Article Text

Abstract
Objectives: To determine whether case fatality rates in South Asian (Bangladeshi, Indian and Pakistani) patients with acute myocardial infarction have shown similar declines to those reported for white patients during the past 15 years.
Design: Cross-sectional, observational study.
Setting: Coronary care unit in east London.
Patients: 2640 patients—29% South Asian—admitted with acute myocardial infarction between January 1988 and December 2002.
Main outcome measures: Differences over time in rates of in-hospital death, ventricular fibrillation and left ventricular failure.
Results: The proportion of South Asians increased from 22% in 1988–92 to 37% in 1998–2002. Indices of infarct severity were similar in South Asian and white patients, with declining frequencies of ST elevation infarction (88.2% to 77.5%, p < 0.0001), Q wave development (78.1% to 56.9%, p < 0.0001) and mean (interquartile range) peak serum creatine kinase concentrations (1250 (567–2078) to 1007 (538–1758) IU/l, p < 0.0001) between 1988–92 and 1998–2002. Rates of in-hospital death (13.0% to 9.4%, p < 0.01), ventricular fibrillation (9.2% to 6.0%, p < 0.001) and left ventricular failure (33.2% to 26.5%, p < 0.0001) all declined; these changes did not interact significantly with ethnicity. Odds ratios for the effect of time on risk of death increased from 0.81 (95% CI 0.70 to 0.93) to 1.02 (95% CI 0.87 to 1.21) after adjustment for ethnicity and indices of infarct severity (ST elevation, peak creatine kinase, Q wave development and treatment with a thrombolytic).
Conclusions: In the past 15 years, death from acute myocardial infarction among South Asians has declined at a rate similar to that seen in white patients. This is largely caused by reductions in indices of infarct severity.
- acute myocardial infarction
- South Asians
- ethnicity
- mortality
Statistics from Altmetric.com
In the past two decades most Western countries have seen steep declines in mortality for coronary heart disease.1,2 These have been accompanied by better outcomes after acute myocardial infarction that were particularly notable in the late 1980s as thrombolytic drugs were introduced into clinical practice.3,4 Since then, a continuing decline in the incidence and case fatality rates for acute coronary heart disease has been attributed to the effects of reperfusion therapy and secondary prevention strategies combining to limit infarct severity and protect against further plaque events.1,5
Certain subgroups have not seen such favourable trends and for South Asians (Bangladeshi, Indian and Pakistani), in particular, mortality from coronary heart disease has shown little tendency to fall, in contrast to nearly all other ethnic groups.6,7 We have previously reported increased case fatality rates for South Asian patients with acute myocardial infarction, related, at least in part, to their propensity to diabetes.8 More South Asian patients are now presenting with acute coronary syndromes but it is not known whether they are experiencing declines in infarct mortality similar to those seen among white patients. In the present study we attempt to answer this question by reference to a clinical database of admissions to an inner city coronary care unit over a 15 year period.
METHODS
Patient population
We studied 2640 consecutive patients with acute myocardial infarction admitted to a single centre coronary care unit over a 15 year period, between January 1988 and December 2002. The same creatine kinase (CK) based definition of acute myocardial infarction was applied throughout the study to ensure that the risk characteristics of the study population over time were not influenced by a change in the troponin based definition. Any two of the following three criteria were applied: typical chest pain; > 0.1 mV ST elevation in at least one standard or two precordial leads; and a rise in serum CK to > 400 IU/l (the upper limit of the reference range being 200 IU/l).
South Asian patients were predominantly of Bangladeshi, Indian or Pakistani origin. Analysis of the records of all coronary care unit admissions of patients with acute coronary syndromes during 2002 showed that 38% (196 of 521) were South Asian, of whom 27% were Bangladeshi, 37% Indian and 34% Pakistani. This approximates well to the proportion of South Asians (33%) living in the catchment area of the hospital at the time (UK population census 2001).
Data collection
Clinical details were recorded prospectively and stored on an electronic database for subsequent analysis. The number of fields within the database increased substantially during the study period and, except where indicated, only those available for the full 15 years were analysed. These were demographic characteristics, risk factors, admission drugs, emergency treatment, ECG changes (ST change, Q wave development), biochemical analysis on admission and CK release. The principal end point of the study was in-hospital death, and secondary outcomes recorded were ventricular fibrillation and left ventricular failure.
Statistical analysis
For categorical data, trends in characteristics over time were tested by using logistic regression models with year fitted as a continuous variable. For continuous data results are presented as median and interquartile range, and the Spearman rank correlation was used to assess the trend. Patients were divided into four ethnic groups: white, South Asian, Afro-Caribbean and “other”. Only the white and South Asian groups contained sufficient numbers of patients to allow statistical analyses to be performed and the 85 patients coded Afro-Caribbean and “other” were excluded. Clinical outcomes were compared in three time periods by the χ2 test and then trends over time were tested by fitting a continuous variable. Year was divided by five so that the corresponding odds ratio represented the change in risk over a period of five years. Continuous variables (except age and time trend) were fitted as quintiles due to non-normality. The significance level was taken as 5%. The odds ratio for the trend was then compared after adjustment for various combinations of risk factors. As the odds ratio approached 1.0 the covariates were seen to be explaining the trend in outcome.
The local ethics committee approved the study protocol and the study was done in compliance with the Declaration of Helsinki.
RESULTS
Clinical characteristics and ethnicity
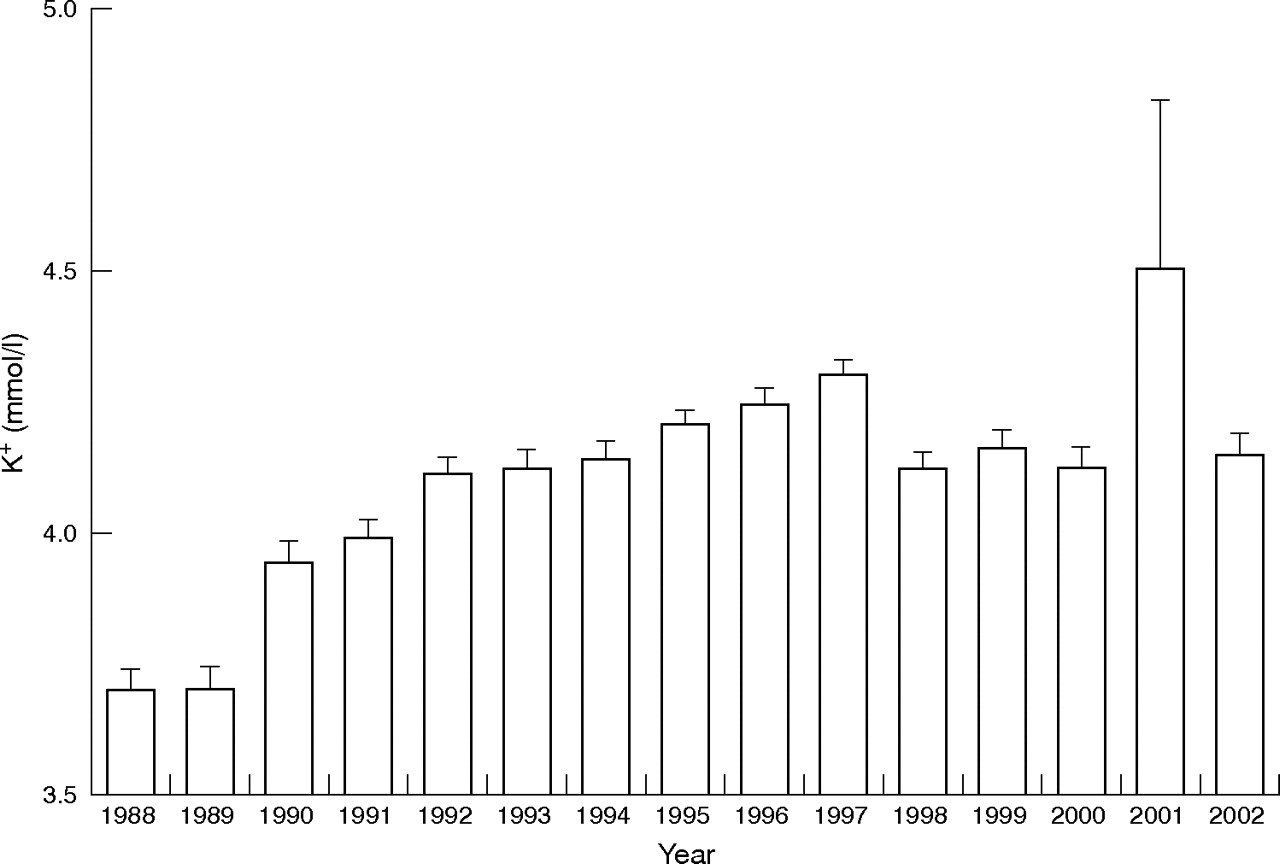
Ethnic profiles changed significantly during the study, the proportion of whites declining as the proportion of South Asians (Bangladeshi, Indian and Pakistani) increased from 22% in 1988–92 to 37% in 1998–2002 (table 1). South Asians were younger than white patients and more of them were men, but in both groups age tended to increase during the 15 year study period. A higher proportion of South Asians had diabetes and fewer smoked compared with white patients, but only among white patients did smoking rates decline during the study. In both groups, rates of hypertension were comparable and tended to increase. Admission serum potassium concentrations were comparable in South Asian and white patients but increased significantly during the study period (fig 1).
Baseline characteristics of South Asian and white patients with acute myocardial infarction

{kind=link}
Admission serum potassium concentrations in all patients by year. Data are presented as mean (SE).
Infarct severity
The frequency of ST elevation infarcts declined progressively during the study period, and this was associated with diminishing use of thrombolytics while door to needle times improved (table 1). A decline in the frequency of Q wave development was also observed and CK release diminished. Comparison of South Asian with white patients showed no significant differences in ECG indices of infarct severity, although CK release tended to be higher in South Asians.
Clinical outcomes
The rate of in-hospital death declined by 27.7% over the 15 year study period, from 13.0% in 1988–92 to 9.4% in 1998–2002 (table 2). With age adjustment, this improvement in survival was similar for South Asian and white patients, there being no significant interaction of ethnicity with the declining rate of in-hospital death during the 15 year study period. Rates of ventricular fibrillation and left ventricular failure also declined but ethnicity also did not interact with the declining rates of these major complications. Logistic regression analysis of the changing risk over the five year terciles (table 3) showed that decreasing indices of infarct severity largely explained the decline in mortality. Thus, the odds ratios for the effect of time on risk of death increased from 0.81 (95% confidence interval 0.70 to 0.93, p = 0.004) to 1.02 (95% confidence interval 0.87 to 1.21, p = 0.79) after adjustment for ST elevation, peak CK, Q wave development and treatment with a thrombolytic (plus ethnicity). Adjustment for serum potassium concentration, in addition to the above factors, effectively abolished the significance of the odds ratio for the effect of time on ventricular fibrillation but not on left ventricular failure.
Clinical outcomes of South Asian and white patients with acute myocardial infarction
Odds ratios (95% confidence intervals) for effect of a five year time change on ventricular fibrillation, left ventricular failure and death
DISCUSSION
This was a cross-sectional outcome study of patients with acute myocardial infarction treated in an inner city coronary care unit over a 15 year period. During this time there was a large increase in the proportion of South Asian (Bangladeshi, Indian and Pakistani) patients, who are usually considered to be at heightened cardiovascular risk.6,9 Nevertheless, the study showed that rates of all major complications have been in progressive decline, with in-hospital mortality now 27.7% lower than it was 15 years ago. Importantly, this improvement in clinical outcome was observed in both South Asian and white patients.
The increasing proportion of South Asians with acute myocardial infarction over the past 15 years—now accounting for 37% of all admissions—reflects the timing of the major immigration waves during the 1960s and 1970s and the accelerated atherogenesis to which this group is prone, myocardial infarction being particularly prevalent in young Asian men.10,11 Not only is myocardial infarction more prevalent in South Asians but outcomes are often worse, with diabetes explaining much of the excess mortality.8 Thus, the incidence of diabetes, and with it hypertension, among our patients with acute myocardial infarction has risen in approximate parallel to the proportion of South Asian patients. Despite these potentially unfavourable changes in the risk characteristics and ethnic mix of our infarct population, we found that the decline in mortality during the 15 years of data collection was similar to those reported by other investigators3,5 and, importantly, these declines were shared by both South Asian and white patients.
A major finding of this study was that the severity of infarction, as reflected by Q wave development and CK release, was similar in South Asian and white patients and declined over the years—almost certainly driven by the faster delivery of thrombolytic treatment plus an increasing frequency of non-ST elevation myocardial infarction. The proportion of patients with previous infarction also decreased sharply, further contributing to reductions in myocardial injury. Whereas faster delivery of thrombolytic treatment has been a leading target of health care in recent years,12 changes in the frequency of non-ST elevation myocardial infarction are harder to explain. Contributory factors may have included reductions in cigarette smoking and increasing pretreatment with aspirin during the study, both of which have been associated with favourable effects on thrombogenicity and ST change.13,14 Similar lifestyle and treatment effects are central to secondary prevention strategies and were probably responsible for the diminishing proportion of patients with previous infarction. The combination of less frequent previous infarction and more benign modes of presentation, despite increasing rates of diabetes, hypertension and Asian ethnicity, provides the most plausible explanation for the reductions in myocardial injury and progressive improvement in outcomes observed in South Asian and white patients during the study. Our study has provided the first direct confirmation of this explanation by showing that adjustment for indices of infarct severity effectively abolished the effect of time on changes in mortality.
In addition to the substantial mortality reductions that occurred during the 15 year study period, reductions in left ventricular failure and ventricular fibrillation were quantitatively similar. The risk of left ventricular failure, like in-hospital mortality, is largely determined by the extent of myocardial injury. Its declining frequency presumably partly reflected less severe modes of presentation, although the logistic regression analysis suggested that other explanatory factors, not recorded in this study, must also have played a part. The risk of ventricular fibrillation is influenced importantly by the admission serum potassium concentration, which increased progressively during the observation period. This may reflect the diminishing severity of infarction (reduced sympathoadrenal activation reduces sodium–potassium exchange across the cell membrane15) but also the increasing proportion of patients with diabetes in whom potassium concentrations are usually well maintained in the acute phase of myocardial infarction.16 The logistic regression analysis confirmed the importance of the changes in potassium concentrations in reducing over time the frequency of ventricular fibrillation.
Ethnicity was documented within our data collection as long ago as 1988, at a time when most data collections specifically excluded any ethnic reference. Only recently in the United Kingdom have the national groups (Bangladeshi, Indian and Pakistani) that constitute South Asian ethnicity been recorded. There is no evidence of substantial differences in case fatality rates for acute myocardial infarction between these groups. It must be recognised, however, that our study is unable to confirm this and our conclusion of declining case fatality rates for South Asians with acute myocardial infarction does not preclude such differences. It is also pertinent to consider the external validity of findings from a single centre, although its inner-city location was an advantage in allowing the question of ethnicity in relation to outcome to be addressed, without confounding by variable, centre-specific management protocols. The central finding of diminishing infarct severity and complication rates for acute myocardial infarction in recent years agrees with other large studies that have examined this issue,17,18 suggesting that our findings with regard to South Asian patients are robust and externally valid.
In conclusion, this study confirms a progressive improvement in outcomes for patients with acute myocardial infarction over a 15 year period starting in 1988. Importantly, we have shown that the improvement in outcomes for patients of South Asian origin has been as good as that for white patients. Reductions in the severity of infarction that were recorded during the study largely explain the observed declining case fatality rates.
REFERENCES
Footnotes
-
Published Online First 30 December 2005
-
Funding: none
-
Competing interests: none declared