejection fraction compared with patients with inferior infarction, even after adjustment for infarct size. These patients have a higher incidence of congestive heart failure, cardiogenic shock and cumulative cardiac mortality.27 ,28 Trials should also focus on quality, timing and duration of cooling to achieve the target temperature. Currently, the optimal method of cooling has not been determined, however an RCT in patients with cardiac arrest suggest that endovascular cooling maintains target temperatures better than conventional surface cooling methods, with less temperature fluctuation and fewer complications.29 Perhaps, the combinations of prehospital cooling, cold saline and more powerful cooling devices will allow more rapid lowering of core temperature even before reperfusion takes place, thereby optimising cooling time. With improved rapid cooling, TH may have a more pronounced impact as an adjunctive therapy for STEMI to reduce infarct size in addition to the incidence of adverse outcomes.
Limitations
Our meta-analysis has several potential limitations. First, this is a meta-analysis performed on study-level data. Second, there was no standardisation among the trials regarding study design, treatment exposure and target temperature or specific outcomes. The studies included different cooling catheters to achieve temperature goals. In addition, all the patients in the hypothermia arms did not reach the target temperature; such underdosing may have underestimated the full benefit of TH. Third, the definition of MACE differed across studies, depending on trial-specific definitions. It was consistently used as an end point across trials, thus part of our composite analysis, but the heterogeneity in its interpretation poses limitations on conclusions. Fourth, different imaging modalities (CMR vs SPECT) were used to assess infarct size. The varying sensitivities of these modalities are potential confounders that may have affected the results of this end point. Lastly, given the small number of RCTs that have evaluated the efficacy of TH, our sample size is still limited for analysis.
Conclusions
Our meta-analysis is consistent with the available, yet limited evidence to support the use of TH in the STEMI population undergoing primary PCI. The main benefit of its use was seen in the reduction of infarct size in patients with anterior wall myocardial infarction.
Key messages
What is already known on this subject?
Therapeutic hypothermia (TH) has been shown to offer neurological benefits in patients who have had a cardiac arrest. The impact of TH in the ST elevation myocardial infarction (STEMI) population failed to show a significant reduction in infarct size and associated complications; however the randomised controlled trials (RCTs) were underpowered to draw conclusions.
What might this study add?
We performed a comprehensive systematic review and meta-analysis of RCTs to assess the efficacy and safety of TH in patients with STEMI. A significant benefit of this therapy was the reduction of infarct size in patients with anterior wall involvement (p =0.03). Although a safe modality, there was no effect on all-cause mortality, new myocardial infarction or heart failure/pulmonary oedema.
How might this impact on clinical practice?
These findings will drive the need for further investigation into the optimal use for this therapeutic option to improve outcome after a STEMI. The need to verify these findings and to assess possible long-term clinical benefit and harms with an adequately powered RCT limited to patients with anterior wall myocardial infarction presents itself.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
Contributors All the authors have made substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; and drafting the work or revising it critically for important intellectual content; final approval of the version to be published; and agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.